NEUROLOGIC AL EXAMINATIO N INTRODUCTI ON A examinati








 are defined as the connections of motor nerves before")







 – Three Categories: • Eye opening •")

















 assessment of eye movement in")







 CN X Vagu s:")



 Hemi-atrophy")








 Pain/Temperature Sensation (Spinothalamic Tract) Vibration/Position Sensation (Posterior Columns) Cortical")
 Temperature • Sensation of Cold")


 •")

 • GRADED 0 - 5 – 0 -")







- Slides: 71
NEUROLOGIC AL EXAMINATIO N
INTRODUCTI ON: A examinati is assessment of neurologi th onsensory neuron and cal e whether nervous system is responses, the especially reflexes, to mot impaired. This typically includes ora determine physical examination and a review of the patient's medical history but not deeper investigation such as neuroimaging. It can be used both as a screening tool and as an investigative
Examples of Definitions awake, • Alert: looks about responds in a meaningful manner to verbal instructions or gestures • Drowsy: oriented when awake but if left alone will sleep • Confused: disoriented to time, place, or person o memory difficulty is common has difficulty with commands exhibits alteration in perception of stimuli, may be agitated
• Stuporo generally unresponsive except to vigorous us: stimulation may make attempt at verbalization to vigorous/repeated stimuli Opens eyes to deep pain • Comatose: unarousable and unresponsive some localization or movement may be acceptable within the comatose category depending on the coma definitions e. g. light coma to deep coma Does not open eyes to deep pain
The difference between Coma and Sleep: • sleeping persons respond to unaccustomed stimuli • sleeping persons are capable of mental activity (dreams) • sleeping persons can be roused to normal consciousness • cerebral oxygen uptake does not decrease during sleep as it often does in coma
Special States of Altered Levels of Consciousness • Brain Death: An irreversible loss of cortical and brain stem activity. • Persistent Vegetative State: A condition that follows severe cerebral injury in which the altered state becomes chronic or persistent. • Locked-in Syndrome: A state of muscle paralysis, involving voluntary muscles, while there is preservation of full consciousness and cognition.
Indicatio ns: A neurological examination is indicated whenever a physician suspects that a patient may have a neurological disorder. Any new symptom of any neurological order may be an indication for performing a neurological examination.
Signs &/or symptoms that cannot be faked must be examined closely. Examples include, asymmetry in pupils, abnormal retinal exams, nystagmus, muscle atrophy, and muscle ORGANİC fasciculation. DİSEASE?
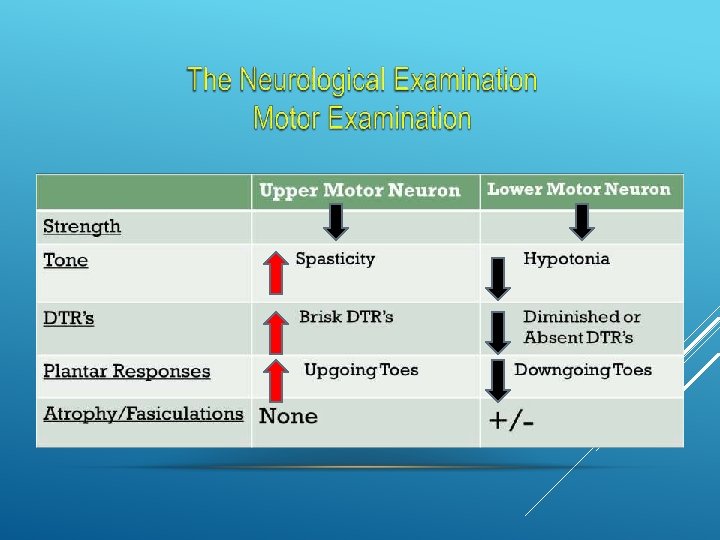
Upper Motor Neurons (UMN) are defined as the connections of motor nerves before they leave the spinal cord Lower Motor Neurons (LMN) are defined as after the synapse (connection) into the peripheral nerve cell bodies.
Objectiv es Organize Exam into the 6 Subsets of Function Concept of Screening Examination Understand Afferent and Efferent Pathways for Brainstem Reflexes Differentiate Between Upper and Lower Motor Neuron Findings
Six Subsets of the Neuro Exam Here’s what you need to examine. Mental Status Cranial Nerves Motor Sensory Coordination Reflexes
