Anxiety Disorders A Closer Look at Psychological Disorders







 ●Excessive anxiety and worry occurring for at least 6 months")






, Howard")






 n Nature n (biological): Heredity – a likelihood")
 n Nature (biological): n n Brain function –")
 n Nature n (biological): Evolution – We are")
 n Nurture (learning): n n n Conditioning –")
 Many phobias appear to")
 n Other Explanations for Anxiety Disorders: n n")










- Slides: 38
Anxiety Disorders A Closer Look at Psychological Disorders
n Ryan’s social phobia has led him to lose jobs and n relationships. In this case, Ryan has a disorder because his behavior is: A. dangerous. B. common. C. medically based. n D. dysfunctional. n If researchers discovered that genetically influenced abnormalities in brain structure contribute to bipolar disorder, this would most clearly add credibility to: A. the DSM-V. n B. the medical model. C. the social-cognitive perspective. D. psychoanalytic theory. n n n n The DSM-V is a diagnostic guide that: n A. describes psychological disorders and their prevalence. n n n B. describes psychological disorders and their causes. n C. describes only disorders that have medical causes. n D. has been shown to have poor reliability and validity. Years after he barely survived a terrorist attack that killed his wife and two children, Mr. Puskari suffers recurring flashbacks and frequent nightmares of the event that render him incapable of holding a steady job. Mr. Puskari is most clearly showing signs of: A. obsessive-compulsive disorder. B. generalized anxiety disorder. C. post-traumatic stress disorder. D. dysthymic disorder. The most common psychological disorder in the U. S. is/are: A. schizophrenia. B. alcohol abuse. C. mood disorders. D. phobias.
DO NOW ¨ Can you think of examples of people/characters from literature, TV, or movies who suffered from one (or more!) of the following disorders? n n Phobic disorder Panic disorder Obsessive-compulsive disorder Post-traumatic stress disorder
n Ryan’s social phobia has led him to lose jobs and n relationships. In this case, Ryan has a disorder because his behavior is: A. dangerous. B. common. C. medically based. n D. dysfunctional. n If researchers discovered that genetically influenced abnormalities in brain structure contribute to bipolar disorder, this would most clearly add credibility to: A. the DSM-V. n B. the medical model. C. the social-cognitive perspective. D. psychoanalytic theory. n n n n The DSM-V is a diagnostic guide that: n A. describes psychological disorders and their n prevalence. n n B. describes psychological disorders and their causes. n C. describes only disorders that have medical causes. n D. has been shown to have poor reliability and validity. Years after he barely survived a terrorist attack that killed his wife and two children, Mr. Puskari suffers recurring flashbacks and frequent nightmares of the event that render him incapable of holding a steady job. Mr. Puskari is most clearly showing signs of: A. obsessive-compulsive disorder. B. generalized anxiety disorder. C. post-traumatic stress disorder. D. dysthymic disorder. The most common psychological disorder in the U. S. is/are: A. schizophrenia. B. alcohol abuse. C. mood disorders. D. phobias.
First, a warning… n Don’t overreact if you begin to discover in yourself some of the symptoms we will discuss. That’s typical. n We all have some of these symptoms some of the time. n Just remember, they do not suggest a disorder unless they meet all four of the criteria we talked about before – the symptoms must be maladaptive, unjustifiable, disturbing, and atypical.
Anxiety Disorders n There are several different kinds of anxiety disorders: Anxiety Disorders Generalized anxiety disorder Panic disorder Phobia Obsessivecompulsive disorder Posttraumatic stress disorder
Anxiety Disorders n n n Anxiety is a general state of dread or uneasiness that a person feels in response to a real or imagined danger. People suffering from anxiety disorders feel anxiety but not just normal anxiety. They suffer anxiety that is out of proportion to the situation provoking it. Anxiety disorders are the most common type of mental illness in the United States, affecting 40 million Americans annually.
