BIOMEDICAL WASTE DISPOSAL PRESENTED BY CHRISTEENA JOSEPH 2

BIOMEDICAL WASTE DISPOSAL PRESENTED BY CHRISTEENA JOSEPH 2 ND YEAR PG

CONTENTS � INTRODUCTION � DEFINITION � SOURCES OF BIOMEDICAL WASTE � INFECTIONS ASSOCIATED WITH BIOMEDICAL WASTE � BIOMEDICAL WASTE DISPOSAL FLOW CHART � CATEGORIES OF BIOMEDICAL WASTE SCHEDULE AS PER WHO STANDARDS

� COLOR CODING FOR SEGREGATION OF BIOMEDICAL WASTE � MANAGEMENT OF BIOMEDICAL WASTE � WASTE MANGEMENT IN DENTAL OFFICES � PACKAGING AND STORAGE OF BIOMEDICAL WASTE � BIOMEDICAL WASTE DISPOSAL METHODS � CONCLUSION

INTRODUCTION � In todays upgrowing society the disease rates are cosiderably high. Their is an increase in demand of new trends in disease management and health care sectors. � The biomedical waste managment is an alarming issue world wide � BMW-threat for man, community and environment.

� Safe and scientific methods of biomedical waste management and disposal is an important problem to be solved.

WASTE Wastes Solid waste Household waste Industrial waste Biomedical waste or hospital waste Liquid Waste Gaseous Waste

DEFINITION � BIOMEDICAL WASTE ? � Acc to bio medical waste rules , 1998 of India“ bio-medical waste” means any waste which is generated during the diagnosis, treatment or immunization of human beings or animals or in research activities pertaining there to or in the production or testing of bio medicals. environmental management in health care facilities-Kathryn D. Wagner

� Any unwanted residual material which cannot be discharged directly, or after suitable treatment can be discharged in the atmosphere or to a receiving water source, or used for landfill is waste. (Wilson, 1981) environmental management in health care facilities-Kathryn D. Wagner

WASTE MANAGEMENT � Waste Management is collection, transport, processing, recycling , disposal of waste material. This term usually relates to materials produced by human activity and is generally undertaken to reduce effect on health, the environment. � Practice of waste management may differ in developing nation to under developing nation, urban to rural area and residential to industrial setup. environmental management in health care facilities-Kathryn D. Wagner

HEALTH WASTE CHARACTERIZATION NON RISK WASTE HEALTHCARE WASTE RISK WASTE environmental management in health care facilities-Kathryn D. Wagner

BIOMEDICAL WASTE SHARPS 1% RADIOACTIVE , CYTOTOXIC WASTE PATHOLOGICA L AND INFECTIOUS WASTE, 15% NON INFECTEOUS WASTE 80 % environmental management in health care facilities-Kathryn D. Wagner

SOURCES OF BIOMEDICAL WASTE MAJOR SOURCES Hospitals labs Research centres Animal research Blood banks Nursing homes Mortuaries Autopsy centres MINOR SOURCES Community medicine with recent advances-AH Suryakantha Clinics Dental clinics Home care Cosmetic clinics Paramedics Funeral services institutions

COMPONENTS Human anatomical waste EXAMPLES Tissues, organs, body parts Animal waste Generated during research/experimentation, from veterinary hospitals Microbiology and biotechnology waste Waste sharps Liquid waste Laboratory cultures, microorganisms, human and animal cell cultures, toxins hypodermic needles, syringes, scalpels, broken glass Generated from any of the infected areas Community medicine with recent advances-AH Suryakantha

§Soiled waste § Chemical waste §Discarded medicines and cyto-toxic drugs §Radioactive Components §Incineration ash Dressing, bandages, plaster casts, material contaminated with blood Alcohol, Sulphuric acid, chlorine powder, Glutaraldehyde, Picric acid, fertiliser, ammonia Barium enema, X-rays, Cancer chemotherapy, tar-based products Radioactive components Community medicine with recent advances-AH Suryakantha

� RISK WASTES › › › › infectious waste Genotoxic waste Chemical waste Waste with heavy metal contents Pressurized containers Sharps Pharmaceutical waste Pathological waste Community medicine with recent advances-AH Suryakantha

� At risk Sanitation workers Medical and paramedic al workers Patients and attenders public

HAZARDOUS HEALTH CARE WASTE CAN RESULT IN � INFECTION � GENOTOXICITY AND CYTOTOXICITY � CHEMICAL TOXICITY � RADIOACTIVE HAZARDS � PHYSICAL INJURIES � PUBLIC SENSITIVITY Community medicine with recent advances-AH Suryakantha

INFECTION � The infectious agents enter the body through § § § Puncture Abrasion Cut in the skin Through mucous membranes By inhalations and ingestions control of hospital infections a practical book – Gajayliffe, A. P. Fraise

Most common infections � � � 1. Gastro enteric through faeces and/or vomit e. g. Salmonella, Vibrio Cholera, Helminthes Hepatitis A 2. Respiratory through inhaled secretions e. g. Mycobacterium tuberculosis; measles virus; streptococcus pneumonae 3. Ocular infections through eye secretions e. g. Herpes virus, 4. Skin infection through pus e. g. Streptococcus 5. Meningitis through Cerebrospinal fluid e. g. neisseria meningitides, control of hospital infections a practical book – Gajayliffe, A. P. Fraise

� Blood borne diseases • AIDS • Septicaemia and bacteraemia • Viral Hepatitis B & C � 7. Hemorrhagic fevers through body fluids • Lassa, Ebola and Marburg viruses control of hospital infections a practical book – Gajayliffe, A. P. Fraise

PROBLEMS ASSOCIATED WITH BIOMEDICAL WASTE ORGANISMS DISEASE CAUSED VIRUSES HIV, hepatitis A, hepatitis B, Hepatitis A, C, Enteroviruses AIDS, INFECTIOUS HEPATITIS, DENGUE, TI CK- BORNE FEVER RELATED WASTE ITEM INFECTED NEEDLES. BODY FLUIDS, HUMAN EXCRETA, BLOOD , BODY FLUIDS BACTERIA SALMNELLA TYPHI, VIBRIO CHOLERAE, CLOSTRIDIU M TETANI, PSUEDOMONAS, STREPTOCOCCUS Typhoid, Cholera, Tetanus Wound infections, septicemia, rheumatic fever, endocarditis, skin and soft tissue infections Human excreta and body fluid in landfills and hospital wards, Sharps such as needles, surgical blades in hospital waste. PARASITES Wucheraria Bancrofti, Plasmodium Cutaneous leishmaniasis, Kala Azar, Malaria Human excreta, blood and body fluids in poorly managed sewage system of hospitals.