Concept of a Screening Exam Screening each of the subsets allows one to check on the entire neuroaxis (Cortex, Subcortical White Matter, Basal Ganglia/Thalamus, Brainstem, Cerebellum, Spinal Cord, Peripheral Nerves, NMJ, and Muscles) Expand evaluation of a given subset to either • Answer questions generated from the History • Confirm or refute expected or unexpected findings
Neurological Examination Mental Status Exam “FOGS” Family story of memory loss Orientation General Information Spelling &/or numbers Recognition of objects
1. INTERVIEW The patient/family interview will allow to: • ƒ gather data: both subjective and objective about the patient's previous/present health state • ƒ provide information to patient/family • ƒ clarify information • ƒ make appropriate referrals • ƒ develop a good working relationship with both the patient and the family • ƒ initiate the development of a written plan of care which is patient specific
Interview to identify • presence headacheof: • • • difficulty with speech inability to read or write alteration in memory altered consciousness confusion or change in thinking disorientation decrease in sensation, tingling or pain motor weakness or decreased strength decreased sense of smell or taste change in vision or diplopia difficulty with swallowing decreased hearing
Physical Examination Considerations • Level of Consciousness – Most important aspect of neurologic examination – Level of consciousness first to deteriorate; changes often subtle, therefore requiring careful monitoring. • Consciousness: – Composed of Two Components: • Arousal (Alertness) • Awareness (Content) – Assessment: Orientation vs. Disorientation » Person, Place & Time
Assessing LOC • Glasgow Coma Scale (GCS) – Three Categories: • Eye opening • Best motor response • Best verbal response – Scoring • Highest or best possible score 15 • A score of < 8 indicates coma
Glasgow Coma Scale
Pupillary Examination examination can be • The performed or minimally pupilla in the unconscious quickly and easily responsive patient when a TBI is suspected, and ry can provide valuable information about the degree of initial or progressing brain injury. Several types of TBI’s may cause pupillary changes, which indicate the need for rapid interventions to decrease ICP caused by cerebral bleeding and/or edema. Nurses are in a key position to detect early changes in a patient's condition and administer or advocate for immediate interventions.
Check pupil size in lighted room, and reactivity to light in a darkened room.
Unequal pupil size can be a sign of a serious brain injury.
Brain Injury with bleeding or swelling Rapid interventions are needed to prevent death or permanent brain damage – TBI’s can progress rapidly!
Mental Status Level of Alertness • Subjective view of Examiner • Definition of Consciousness • Terminology for Depressed Level of Consciousness • Concept of Coma • Delerium Degree of Orientation • To what?
Mental Status Concentration • Serial 7’s or 3’s • “WORLD” backwards • Months of the Year Backwards • Try to quantify degree of impairment * A and O and Concentration need to be intact for other aspects of the Mental Status Exam to have localizing value!
Mental Status Memory Immediate Recall • A task of concentration Short-Term Memory • “ 3/3 objects after 5 minutes” Long-Term Memory • Last thing to go
Mental Status Aphasia vs Dysarthria Languag Receptive Language e • Command Following Expressive Language • Fluency • Word Finding Repetition • Screens for Receptive, Expressive, and Conductive Aphasias
