Gregg Lueder Marlo Galli JAAPOS Journal of American
 Journal of American Association for Peadiatric")








 Journal of American Association for Peadiatric")





- Slides: 18
Gregg Lueder & Marlo Galli ( JAAPOS ) Journal of American Association for Peadiatric Ophthalmology and strabismus 2008
� Infantile esotropia or "congenital" esotropia is a common type of childhood strabismus. � This esodeviation has onset before 6 months of age and occurs in children who have a low refractive error and typically are neurologically normal. � Donahue, SP. Clinical practice. Pediatric strabismus. N Engl J Med 2007; 356: 1040. � Guthrie, ME, Wright, KW. Congenital esotropia. Ophthalmol Clin North Am 2001; 14: 419
� The esotropia is typically large angle, usually greater than 25 to 30 prism diopters � Children who have infantile esotropia sometimes turn their faces toward the fixing eye, which is preferably positioned in adduction (cross-fixation). � Guthrie, ME, Wright, KW. Congenital esotropia. Ophthalmol Clin North Am 2001; 14: 419
Child with infantile esotropia
� Idiopathic infantile esotropia is associated with a variety of other ocular motility abnormalities that may manifest later in childhood as: � Oblique muscle dysfunctions � Dissociated strabismus complex � Latent nystagmus � Amblyopia, ( which may develop in 17 to 50% of affected children ). • Calcutt, C, Murray, AD. Untreated essential infantile esotropia: factors affecting the development of amblyopia. Eye 1998; 12 ( Pt 2): 167.
� Surgery designed to strengthen or weaken the extraocular muscles is the mainstay of therapy. The procedure most commonly performed is to weaken the medial rectus muscle(s). � Usually it is performed in both eyes. � Successful ocular alignment initially is achieved in the majority of children. • Birch, E, Stager, D, Wright, K, Beck, R. The natural history of infantile esotropia during the first six months of life. Pediatric eye disease investigator group. J AAPOS 1998; 2: 325.
� The primery goal of treating infantile esotropia is to restore binocular vision and the Surgical realignment of the eye is the principal method used to achieve this goal.
� Several studies have demonstrated that restoring alignment prior to 2 years of age results in better outcomes compared with alignment at a later age. � Taylor DM, ME, How early is early surgery in the management of strabismus? . Arch Ophthalmol 1963; 70: 752 -6 � Zak TA, Morion JD, Early surgery for infantile esotropia. Can J Ophthalmol 1982; 17: 213 -8 � Simonsz HJ, Kolling GH, Unnebrink K. Final report of early vs late Infantile strabismus surgery study (ELISSS) a controlled, prospective, multicenter study. Strabismus 2005; 13: 169 -99
� Some strabismus surgeons postpone surgery until the angle of deviation stabilizes. � This approach, however, may result in a delay of treatment that could adversely affect the outcome. .
Gregg Lueder & Marlo Galli (J AAPOS ) Journal of American Association for Peadiatric Ophthalmology and strabismus 2008 • Department of Ophthalmology and visual sciences, Washington University, School of Medicine, St Louis, Missouri, USA
� Some strabismus surgeons wait until the angle of deviation stabilizes prior to operating on patients with infantile esotropia. � This study evaluated whether a preoperative increase in the angle of deviation affected surgical outcomes.
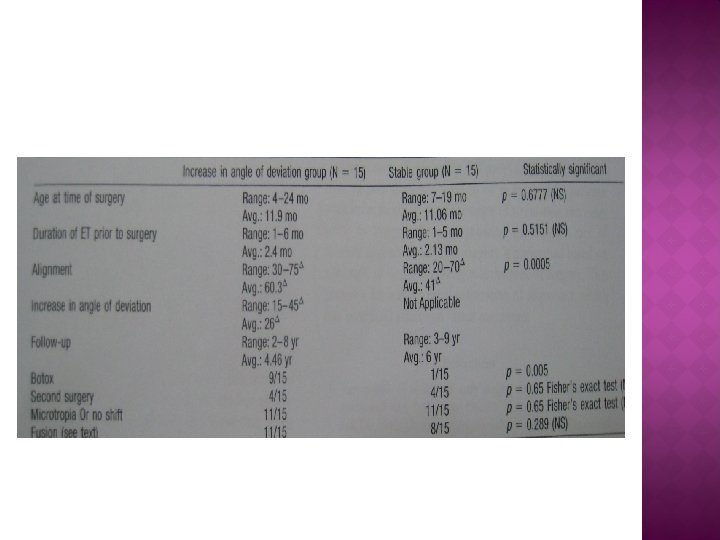
� This was a retrospective comparative case series in which records of patients with infantile esotropia, who had surgery performed before age 2 years and who were followed for at least 2 years postoperatively, were reviewed to identify two groups for comparison: � the first had ≤ 5Δ change in the angle of deviation between the first office visit and time of surgery � the second had a ≥ 10Δ increase in the angle of deviation prior to surgery. “ surgery was performed for the angle present at the time of surgery “.
� Outcomes were considered successful if the patients had microtropias. � All the angle of measurements were performed by a certified orthoptist. � The surgeries were all performed by a single surgeon. � Surgery consisted of bilatral medial rectus recessions with or without botulinuim toxin injection. “ botox injections were used with angle of 65 PD or greater “.
� 15 patients were identified in each group. � The interval between the first office visit and time of surgery was the same in both groups (mean, 2 months). � Outcomes were successful in 11 of 15 (73%) in each group (no significant difference, p = 0. 659).
� There was no difference in outcome between children whose angles of deviation were stable and those whose angles increased prior to surgery. � This indicates that strabismus surgery does not need to be delayed while waiting for the angle of deviation to stabilize. � Surgical correction may therefore be achieved at an earlier age, which may have a beneficial effect on outcome. .