GENOTOXICITY AND CYTOTOXICITY Irritant to skin and eyes � E. g. alkylating agent, intercalating agent • Carcinogenic and Mutagenic � e. g. Secondary neoplasia due to chemotherapy • Application of treatment and disposal methods-Int. J. Environ. Res. Public Health 2015 , 6818 -6831

CHEMICAL TOXICITY Many drugs are hazardous • May cause intoxication , burns, poisoning on exposure • Application of treatment and disposal methods-Int. J. Environ. Res. Public Health 2015 , 6818 -6831

RADIOACTIVE HAZARDS � Radioactive waste exposure may cause headache, dizziness, vomiting and tissue damage Application of treatment and disposal methods-Int. J. Environ. Res. Public Health 2015 , 6818 -6831

PHYSICAL INJURIES � Sharps � Chemical � Explosive agents �PUBLIC SENSITIVITY Visual impact of the anatomical waste, recognizable body parts Application of treatment and disposal methods-Int. J. Environ. Res. Public Health 2015 , 6818 -6831

WASTE WITH HIGH CONTENT OF HEAVY METALS § § Waste with high content of heavy metals Batteries Broken thermometers Blood pressure guages etc Application of treatment and disposal methods-Int. J. Environ. Res. Public Health 2015 , 6818 -6831

HEAVY METAL CONTENT WASTE

PRESSURISED CONTAINERS AEROSOLS GAS CATRIDGES GAS CYLINDERS

SHARP WASTES § § § Needles Infusion Sets Scalpels Knives Blades Broken Glass Application of treatment and disposal methods-Int. J. Environ. Res. Public Health 2015 , 6818 -6831

PHARMACUETICAL WASTE • • • Expired Pharmaceuticals Contaminated Pharmaceuticals Banned Pharmaceuticals Application of treatment and disposal methods-Int. J. Environ. Res. Public Health 2015 , 6818 -6831


PATHOLOGICAL WASTE • • Excreta Human tissues/fluids Body parts Blood or body fluids Application of treatment and disposal methods-Int. J. Environ. Res. Public Health 2015 , 6818 -6831

HOSPITAL WASTE DISPOSED

LIQUID WASTE Liquid pathological and chemical waste should be appropriately treated before discharge into the sewer. Pathological waste must be treated with chemical disinfectants, neutralized and then flushed into the sewage system. � Chemical waste must be neutralized with appropriate reagents and then flushed into the sewer system. This method requires highly qualified technicians for operation of the process and uses hazardous substances that require comprehensive safety measures � Biomedical Waste Management A Step Towards A Healthy Future. KAMLESH TEWARY.

The effluent generated from the hospital should conform to the following limits: Parameters Permissible limits p. H 6. 5 -9. 0 Suspended solids 100 mg/l Oil and grease 10 mg/l Bio-assay test 90% survival of fish after 96 hours in 100% effluent � These limits are applicable to those hospitals, which are either connected with sewers without terminal sewage treatment plant or not connected to public sewers. � Biomedical Waste Management A Step Towards A Healthy Future. KAMLESH TEWARY.


WASTE IN DENTAL OFFICES � BLOOD � SHARPS � ANATOMICAL WASTE � PATHOLOGICAL WASTE � DENTAL AMALGAMS � X –RAYS AND DEVELOPERS � CONTAMINATED LAUNDRY infection control and management of hazardous materials for dental team-Chris H. Miller

BLOOD � Blood mixed with saliva and other fluids evacuated in the dental office as waste water system. � Rinse sink traps and evacuation lines daily with disinfected solution � Carefully pour blood, suction fluids into the drain connected to the sewer system(meeting local regulatory guidelines)in an acceptable method infection control and management of hazardous materials for dental team-Chris H. Miller

PATHOGENIC WASTE Teeth and other tissues � Potentially infectious teeth disposal should be in a color labeled container (many areas allow in house neutralization of such items) � Disposal of treated tooth and other tissue are as to the local guidelines � Pathologic waste is hidden from public and its disposal is secured and receptable. infection control and management of hazardous materials for dental team-Chris H. Miller

DENTAL AMALGAM � Amalgam restored teeth can be disinfected before disposal with sterilizing chemical for 30 minutes and should rinse treated teeth well. Teeth with amalgam restoration must not be heat sterilized to avoid the possibility of mercury vapor release during the sterilization procedure. � Extracted teeth should not ordinarily be returned to patients, however, the new guideline allows extracted teeth to be returned to the patient. It should be soaked first in sodium hypochlorite for 10 minutes before returning to the patient. infection control and management of hazardous materials for dental team-Chris H. Miller

Do use precapsulated alloys and stock a variety of capsule sizes Do recycle used disposable amalgam capsules Do salvage, store and recycle non-contact amalgam (scrap amalgam) Do salvage (contact) amalgam pieces from restorations after removal and recycle the amalgam waste Do use chair-side traps, vacuum pump filters and amalgam separators to retain amalgam and recycle their contents. Do recycle teeth that contain amalgam restorations. Do manage amalgam waste through recycling as much as possible Don’t use bulk mercury Don’t put used disposable amalgam capsules in biohazard containers, infectious waste containers (red bags) or regular garbage. Don’t put non-contact amalgam waste in biohazard containers, infectious waste containers (red bags) or regular garbage Don’t put contact amalgam waste in biohazard containers, infectious waste containers (red bags) or regular garbage Don’t rinse devices containing amalgam over drains or sinks Don’t dispose of extracted teeth that contain amalgam restorations in biohazard containers, infectious waste containers (red bags), sharps containers or regular garbage Don’t flush amalgam waste down the drain or toilet