Langua ge
Mental Calculations, R-L confusion, finger Status agnosia, agraphia • Gerstmann’s Syndrome (Dominant Parietal Lobe) Hemineglect • Non-Dominant Parietal Lobe Delusional Thinking, Abstract Reasoning, Mood, Judgement, Fund of Knowledge, etc • Important for Psychiatry • Does not localize well to one region of the cortex • Neurocognitive Testing required to get at more specific deficits
OLFACTORY NERVE I
Distinguish Coffee from Cinnamon Smelling Salts irritate nasal mucosa and test V 2 Trigemminal Sense Disorders of Smell result from closed head injuries OLFACTORY NERVE
OPTİC NERVE CRANİAL NERVE II
Optic Nerve Acuity Visual Fields Afferent input to Pupillary Light Reflex • APD Look at the Nerve (Fundoscopic Exam) “VA equals 20/20 OU at near” “PERRLA”
Abducens Nerve Cn VI Oculomotor Nerve Cn III Trochlear Nerve c. n. IV
CN III Oculomotor: moves eyes in all directions except outward and down & in; opens eyelid; constricts CN pupil. IV Trochlear: moves eyes down and in…. .
CN VI Abducens: moves eyes outward EOM’s: (extraoccular movement) assessment of eye movement in all directions ( III, IV VI)
TRİGEMİNAL NERVE V
CN V Trigemin 3 branches; sensation al: the face, cornea and to scalp; opens jaw against resistance
FACİAL NERVE-VII
CN VII Facial: moves the face; taste. CN VII paralysis
VESTİBULOCOCHLEAR NERVE-VIII
Vestibulocochlear Nerve • Patientsand will complain of tinnitis, hearing loss, Hearing Balance and/or vertigo Weber and Renee Test • Differentiates Conductive vs Sensorineural hearing loss Afferent input to the Oculocephalic Reflex • Doll’s Eye Maneuver • Cold Calorics
Glossopharyngeal and Vagus Nerves c. n. ’s IX and X
CN IX Glossopharyngeal: moves the pharynx (swallow, speech & gag) CN X Vagu s: voice quality
Spinal Accessory Nerve c. n. XI Sternocleido. Mastoid strength Trapezius strength
Shoulder Shrug CN XI SPİNAL ACCESSORY: TURNS HEAD AND ELEVATES SHOULDERS
Hypoglossal Nerve c. n. XII
Hypoglossal Nerve Protrudes the tongue to the opposite side Tongue in cheek (strength) Hemi-atrophy and fasiculations (LMN)
Strength Tone DTR’s Plantar Responses Involuntary Movements
Strength Medical Research Council Scale 5/5 = Full Strength 4/5 = Weakness with Resistance 3/5 = Can Overcome Gravity Only 2/5 = Can Move Limb without Gravity 1/5 = Can Activate Muscle without Limb 0/5 = Cannot Activate Muscle
Describe the Distribution of Weakness • Upper Motor Neuron Pattern • Peripheral neuropathy Pattern • Myopathic Pattern WEAKNESS
Tone is the resistance appreciated when moving a limb passively “Normal Tone” Hypotonia • “Central Hypotonia” • “Peripheral Hypotonia” Increased Tone • Spasticity (corticospinal) TONE • Rigidity (Basal Ganglia, Parkinson’s Disease) • Dystonia (Basal Ganglia)
DTR’s 0/4 = Absent 1 -2/4 = Normal Range 3/4 = Pathologically Brisk 4/4 = Clonus
Involuntary Movements • Chorea Hyperkinetic Movements • Athetosis • Tics • Myoclonus Bradykinetic Movements • Parkinsonism (Bradykinesia, Rigidity, Postural Instability, Resting Tremor) • Dystonia
Drift Assessment: test for motor weakness Arm: hold arms out with palms up; eyes closed • Pronator drift: hands pronate (roll over); • Motor drift: arm “drifts” downward • Cerebellar drift: arm “drifts” back toward head or out to side Leg: no need to close eyes motor: leg “drifts”toward bed