GAD Clinical Features (symptoms) ●Excessive anxiety and worry occurring for at least 6 months ●Inability to control the worry ●Considerable distress or impairment in social, occupational or other important areas of life ●Presence of 3 or more of the following: o Restlessness o Being easily fatigued o Difficulty concentrating or mind goes blank o Irritability o Muscle tension o Sleep disturbances
Panic Disorder n n Panic is a feeling of sudden, helpless terror, such as the overwhelming fright one might experience when cornered by a predator. Sufferers of a panic disorder have anxiety accompanied by panic attacks – episodes of unexplained terror and fear that something bad is going to happen. ¨ n Symptoms: may include a sense of smothering, choking, or difficulty breathing; faintness or dizziness; nausea; and chest pains. ¨ n n Panic attacks can last for a few minutes or for an hour or more. Panic disorder may be inherited. The panic victim usually experiences the first attack shortly after a stressful event, but future attacks usually appear out of nowhere. Can cause secondary disorders, such as agoraphobia. ¨ After a number of panic attacks, victims may become so concerned about exhibiting panic in public that they may be afraid to leave home, developing agoraphobia, or a fear of going out in public
Phobic Disorder n n The word “phobia” is the Greek word for “morbid fear. ” It refers to Phobos, the Greek god of terror. The names of most phobias begin with the Greek word for the feared object or situation. A phobia is a fear that is both irrational and disruptive (impairs the ability to lead a normal life). People can have n n n Specific phobias – fear of a particular object, thing, or situation (heights, dogs, spiders, enclosed spaces, etc. ) Social phobias – fear you will embarrass yourself in a social setting (fear of speaking in public, eating in public, meeting strangers, etc. ) Agoraphobia – fear of being away from a safe place (like home); of being away from a familiar person (like a spouse); or of being in crowds or in other situations that are difficult to leave.
0 Abnormal Behavior: Myths and Realities Anxiety Disorders Somatoform Disorders Dissociative Disorders Mood Disorders Schizophrenic Disorders Going out by oneself Being alone Crowds Social Phobias Tunnels or bridges Public transport Eating in public Speaking to new acquaintances Simple Phobias Speaking in public Animals Closed places Storms Water Heights Bugs, mice, snakes, bats Portion of population reporting each phobia (%) Type of Phobias Agoraphobias 25 20 15 10 5 Eating Disorders
Kinds of Phobias Specific Phobia Social Phobia Agoraphobia Fear of particular object Fear and embarrassment in dealing with others Fear of entering certain fear-evoking or unfamiliar situations, which often accompany panic attacks…so avoids crowds where attacks could occur Difference between social and agoraphobia…social afraid of scrutiny of others, while agoraphobia afraid of own internal cues
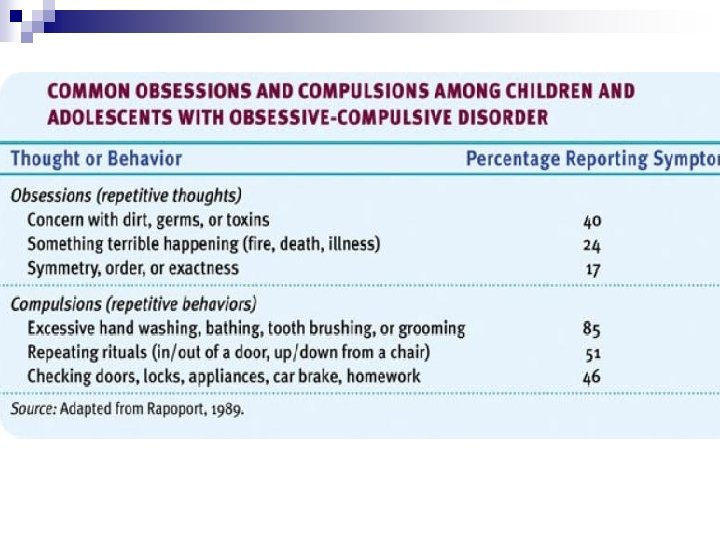
Obsessive-Compulsive Disorder n Two major components: n n n Obsessions – repetitive thoughts Compulsions – repetitive rituals/behaviors Obsessions and compulsions are not always bad things… n n You might become obsessed with the lyrics to your favorite song, which get stuck in your head all day A good athlete might be obsessed with winning and compulsive about training. A good student might be obsessed with grades and compulsive about studying. These are not bad things.