X RAY AND DEVELOPER � Separate fixer and developer solutions in the container provided by the approved waste carrier and supplier. � Label the container. � Once the container is full contact appropriate waste carrier for disposal. infection control and management of hazardous materials for dental team-Chris H. Miller

Analysis of Information, Impact and Control of HIV amongst Dental Professionals of Central India Jatin Agarwal et al Journal of Clinical and Diagnostic Research. 2015 Jul, Vol-9(7): ZC 80 -ZC 84 Aim: To obtain comprehensive information about the HIV related information, its impact on the health care provider’s attitude towards treating patients living with HIV/AIDS (PLWHA), infection control & waste disposal practices among dental professionals of Malwa region of Madhya Pradesh; situated in Central India. � Materials and Methods: A cross-sectional survey was conducted among 320 private dental practitioners. Data was collected using a pretested, self administered 40 item questionnaire and statistically analysed. �

� Results: The response rate was 81. 25%. Over all 50. 76% dentists were graded as having good knowledge of HIV. Unfortunately, their willingness to treat these patients remained low. Junior dentists expressed less hesitation with regard to acceptance of risk patients than other dentists. Over 65% of the respondents reported adherence to universal precautions. The most alarming observation was that dentists were not following safe waste management practices.
 In house segregation (collection, segregation and packaging in")
BIOMEDICAL WASTE FLOW CHART GENERATOR (hospitals) In house segregation (collection, segregation and packaging in color coded poly bags) Common storage points in hospitals Transpotation (approved special vehicle Unloading and storage Disposal (recycling and landfill) treatment (incineration, autocla ving and shreding environmental management in health care facilities-Kathryn D. Wagner

Categories of biomedical waste schedule as per WHO standards WASTE CATEGORY TYPE OF WASTE TREATMENT AND DISPOSAL OPTION Category No. Human Anatomical Waste (Human tissues, organs, body Incineration@ / deep 1 parts) burial* Animal Waste (Animal tissues, organs, body parts, carcasses, bleeding Category No. Incineration@ / deep parts, fluid, blood and experimental animals used in 2 burial* research, waste generated by veterinary hospitals and colleges, discharge from hospitals, animal houses) Microbiology & Biotechnology Waste (Wastes from laboratory cultures, stocks or specimen of live micro organisms or attenuated vaccines, human and animal cell Category No. cultures used in research and infectious agents from 3 research and industrial laboratories, wastes from production of biologicals, toxins and devices used for transfer of cultures) Community medicine with recent advances-AH Suryakantha Local autoclaving/ microwaving / incineration@

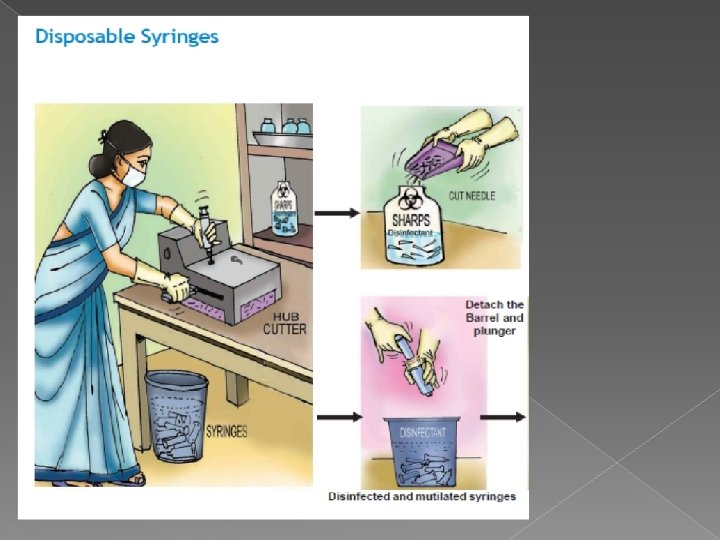
Waste Sharps (Needles, syringes, Disinfecting (chemical Category No. scalpels, blades, glass, etc. that may treatment@@ / autoclaving / 4 cause puncture and cuts. This includes microwaving and mutilation / both used and unused sharps) shredding Category No. 5 Discarded Medicine and Cytotoxic drugs Incineration@ / destruction (Wastes comprising of outdated, and drugs disposal in contaminated and discarded medicines) secured landfills Soiled Waste (Items contaminated with Category No. body fluids including cotton, dressings, Incineration@ / autoclaving / 6 soiled plaster casts, lines, bedding and microwaving other materials contaminated with blood. ) Category No. 7 Solid Waste (Waste generated from Disinfecting by chemical disposable items other than the waste treatment@@ / autoclaving / sharps such as tubing, catheters, microwaving and mutilation / intravenous sets, etc. ) shredding# #

Category No. 8 Liquid Waste (Waste generated from Disinfecting by chemical the laboratory and washing, cleaning, treatment@@ and discharge house keeping and disinfecting into drains activities) Category No. 9 Incineration Ash (Ash from Disposal in municipal landfill incineration of any biomedical waste) Category No. 10 Chemical Waste (Chemicals used in Chemical treatment @@ production of biologicals, chemicals and discharge into drains for used in disinfecting, as insecticides, liquids and secured landfill etc. ) for solids. Community medicine with recent advances-AH Suryakantha

COL OR WASTE Yellow Human & Animal anatomical waste / Micro-biology waste and soiled cotton/dressings/linen/beddings etc. Incineration / Deep burial Tubings, Catheters, IV sets. Autoclaving / Microwaving / Chemical treatment Blue / Blue White Waste sharps ( Needles, Syringes, Scalpels, blades etc. ) Autoclaving / Microwaving / Chemical treatment & Destruction / Shredding Black Discarded medicines/cytotoxic Disposal in secured drugs, landfill Incineration ash, Chemical waste. Red TREATMENT

MANAGEMENT OF BIOMEDICAL WASTE Survey of waste generated. 2. Segregation of hospital waste. 3. Collection & Categorization of waste. 4. Storage of waste. ( Not beyond 48 hrs. ) 5. Transportation of waste. 6. Treatment of waste. 1. Community medicine with recent advances-AH Suryakantha