Movement Assessment Movements are purposeful or non-purposeful tubings or bed linens, scratching nose localizing: moving toward or removing a painful stimulus; must cross the midline; occurs in the cortex withdrawal: pulling away from pain; occurs in the hypothalamus purposeful: picking at non-purposeful: do not cross the midline abnormal flexion: (decorticate) rigidly flexed arms and wrists; fisted hands; occurs in upper brainstem abnormal extension: (decerebrate) rigidly, rotated inward extended arms with flexed wrists and fisted hands; occurs in midbrain or pons. Decorticate Decerebrate
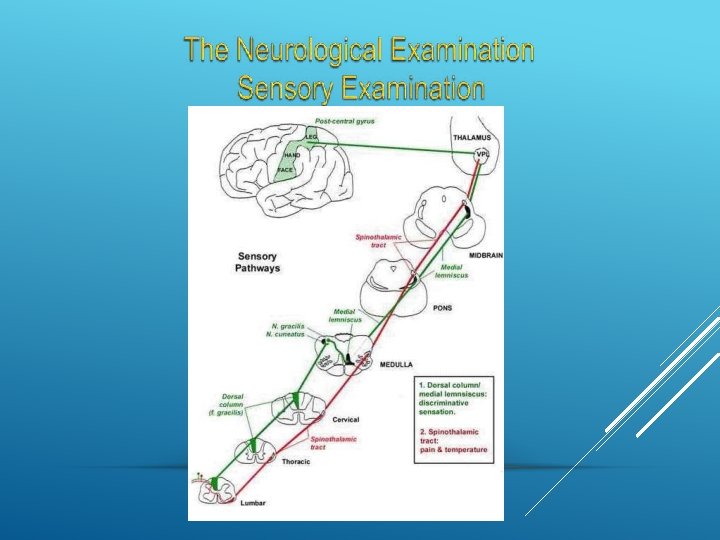
Light Touch (Multiple Pathways) Pain/Temperature Sensation (Spinothalamic Tract) Vibration/Position Sensation (Posterior Columns) Cortical Sensory Modalities Stereognosis Graphesthesia Two-Point Discrimination Double Simultaneous Extinction Primary Sensory Modalities
Pain and • Pinprick (One pin per patient!) Temperature • Sensation of Cold • Look for Sensory Nerve or Dermatomal Distribution Vibration Sensation • C-128 Hz Tuning Fork (check great toe) Joint Position Sensation • Check great toe
Higher Cortical Sensory Function Graphesthesia Stereognosis Two-Point Discrimination Double Simultaneous Extinction Gerstmann’s Syndrome (acalculia, right-left confusion, finger agnosia, agraphia) • Usually seen in Dominant Parietal Lobe lesions
Dysmetria on Finger-Nose-Finger Testing* Irregularly-Irregular Tapping Rhythm* Dysdiadochokinesis* Impaired Check* Hypotonia* Impaired Heel-Knee-Shin* Falls to Side of Lesion* Nystagmus. HEMİSPHERE (Variable Directions) * All Deficits are Ipsilateral to the side of the lesion. DYSFUNCTİON
Truncal Ataxia Titubation Ataxic Speech Gait Ataxia • Acute Ataxia (unsteady Gait) • Chronic Ataxia (wide-based, steady Gait)MİDLİNE DYSFUNCTİON
REFLEX ES
MUSCLE STRETCH REFLEXES (DEEP TENDON REFLEXES) • GRADED 0 - 5 – 0 - ABSENT – 1 - PRESENT WITH REINFORCEMENT – 2 - NORMAL – 3 - ENHANCED – 4 - UNSUSTAINED CLONUS – 5 - SUSTAINED CLONUS
MSR / DTR • BICEPS • BRACHIORADI ALIS • TRICEPS • KNEE • ANKLE
OTHER REFLEXES • Upper motor neuron dysfunction – BABINSKI • present or absent • toes downgoing/ flexor plantar response – HOFMAN’S – JAW JERK • Frontal release signs – GRASP – SNOUT
Abmornal Abnormal Reflexes: Reflexes Babinski: initial inflection of great toe in response stroking of sole; upgoing toe is abnormal Grasp: involuntary grasp in response to stimulation of palm; abnormal in an adult Doll’s eyes: impairment of eye movement to opposite side when head is turned = damage to brainstem; no movement = loss of brainstem
• • • Neuro Aessessment • . 4. A Coup Contracoup injury is 1. Peripheral Nervous System defined as: When the head strikes (PNS) is made. Quiz up of the a fixed following except: : Cranial nerves (12) Ventricles Axons and Neurons Spinal nerves (31) Cerrebellar nerves 2. The Autonomic Nervous System contains both the Sympathetic Division of nerves and the Parasympathetic Division of nerves. True or False _. 3. Intracranial Hemorrhage can occur in the following places except: Epidural space Subarachnoid space Ethmoid space object, the coup injury occurs at the site of impact and the contrecoup injury occurs at the opposite side. True or False_ • 5. The Facial nerve controls: • Movement of the chin, tongue and parotid glands. • Movement of the tongue, soft palete and eyebrows. • Movement of the chin and cheeks muscles. • Movement of all the facial expression muscles. • 6. Which nerve controls movement on the neck and shoulders? • Abducens • Accoustic • Spinal Assesory • Occulomotor