Obsessive-Compulsive Disorder Cycle
Examples of People with OCD As a young man (shown in the photo), Howard Hughes was a handsome, dashing daredevil pilot and movie producer who appeared to be reasonably well adjusted. However, as the years went by, his behavior gradually became more and more maladaptive, as obsessions and compulsions came to dominate his life. In his later years (shown in the drawing), he spent most of his time in darkened rooms, naked, unkempt, and dirty, following bizarre rituals to alleviate his anxieties. (The drawing was done by an NBC artist and was based on descriptions from men who had seen Hughes. )
Post-Traumatic Stress Disorder Four or more weeks of the following symptoms constitute post-traumatic stress disorder (PTSD). 1. Haunting memories. 2. Nightmares/flashbacks. 3. Social withdrawal. 4. Jumpy anxiety. 5. Sleep problems. Bettmann/ Corbis
Post-traumatic Stress Disorder n n A condition in which a person who has experienced a traumatic event feels severe and long-lasting aftereffects. Intense stress is the trigger, and symptoms include nightmares, persistent fear, difficulty relating normally to others, and troubling memories or flashbacks of the traumatic event. PTSD can be extremely long-lasting, lasting decades after the event. People who are exposed repeatedly or over a long period of time to distressing conditions are more likely to develop the disorder ¨ Example: military combat veterans, rape and assault victims, abused children, survivors of natural disasters, etc.
Resilience to PTSD n Only about 10% of women and 20% of men react to traumatic situations and develop PTSD. • Holocaust survivors show remarkable resilience against traumatic situations • All major religions of the world suggest surviving a trauma leads to growth of the individual.
Etiology of Anxiety Disorders What causes an anxiety disorder?
What Causes Anxiety Disorders? n Predictions: ¨. ¨. ¨.
What Causes Anxiety Disorders? n As always seems to be the case, one has to consider both nature and nurture for possible explanations as to the cause of anxiety disorders.
What Causes Anxiety Disorders? (cont. ) n Nature n (biological): Heredity – a likelihood for developing anxiety disorders. The specific fear may not be inherited, but the predisposition to be fearful is. ¨ Twin studies suggest a moderate genetic predisposition to anxiety disorders. They may be more likely in people who are especially sensitive to the physiological symptoms of anxiety. Figure 14. 6: Twin studies of anxiety disorders. The concordance rate for anxiety disorders in identical twins is higher than that for fraternal twins, who share less genetic overlap. These results suggest that there is a genetic predisposition to anxiety disorders. (Data based on Noyes et al. , 1987; Slater & Shields, 1969; Torgersen, 1979, 1983)
What Causes Anxiety Disorders? (cont. ) n Nature (biological): n n Brain function – Brain scans show that people with anxiety disorders have brains that literally function differently from those who don’t (like in the amygdala, the emotion center). This is why such disorders often respond to medication. Abnormalities in neurotransmitter activity at GABA synapses have been implicated in some types of anxiety disorders, and abnormalities in serotonin synapses have been implicated in panic and obsessive-compulsive disorders. Generalized anxiety, panic attacks, and even OCD are linked with brain circuits like the anterior cingulate cortex. Anterior Cingulate Cortex of an OCD patient. A PET scan of the brain of a person with Obsessive-Compulsive Disorder (OCD). High metabolic activity (red) in the frontal lobe areas are involved with directing attention. Brain image of an OCD patient
What Causes Anxiety Disorders? (cont. ) n Nature n (biological): Evolution – We are likely to fear situations that posed danger to the earliest humans. People who didn’t have a healthy dose of fear were less likely to survive. Those who did survive passed on their tendency to fear these dangers to us. § Note: We don’t have a similar inherited tendency to fear threats that have developed more recently. Cars, for example, kill more people in the modern world than snake bites do, yet more people fear snakes than fear cars.
What Causes Anxiety Disorders? (cont. ) n Nurture (learning): n n n Conditioning – We associate fear with certain places or things (like Little Albert). Many anxiety responses, especially phobias, may be caused by classical conditioning and maintained by operant conditioning (we are rewarded when our anxiety is reduced because we avoid the object, for example). Observational learning – We can also learn fears from our parents our older siblings. If we see them experience fear during a thunderstorm, we may learn to fear thunderstorms as well (remember the caged monkeys who became afraid of snakes). Reinforcement – We also learn to associate emotions with actions, depending on the results that follow those actions. If it will reduce our anxiety or fear, we will continue the behavior. (If we are afraid of heights, we learn to avoid heights. Someone with OCD might learn that his compulsive handwashing reduces his anxiety, so he repeats the behavior.