SOURCE REDUCTION � SOURCE REDUCTION-ways to lessen the amount of material. � Segregation-keeping non infectious waste out of the infectious water stream. � Minimization-reduce or eliminate waste at the source. � Engineering controls- methods to reduce quantity of waste. environmental management in health care facilities-Kathryn D. Wagner

STEPS TO MANAGE HAZARDOUS WASTES BEFORE DISPOSAL 1. Know what hazards you have 2. Purchase smallest quantity needed, and don’t purchase hazardous materials if safe alternative exists. USE MERCURY FREE THERMOMETRE guidelines for safe disposal of unwanted pharmacueticals in and after emergencies-who 1991, Tim grayling

� 3. Limit use and access to trained persons with personal protective gear guidelines for safe disposal of unwanted pharmacueticals in and after emergencies-who 1991, Tim grayling

4. GET RID OF UNNECESSARY STUFFS � Don’t accumulate unneeded products � Don’t let peroxides and oxidising agents turn into bombs guidelines for safe disposal of unwanted pharmacueticals in and after emergencies-who 1991, Tim grayling

LABEL OF HAZARD WARNINGS

6. COMMUNICATE ABOUT THE WORK HAZARDS � Job description � Posters on doors � Labels on hazards � Give feedback on use of PPE and disposal in evaluation � Role model safe use and disposal 7. RECYCLE PRODUCTS WHICH ARE POSSIBLE guidelines for safe disposal of unwanted pharmacueticals in and after emergencies-who 1991, Tim grayling

SEGREGATION OF WASTE � At the point of generation. � In a color coded leak proof container. � Container should bear ‘BIOHAZARD SYMBOL’ and appropiate wordings. � Container should never be completely filled. Community medicine with recent advances-AH Suryakantha

� Segregation of waste should be monitored strictly because, Once the waste are mixed it becomes infectious. so avoid mixing of non infectious waste and infectiouswaste � To reduce the infectious waste � To decrease the expenditure on disposing infectious waste. Community medicine with recent advances-AH Suryakantha

SEGREGATION OF SOLID BIOMEDICAL WASTE

WASTE REQUIRING PRETREATMENT BEFORE DISPOSAL � MICROBIOLOGICAL WASTE �Autoclaving �Final disposal as general waste-red bag Community medicine with recent advances-AH Suryakantha

WASTE Tubes used for serum separation, centrifugation of samples, preparation of dilutions etc. � sample cups , Tips , Caps. � � � Any other contaminated plastic wares � � � Method: Chemical Disinfection Sodium hypochlorite Final Disposal- Blue bag Community medicine with recent advances-AH Suryakantha

� Frequency of changing of Na hypochlorite solution-Daily Technical person. A trained housekeeping person can do preparation under observation. � Disposal of liquid and solid � � Liquid: Pour into drain with running tap � - Solid: Blue bag Community medicine with recent advances-AH Suryakantha

� Wastes comprising of out dated, contaminated and discarded medicines, solid chemicals used for disinfection in Lab & Hospitals as insecticides- black bag Community medicine with recent advances-AH Suryakantha

Waste disposed without pretreatment Yellow bag � Contaminated gloves; latex & plastic(Uncontaminated – general waste) � Contaminated tissue /blotting papers � Contaminated cotton � Human tissue/organs White - sharp disposal container � Broken glass, pipettes, broken test tubes, � Needles, razor blade, scalpel Community medicine with recent advances-AH Suryakantha

Packaging and labeling � Bags 3/4 th filled should be tied, � be supervised Name of Ward, � Date of Packaging, � Destination (Treatment Site) � Bio Hazard/Cytotoxic Symbol � Weighing & Recording � Separate Register and Weighing Machine � Daily recording is mandatory Community medicine with recent advances-AH Suryakantha
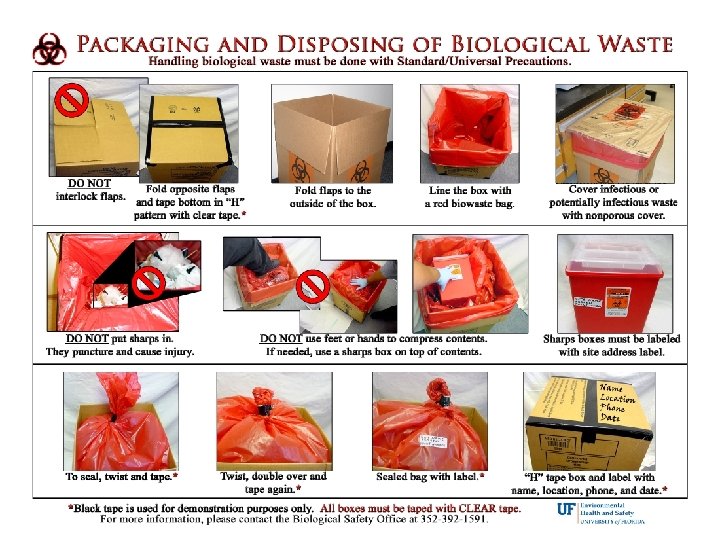

Collection, transpotation and storage Waste collected and stored in thick noncorrosive disposable plastic bags or containers of specific colour code. � The waste in bags or containers should be stored in a separate area, room, or building of a size appropriate to the quantities of waste produced and the frequency of collection. � Health care waste should be transported within the hospital or other facility by means of hand cart wheeled trolley. � Community medicine with recent advances-AH Suryakantha

TRANSPOTATION � Transportation of BMW can be divided into internal and external transportation. � INTERNAL: it is for yellow , red , blue and white bags. � EXTERNAL: it is for the general waste collected in the black coloured plastic bags. Community medicine with recent advances-AH Suryakantha

SAFE TRANSPORTATION

Safe transportation of biomedical waste in a health care institution. Kumar A, Duggal S, Gur R, Rongpharpi SR, Sagar S, Rani M, Dhayal D, Khanijo CM. Indian J Med Microbiol. 2015 Jul-Sep; 33(3): 383 -6 � INTRODUCTION: � The chances of health care waste (Biomedical waste) coming in contact with the health care workers, patients, visitors, sanitary workers, waste handlers, public, rag pickers and animals during transportation are high. � MATERIALS AND METHODS: � The study was conducted over a period of seven months (April 2013 -October 2013) in a 500 -bedded hospital where the average quantum of biomedical waste is 0. 8 kg/bed/day. The issues related to transportation of health care waste from 39 generation sites to the health care waste storage site inside the hospital (intramural transfer) were addressed analysed in a predesigned proforma.