• • • 7. A serious injury to the cervical spine and spinal cord most likely will result in the following condition: Hemiplegia Quadraplegia Paraplegia Contralateral paralysis 8. Any suspected head, neck or spine injured victim should immediately be given spinal immobilization precautions, except: When the victim complains of pain only upon turning his head to one side. When the victim refuses to allow spinal immobilization even after listening carefully to multiple attempts to explain the dangers and risk involved. When the victim is intoxicated on alcohol and cannot speak clearly. When the victim was never unconscious and denies any pain. • 9. When assessing a patient with altered LOC, you feel his state of awareness/arousal is best described as “Obtunded”, this means: • Very drowsy, when not stimulated, but can follow simple commands when stimulated (i. e. shaking or shouting); verbal responses include one or two words, but will drift back to sleep without stimulation. • A state of drowsiness; client needs increased external stimuli to be awakened but, remains easily arousable; verbal, mental & motor responses are slow or sluggish. • Awakens only to vigorous and continuous noxious (painful) stimulation; minimal spontaneous movement; motor responses to pain are appropriate but, verbal responses are minimal and incomprehensible (i. e. moaning). • Vigorous external stimulation fails to produce any verbal response; both arousal and awareness are lacking; no spontaneous movements but, motor
• • • • 10. The Glasgow Coma scale tests for three kinds of responses, they are: Eye Opening Motor Response Verbal Response Auditory Response 11. The best and worst possible score on the GCS is: 15 and 0 13 and 3 15 and 3 18 and 5 12. When assessing pupillary response, you are looking for the following conditions except: Coordinated eye movement and bilateral blinking. Reactivity to and accommodation to light. Symmetry of pupils and accommodation to light. Abnormal pupil shape. • 13. A constricted “pin point” pupil indicates: (best answer) a) Brain Stem herniation b) Cardiac Arrest c) Cerebral Infarction of the parietal lobe d) Cerebral Infarction of the occipital lobe e) A wide variety of conditions, some being extremely life threatening. • 14. What Cranial nerve(s) controls the movement of the eyes down and CN IIin? Optic a) CN VI Abducens 15. The Motor strength scale goes b) CN III Oculomotor from 0/5 to 5/5, 0 being no strength at 5 being normal strength. A c) all CNand IV Trochlear d) • person with a motor strength of 4/5 would be: • overcomes gravity; offers no resistance • strong against resistance • weak against resistance • no muscle movement
• • • 16. Match the following postures with its definition: Decerebrate_ Decorticate_ a) Abnormal flexion: rigidly flexed arms and wrists; fisted hands; occurs in upper brainstem b) Abnormal extension: rigidly, rotated inward, extended arms with flexed wrists and fisted hands; occurs in midbrain or pons. c) 17. The Babinski reflex is the initial inflection (extension) of great toe in response stroking of the sole of the foot, select the correct answer: d) An upgoing great toe is abnormal. e) An upgoing great toe is normal. f) An upgoing great toe is abnornal in g) adults. h) An upgoing great toe is normal in infants. • • • • • Answers 1 e 2 True 3 d 4 True 5 d 6 c 7 b 8 b 9 a 10 d 11 c 12 a 13 e 14 c 15 c 16 Decer = b. Decor =a 17 c&d