Figure 14. 7: Conditioning as an explanation for phobias. (a) Many phobias appear to be acquired through classical conditioning when a neutral stimulus is paired with an anxiety-arousing stimulus. (b) Once acquired, a phobia may be maintained through operant conditioning. Avoidance of the phobic stimulus reduces anxiety, resulting in negative reinforcement.
What Causes Anxiety Disorders? (cont. ) n Other Explanations for Anxiety Disorders: n n n Our Unconscious – Freud suggested that we repress our painful and intolerable ideas, feelings, and thoughts, resulting in anxiety. Cognitive Theories – Cognitive theories hold that certain styles of thinking, over-interpreting harmless situations as threatening, for example, make some people more vulnerable to anxiety disorders. Personality – The personality trait of neuroticism has been linked to anxiety disorders, and stress appears to precipitate the onset of anxiety disorders. Figure 14. 8: Cognitive factors in anxiety disorders. Eysenck and his colleagues (1991) compared how subjects with anxiety problems and nonanxious subjects tended to interpret sentences that could be viewed as threatening or nonthreatening. Consistent with cognitive models of anxiety disorders, anxious subjects were more likely to interpret the sentences in a threatening light.
Trichotillomania n https: //www. youtube. com/watch? v=FKX 79 Ku. DYy. Y
Somatoform Disorders Characterized by physical symptoms that seem to suggest a physical disorder, yet have no physical causes or evidence suggests that the symptoms are linked to psychological factors Also includes: Munchausen Syndrome, Munchausen by proxy, and Ganser Syndrome 1. Conversion Disorder 2. Hypochondriasis 3. Body Dysmorphic Disorder
Conversion Disorder ●Unexplained symptoms or deficits affecting voluntary motor or sensory function that suggest a medical condition, yet no medical condition exists https: //www. youtube. com/watch? v=_j. Ouq. Acg. Mr. A&t =245 s ●Onset is usually after a stressful event ●Common symptoms are paralysis, blindness, deafness and difficulty walking o. Many of the symptoms are anatomically impossible…i. e. glove anesthesia – inability to feel the hand, yet has sensation in the arm
Conversion Disorder One of the most significant indicators of Conversion Disorder… La Belle Indifference (beautiful indifference) ●The person has extreme anxiety in other areas of life, but lack of concern about what appears to be an incapacitating physical ailment ● Often such symptoms allow the individual to escape from current frustrating situations and sometimes lead to a “secondary gain” such as attention or affection
Hypochondriasis ● Preoccupation with the idea that one has or might get a serious disease, along with misinterpretation of bodily systems or functions ● 3 major characteristics… 1. Physiological arousal (worried, anxious and often have sleep disturbances) 2. Bodily focus (close monitoring of bodily features & preoccupied with physical complaints) 3. Behaviors designed to avoid or check for physical illness (avoids those who have a disease and engages in repeated self-inspection or medical consultation)
Body Dysmorphic Disorder ●Preoccupation with an imagined or exaggerated defect in personal appearance ●Essential feature of BDD is the belief in an imagined defect in appearance ●This preoccupation is time consuming o. Often being about the shape/size of facial features, acne/spots on skin, wrinkles, thinning hair and scars
Body Dysmorphic Disorder ●Individuals with BDD experience marked distress over their supposed deformity ●feelings of self-consciousness about their “defect” may lead to avoidance of work or public situations ●individuals with BDD experience higher rates of Major Depression & suicidal tendencies ●BDD typically becomes evident in adolescence & affects males and females equally
Body Dysmorphic Disorder ●Some examples of what individuals with BDD “see” when they look in the mirror…
If you can watch the mind explained: Anxiety on Netflix! Very good!
Next Class: n Timeline: Reading Guide 8 B n We’ll review some big concepts but plan to see videos mostly of Schizophrenia and a few on Mood. n PPT will go on blog after class to help guide w/any confusion