RESULTS: The biomedical waste management team inspected the generation sites in the hospital on a daily basis and conformance to the procedures was checked. It was found that waste was collected at scheduled timings in 99. 6% occasions; however, compliance to wearing personal protective equipment (PPE) was poor and ranged from 1. 22 -1. 84%. � CONCLUSION: � Transportation of health care waste is a crucial step in its management. Regular training program for all the sections of health care workers with special emphasis on waste handlers is needed � �

BIOSPILL-KIT � � � Container of undiluted household bleach Several pairs of gloves Safety glasses Absorbent material Biohazardous waste (autoclave) bags Dust pan & scoop or tongs for broken glass

DISPOSAL METHOD OF BIOMEDICAL WASTE � � � � � Incineration Chemical disinfection Inertisation Autoclave Encapsulation Microwave hydroclave Shredder Plasma pyrolysis Deep burial

INCINERATION Medical waste incineration involves the burning of wastes produced by hospitals, veterinary facilities, and medical research facilities. � These wastes include both infectious ("red bag") medical wastes as well as non-infectious, general housekeeping wastes. � The emission factors presented here represent emissions when both types of these wastes are combusted rather than just infectious wastes. �

THREE TYPES OF INCINERATED COMMONLY USED � Controlled air. � Excess air incinerator. � - Rotary kiln.
")
Controlled-Air Incinerators � Controlled-air incineration is the most widely used medical waste incinerator (MWI) � technology, and now dominates the market for new systems at hospitals and similar medical facilities. � Waste feed capacities for controlled air incinerators range from about 0. 6 to 50 kg/min (75 to 6, 500 lb/hr) (at an assumed fuel heating value of 19, 700 k. J/kg

2 STAGES In the first stage, waste is fed into the primary, or lower, combustion chamber, which is operated with less than the required amount of air required for combustion. � Combustion air enters the primary chamber from beneath the incinerator hearth (below the burning bed of waste). � This air is called primary or underfire air. In the primary (starved-air) chamber, the low air-to-fuel ratio dries and facilitates volatilization of the waste, and most of the residual carbon in the ash burns. � �

� At these conditions, combustion gas temperatures are relatively low (760 to 980°C [1, 400 to 1, 800°F]). In the second stage, excess air is added to the volatile gases formed in the primary chamber to complete combustion. � Secondary chamber temperatures are higher than primary chamber temperatures--typically 980 to 1, 095°C (1, 800 to 2, 000°F). � � Depending on the heating value and moisture content of the waste, additional heat may be needed. This can be provided by auxiliary burners located at the entrance to the secondary (upper) chamber to maintain desired temperatures

� Excess air incinerators are typically a compact cube with a series of internal chambers and baffles. � Although they can be operated continuously, they are usually operated in a batch mode. waste is manually fed into the combustion chamber. � The charging door is then closed, and an afterburner is ignited to bring these condary chamber to a target temperature (typically 870 to 980°C [1600 to 1800°F]).

� When the target temperature is reached, the primary chamber burner ignites. The waste is dried, ignited, and combusted by heat provided by the primary chamber burner, as well as by radiant heat from the chamber walls � Moisture and volatile components in the waste are vaporized, and pass (along with combustion gases) out of the primary chamber and through a flame port which connects the primary chamber to the secondary or mixing chamber.

Secondary air is added through the flame port and is mixed with the volatile components in the secondary chamber. Burners are also installed in the secondary chamber to maintain adequate temperatures for combustion of volatile gases. � Gases exiting the secondary chamber are directed to the incinerator stack or to an air pollution control device. � When the waste is consumed, the primary burner shuts off. Typically, the afterburner shuts off after a set time. Once the chamber cools, ash is manually removed from the primary chamber floor and a new charge of waste can be added. �

� Waste feed capacities for excess air incinerators are usually 3. 8 kg/min (500 lb/hr) or Less Rotary Kiln Incinerators � Rotary kiln incinerators, like the other types, are designed with a primary chamber, where the waste is heated and volatilized, and a secondary chamber, where combustion of the volatile fraction is completed. The primary chamber consists of a slightly inclined, rotating kiln in which waste materials migrate from the feed end to the ash discharge end. � The waste rate is controlled by adjusting the rate of kiln rotation and the angle of inclination. Combustion air enters the primary chamber through a port. � An auxiliary burner is generally used to start combustion and maintain desired combustion temperatures.

Both the primary and secondary chambers are usually lined with acid-resistant refractory brick The secondary chamber operates at excess air. Combustion of the volatiles is completed in these condary chamber. � Due to the turbulent motion of the waste in the primary chamber, solids burnout rates and particulate entrainment in the fuel gas are higher for rotary kiln incinerators than for other incinerator designs. � As a result, rotary kiln incinerators generally have add-on gas cleaning devices. �

INCINERATOR ASH DISPOSAL

CHEMICAL DEGRADATION Chemical degradation methods, which convert cytotoxic compounds into non-toxic/nongenotoxic compounds, can be used not only for drug residues but also for cleaning of contaminated urinals, spillages, and protective clothing. � The methods are appropriate for developing countries. Most of these methods are relatively simple and safe; � they include oxidation by potassium permanganate (KMn. O 4) or sulfuricacid (H 2 SO 4), denitrosation by hydrobromic acid (HBr), or reductionby nickel and aluminium. � Application of treatmet and disposal methods-Int. J. Environ. Res. Public Health 2015 , 6818 -6831

� The methods are not appropriate for the treatment of contaminated body fluids. � It should be noted that neither incineration nor chemical degradation currently provides a completely satisfactory solution for the treatment of waste, spillages, or biological fluids contaminated by antineoplastic agents. � Until such a solution is available, hospitals should use the utmost care in the use and handling of cytotoxic drugs. Application of treatmet and disposal methods-Int. J. Environ. Res. Public Health 2015 , 6818 -6831

