ODONTOGENIC CYSTS What are they Cysts are PATHOLOGICAL

















 Odontogenic Cysts- An overview. Dental Update 2015; 42: 548")

- Slides: 20
ODONTOGENIC CYSTS
What are they? Cysts are PATHOLOGICAL EPITHELIAL LINED cavities. Contains fluid or semi-fluid. Odontogenic means originating in tooth or surrounding tissues. Arising from epithelial remnants of tooth. DEVELOPMENTAL OR INFLAMMATORY.
How do you detect them? Usually asymptomatic. (slow growth so structures move out way when growing i. e ian. If altered sensation etc then may be indication of more aggressive pathology!!) Findings are mostly incidental on radiograph. Can create clinical swelling. Thinning of bone due to growth can result in ‘egg shell cracking’ (pathogenesis of development and expansion debated)
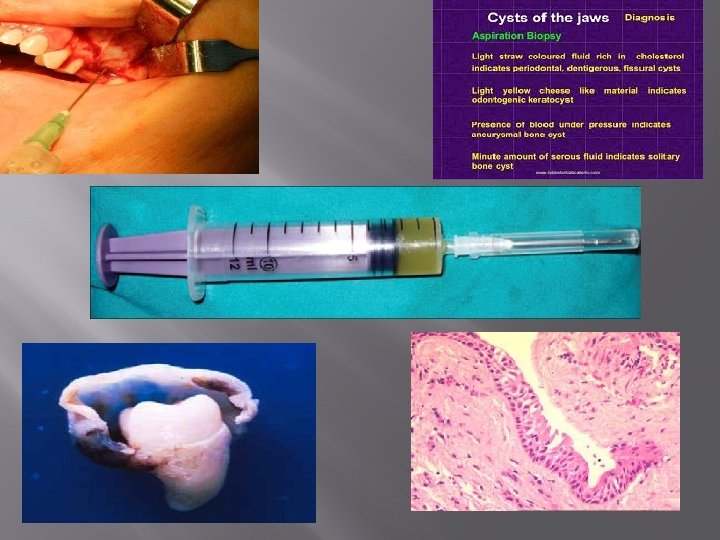
Then What? ? A radiolucency on radiograph can confirm cyst like structure. BUT Diagnosis still required. Keep in mind could also be odontogenic tumour such as ameloblastoma or osteolytic lesion such as metastatic cancer. � SO Things such as sensibility testing, cbct, biopsy of cyst lining and aspiration of cyst contents all help with diagnosis.
Radicular cyst MOST COMMON 60% of odontogenic cysts -Inflammatory type cyst - 60% maxilla compared to 40% mandible (poss due to increase of trauma in maxilla) - associated with NON-VITAL tooth. -Pt may c/o- pain from area and +/- sinus. - cyst developed by chronic inflammation following pulpal necrosis. � Round / ovoid radiolucency with radio-opaque margin extending from lamina dura. Histopathology shows these cysts lined with stratified squamous epithelium which may have mucous or cillated cells, with deposits of cholesterol a common find
Radicular cont � Lining arises from rest cells of malassez in perio lig which are stimulated by endotoxins and inflammatory cytokines. Theory is that the epithelium surrounds a granuloma and as this grows, granuloma becomes necrotic and liquefies. Can’t tell difference between cyst, granuloma or abscess radiographically. TREATMENT = RCT or Extraction of tooth (if large cyst may require enucleation)
Residual cyst 10% of Odontogenic cysts. Radicular cysts which remains after removal of tooth. � Similar features therefore to radicular (obvs now with no tooth involved) � Histologically has less inflammatory features (source of irritation has been removed) � TREATMENT= marsupialisation or enucleation �
Dentigerous cyst 18 -24% of Odontogenic cysts. � Enclose crown of UNERUPTED, usually impacted, tooth such as 3 rd molars/maxillary canines by expansion of its follicle. (fluid accumulation between enamel of tooth and the reduced enamel epithelium) � Affect males> females, commonly in 3 rd decade. � 3 variations : central (crown in centre), lateral (follicle dilated and doesn't completely enclose crown), circumferential (appears that whole tooth covered but still occurring from amelo-cemental junction). � �
Dentigerous cont Attached to tooth at amelo-cemental junction. Well circumscribed, unilocular radiolucency. with well-defined sclerotic margins associated to crown or tooth. May cause resorption of adjacent teeth roots. Histologically the lining is a thin regular layer 2 -5 cells thick of thick non-keratinised stratified squamous OR flattened cuboidal epithelium which resembles the reduced enamel epithelium. Cyst contains proteinaceous, yellowish fluid and cholesterol crystals. TREATMENT = Removal of tooth then enucleation of cyst lining or marsupialisation / enucleation of cyst but leave tooth to allow eruption.
Eruption cyst � � � 22% of cysts in paediatric pts but less than 1% in adult population. (usually 1 st perm molar) � Cyst related to unerupted tooth. but rather than developing around tooth, develops within soft tissues overlying tooth. Presents as soft fluctuant swelling on gingivae. Either gingival coloured or blue/purple. No bony involvement.
Eruption cont No radiograph taken usually but if it was there would be radiolucent lesion at alveolar margin. Pathogenesis similar to dentigerous cysts in way that epithelium believed to be derived form reduced enamel epithelium. Histology shows 2 -3 layers of squamous epithelium resembling reduced enamel epithelium. Lining usually inflammed. TREATMENT= most burst spontaneously but marsupialisation can be undertaken
Lateral perio cyst Less than 1% of odontogenic cysts. Form in lateral perio position. Inflammatory in nature. Develop at any age but most common 40 -70 yrs & both gender equally affected. Most common areas are mandibular premolar and anterior maxilla. Occasionally blue fluctuant swelling present adjacent to vital tooth. Unsure of origin of epithelial lining.
Lateral perio cyst cont Present between cervical margin of tooth and the apex. Round or oval in shape with sclerotic margin. Histologically, unicystic or multicystic are commonly lined with thick, non-keratinized layer of squamous or cuboidal epithelium, usually 1 -5 cell layers thick. TREATMENT = Enucleation of the lesion while maintaining the adjacent tooth however the tooth may need extracted.
Keratocystic odontogenic tumour Previously known as keratocyst but due to neoplastic nature change req. � Peak incidence in 2 nd-3 rd decades and most commonly occur in males. 65 -83% occur in mandible (half of these at angle) � Multiple tumours can be associated with naevoid basal cell carcinoma syndrome. � Lesions are developmental arising from either dental lamina or extension of basal cells from overlying epithelium. These are usually destructive cysts as can grown large within mandible. Recurrence rate 50 -60%. Due to satellite cysts (left behind due to thin lining) �
Keratocystic odontogenic tumour cont Radiographically may appear small round or ovoid unilocular or may be larger with scalloped margins. Lesions well demarcated with distinct sclerotic margins. Multi-locular lesions can also occur. Adjacent teeth may displace but rarely root resorption. Histopathology cyst lined with regular keratinised stratified squamous epithelium with 5 -8 cell layers thick. No rete ridges. Well defined basal layer is intensely basophillic. Mitotic figures present. TREATMENT= En-block resection
Enucleation = COMPLETE removal of cyst. Marsupialisation = Creation of window in wall opf cyst to decompress. Left open and then eventually once shrunk, can enucleate the remainder of cyst. Choose this if enucleation would risk damaging surrounding structures/ risk of #. En-block = removal of cyst + surrounding bone.
Summary
References Nayyer, N V. (2015) Odontogenic Cysts- An overview. Dental Update 2015; 42: 548 -555 https: //www. youtube. com/user/Dr. Sandra. Lee
Any Questions?