Cytotoxic drugs for which chemical degradation methods exist � Carmustine, Doxorubicin, Semustine � Chlorambucil , fosfamide, Spiromustine � Chlormethine, Lomustine, Streptozocin � Chlorozotocin , Melphalan , 6 -Thioguanine � Cisplatin, 6 -Mercaptopurine, Uramustine � Cyclophosphamide , Methotrexate , Vincristine sulfate � Daunorubicin, PCNUa, Vinblastine sulfate � Dichloromethotrexate , Procarbazine � Application of treatmet and disposal methods-Int. J. Environ. Res. Public Health 2015 , 6818 -6831

CHEMICAL DISINFECTION In this method chemicals are added to waste to kill or inactivate the pathogens. this method is most suitable for treating liquid waste. � Solid and highly hazardous waste can also be disinfected chemically with limitations; � Shredding or milling of waste is required before disinfection � Power disinfections are required which are themselves hazardous and should be used by trained professionals. � Essentials of public health dentistry-soben peter

� Only surface of intact solid waste will be disinfected � Types of disinfections; � Formaldehyde � Ethylene oxide � Glutaraldelhyde � Sodium hypochlorite � Chlorine dioxide Essentials of public health dentistry-soben peter

INERTIZATION The process of inertization involves mixing waste with cement and other substances before disposal, in order to minimize the risk of toxic substances contained in the wastes migrating into the surface water or ground water. � A typical proportion of the mixture is: 65 percent pharmaceutical waste, 15 percent cement and 5 percent water. � A homogenous mass is formed and cubes or pellets are produced on site and then transported to suitable storage sites. It is relatively inexpensive and not applicable to infectious waste. � Textbook of Medicine update – Kamlesh tewary.

AUTOCLAVE The autoclave should be dedicated for the purposes of disinfecting and treating bio-medical waste. � When operating a gravity flow autoclave, medical waste is subjected to: i. A temperature of not less than 121ºC and pressure of 15 pounds per square inch (psi) for an autoclave residence time of not less than 60 minutes; or ii. A temperature of not less than 135ºC and pressure of 31 psi for an autoclave residence time of not less than 45 minutes; or � Textbook of Medicine update – Kamlesh tewary.

iii. A temperature of not less than 149ºC and a pressure of 52 psi for an autoclave residence time of not less than 30 minutes. � When operating a vacuum autoclave, medical waste is first subjected to a minimum of one pre -vacuum autoclave to purge the autoclave of all air. The waste is then subjected to the following: i. A temperature of not less than 121ºC and pressure of 15 psi for an autoclave residence time of not less than 45 minutes; or ii. A temperature of not less than 135ºC and pressure of 31 psi for an autoclave residence time of not less than 30 minutes. � Textbook of Medicine update – Kamlesh tewary.

ENCAPSULATION � Solid, liquid, and semi-liquid waste can be encapsulated in metal drums � Land. Flling of large quantities of pharmaceuticals is not recommended unless the waste is encapsulated and disposed of in sanitary landfill sites, where the risk of groundwater contamination is minimized. � Large amounts of pharmaceutical waste should not be disposed of with general hospital waste, nor should they be diluted and discharged into sewers (except for certain very mild solutions, such as vitamin preparations). Application of treatment and disposal methods-Int. J. Environ. Res. Public Health 2015 , 6818 6831

� This method involves filling the containers made of high density polyethelyne or metal drums, with waste. � These containers are filled up with a medium of immobilising material such as plastic foam , clays cement motar. � After the medium has dried the containers are sealed and disposed off in the land fill sites.

Intravenous fluids and glass ampoules are special cases. Intravenousfluids (salts, amino acids, lipids, glucose, etc. ), which are relatively harmless, can be disposed of to a landfll or discharged into a sewer. � Ampoules should be crushed on a hard, impermeable surface; workers should wear protective clothing, eye protection, gloves, etc. The glass should then be swept up, collected, and disposed of with sharps. � Ampoules should not be incinerated as they may explode, damaging the incinerator or injuring workers. � Application of treatment and disposal methods-Int. J. Environ. Res. Public Health 2015 , 6818 6831

MICROWAVE � Most microorganisms are destroyed by the action of microwave at a frequency of about 2450 MHz and a wavelength of 12. 24 cm. � The water contained within the waste is rapidly heated by the microwaves and the infectious components are destroyed by heat conduction. � The efficiency of the microwave disinfection should be checked routinely through bacteriological and virological tests. Through the special arrangement of the entry of microwaves into treatment chamber, the waste is evenly heated to a temperature of 97100°C. Application of treatment and disposal methods-Int. J. Environ. Res. Public Health 2015 , 6818 6831

Microwaving is suitable for the treatment of most infectious waste and is done in special microwaving waste treatment facility, with the exception of body parts, human organs, contaminated animals carcasses and metal items. � In this type of disinfection process, the waste is first shredded. The shredded waste is then mixed with water and subjected to microwaves. The microwaves internally heat the waste, rather than applying heat externally, as in an autoclave. � Application of treatment and disposal methods-Int. J. Environ. Res. Public Health 2015 , 6818 6831

The heat generated in this method provides even heating over all portions of the waste, and the high-temperature steam that is generated effectively neutralizes all biologicals. � The shredding operation reduces the volume of the waste by up to 80%, and the treated waste can be disposed of in a landfill. The entire process takes place within a single vessel, and the system can be operated by unskilled workers. � Application of treatment and disposal methods-Int. J. Environ. Res. Public Health 2015 , 6818 6831


HYDROCLAVE It is a much advanced method for treating infectious waste, utilizing steam, but with much faster and much more even heat penetration. � Its a double walled cylindrical vessel, mounted horizondally. The vessel is filled with a mixing arm that rotates slowly inside the vessel. � Essentials of public health dentistry- soben peter

� Hydroclave works; � Stage 1 -loading; it is loaded it can process the bagged waste, sharp containers , liquid containers, cardboard containers, metal objects and pathological waste. � Stage 2 -sterilizing; the powerfull rotators mix the waste and breaks it in to small pieces. Steam is filled in the double walled jacket of vessel, which heats the interior of the vessel. After 20 minites all the waste and liquid become sterile Essentials of public health dentistry- soben peter

Stage 3 -dehydration; the vent is open. The vessel is depressurized through a condensor and sterile liquid is drained into sanitary sewer. Steam mixing is continued untill all the liquid is evaporated and the waste becomes dry. � stage 4 -unloading; the unloading door is opened. the mixture is now rotated in opposite direction, so that all the waste is pushed out. The dry sterile waste is further fined and dropped in the bin and disposed. � Essentials of public health dentistry- soben peter

SHREDDING Shredding will result in reducton in the volume of waste and also it will prevent its re-use and facilitates plastic recycling. it is required for sharp waste and solid waste. It should be ensured that waste is disinfected by chemical/microwaving/ autoclaving before shredding. Community medicine with recent advances-AH Suryakantha

PLASTIC SHREDDER It has an entry chamber known as hopper and an array of rotating shredding knives. The plastics are destroyed in to uniform sized particles, resulting in the reduction in volume Community medicine with recent advances-AH Suryakantha

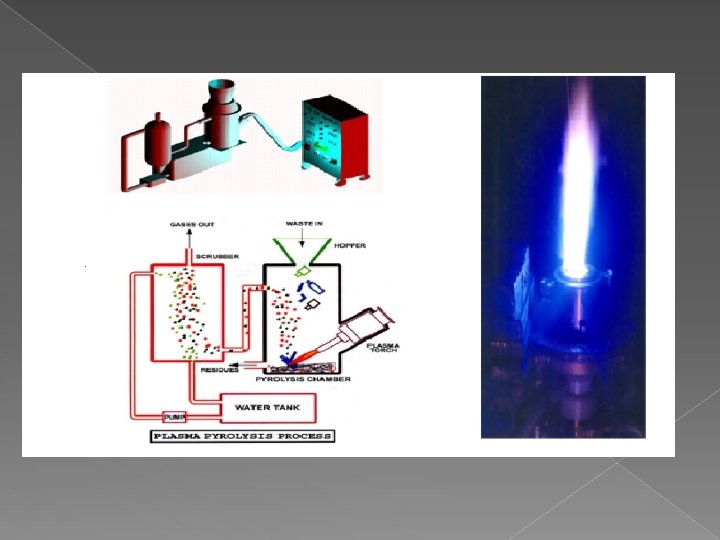
SPECIAL SECTION: PLASMA APPLICATIONS CURRENT SCIENCE, VOL. 83, NO. 3, 10 AUGUST 2002 271 PLASMA PYROLYSIS Plasma pyrolysis is a state-of-the-art technology for safe disposal of medical waste. � It is an environment friendly technology, which converts organic waste into commercially useful by-products. The intense heat generated by the plasma enables it to dispose all types of waste including municipal solid waste, biomedical waste and hazardous waste in a safe and reliable manner. � Medical waste is pyrolyzed into CO, H 2, and hydrocarbons when it comes in contact with the plasma-arc. � Plasma pyrolysis of medical waste special section: plasma application , current science Vol 83, No 3, 10 Aug 2002
. In the plasma pyrolysis")
These gases are burned and produce ahigh temperature (around 1200°C). In the plasma pyrolysis process, the hot gases are quenched from 500° to 70°C to avoid recombination reactions of gaseous molecules that inhibit the formation of dioxins. � The gas analysis results reveal that toxic gases found after the combustion are well within the limit of the Central Pollution Control Board’s emission standards. The plasma environment kills thermally -stable bacteria. � Plasma pyrolysis of medical waste special section: plasma application , current science Vol 83, No 3, 10 Aug 2002

Plasma, the state of matter formed by removing the bound electrons from atoms, is an electrically conducting fluid consisting of charged and neutral particles. � The charged particles have high kinetic energies. When the ionized species in the plasma recombine with the stripped electrons, significant amounts of energy in the form of ultraviolet radiation are released. � Plasma pyrolysis of medical waste special section: plasma application , current science Vol 83, No 3, 10 Aug 2002

� The particle kinetic energy takes the form of heat and can be used for decomposing chemicals. In addition, the presence of charged and excited species renders the plasma environment highly reactive, which can catalyse homogeneous and heterogeneous chemical reactions. � In plasma pyrolysis, the most likely compounds that form from carbonaceous matter are methane, carbon monoxide, hydrogen, carbon dioxide and water molecules. � Plasma pyrolysis integrates thermo-chemical properties of plasma with the pyrolysis process. Plasma pyrolysis uses extremely high temperatures of plasma-arc in an oxygen starved environment to completely decompose waste material into simple molecules. Plasma pyrolysis of medical waste special section: plasma application , current science Vol 83, No 3, 10 Aug 2002

� Hot plasmas are particularly appropriate for treatment of solid waste and can also be employed for destruction of toxic molecules by thermal decomposition. � Unlike incinerators, segregation of chlorinated waste is not essential in this process. Another advantage of plasma pyrolysis is the reduction in volume of organic matter, which is more than 99%. Based on numerous advantages of plasma technology it is speculated that in the near future, plasma pyrolysis reactors will be widely accepted for toxic waste treatment. � Plasma pyrolysis of medical waste special section: plasma application , current science Vol 83, No 3, 10 Aug 2002

Unlike their smoke-belching, conventional counterparts, plasma pyrolysis facilities burn the waste without producing any harmful residuals. � In plasma pyrolysis the quantity of toxic residuals (dioxins and furans) is much below the accepted emission standards and it does not require segregation of hazardous waste. In addition, the pathogens are completely killed and there is a possibility to recover energy �

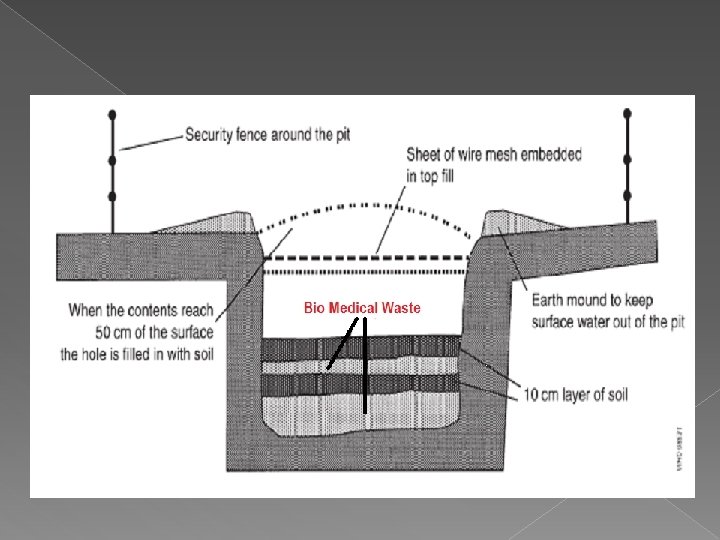
DEEP BURIALS › A pit or trench should be dug about 2 meters deep. It should be half filled with waste, then covered with lime within 50 cm of the surface, before filing the rest of the pit with soil. › It must be ensured that animals do not have any access to burial sites. Covers of galvanised iron/wire meshes may be used. › On each occasion, when wastes are added to the pit, a layer of 10 cm of soil shall be added to cover the wastes. › Burial must be performed under close and dedicated supervision. Textbook of Medicine update – Kamlesh tewary.

› The deep burial site should be relatively impermeable and no shallow well should be close to the site. › The pits should be distant from habitation, and sited so as to ensure that no contamination occurs of any surface water or ground water. The area should not be prone to flooding or erosion. › The location of the deep burial site will be authorised by the prescribed authority. › The institution shall maintain a record of all pits for deep burial Textbook of Medicine update – Kamlesh tewary.
Pyrolytic incinerators Highly effective for all infectious waste Incomplete distruction")
Treatment method Advantages disadvantages a)Pyrolytic incinerators Highly effective for all infectious waste Incomplete distruction of cytotoxins, investing and operating cost are very high b)Single chamber incineration Disinfection efficiency is resonably good. Drastic reduction in waste by volume and weight. residue may be disposed off in landfills. does not require highly skilled persons. investment and operation cost is low. Significant emission of atmospheric pollutants. slag and sloot to be removed periodicaly. thermal resistantchemicals and cytotoxins are not effectively distroyed c)Rotary klin Effective for all infectious Investment and waste operation is very costly 1. incinerators
Chemical disinfection Highly effective method. disinfectants are cheap Requires the services of highly skilled")
2)Chemical disinfection Highly effective method. disinfectants are cheap Requires the services of highly skilled persons, requires safety measures 3)Autoclaving method No environmental pollution, cost effective Requires the services of quilified persons, frequent breakdown can occur. 4)Deep burial Low cost, simple process, relatively safe Site should be accessable, certain precautions should be taken. 5)microwave irradiation Highly efficient, 3040%volume reduction, minimum environmental pollution, and occupational risk and compact nature of the equipment. Investment and operating cost is relatively high

Waste catogories contents Treatments Color code Type of and container disposal options Human anatomic waste Human tissues, organs, body parts Incineration/deep burial yellow Plastic bag Animal waste Animal tissues, organs, body parts, carcasses, bleeding parts , fluids, blood and experimental animals used in research, waste generated by veterinary hospitals, animal houses Inceneration/deep burial Yellow Plastic bag Microbiology and biotechnology waste laboratory Local cultures, stocks, specimns of autoclaving/incener miicroorganisms, human ation/microwaving and animal cell culture used in research and industrial waste, waste from production of biological, toxin, dishes and devices used for transfer of cultures Yellow / red Plastic bag/disinfected container

Waste sharps Needles , syringes, scalpels , blades , glass that may cause puncture and cuts. this includes both used and unused sharps. Disinfection/chemic al treatment and autoclaving/microw aving and shredding Blue /white tranluscent Plastic bag/puncture proof containers Discarded medicines and cytotoxic drugs Waste comprising of outdated, contaminate d anddiscarded medcines inceneration /distruction and disposal in secured landfills/ Black Plastic bags Soiled waste Items contaminated Incineration/autoclavi with blood and body ng/microwaving fluids including cotton, dressing, soiled plstercast, linens, bed dings and other materials contaminated with blood. Yellow/red Disinfected container/plstic bag Solid waste Waste generated from disposal items other than the waste sharps such as tubing, catheters, intra venous sets etc Red/blue/white Disinfected containers/plastic bags Disinfection/chemical treatment and autoclaving/microwav ing and shredding

Liquid waste Waste generated from laboratory and washing, Cleaning, d isinfecting and housekeeping activities. Disinfection by chemical treatment and dischared into the drains. NA NA Incineration ashes Ashes from incineration of any biomedical waste Disposal in muncipal landfill black Plastic bags Chemical waste Chemicals used in the production of biological, chemicals used in disinfections, as insecticides, etc Chemical treatment and discharge into drainsfor liquids and secured landfills for solids black Plastic bags

SUMMARY

REFERENCES � � � Textbook of Community medicine with recent advances -AH Suryakantha Textbook of medicine update-Kamalesh tewary, Vijay kumar. 2 nd edition Textbook of environmental management in health care facilities-Kathryn. D. Waner, Claude. D. Rounds, PE Robert Spurgin. Textbook of Control of hospital infection-Gay ayliffe, A. P. Fraise. 4 th edition Infection control and management of hazardous materials for dental team- Chris H Miller, Charles John Palenik- 3 rd edition

Application of treatment and disposal method. Int. J. Environ. Res. Public Health 2015 � Special section; plasma application, current science vol 83, no 3, 10 aug 2002. � Analysis of information, impact and control of HIV amongst dental professionals in india. Jatin agarwal et al. Journal of clinical and diagnostic reasearch 2015 jul, vol-9(7) � Guideines for safe disposal of unwanted pharmaceuticals in and after emergencies WHO 1991. Tim Grayling, Philip rushbrook, Giles bernard forte. �
- Slides: 123