Acetaminophen paracetamol acetaminophen Prostaglandin synthesis Mechanism of action
")






- Slides: 8
Acetaminophen (paracetamol)
acetaminophen Prostaglandin synthesis Mechanism of action accidental 10 g Circumstances of poisoning suicidal Toxokinetics and pathophysiology GIT Cytochrome liver oxidase NAPQI Conjugated with glutathione Inactive metabolite Toxic intermediate metabolite Binds to hepatic cells Centrilobular hepatic necrosis
Clinical picture 12 -24 hours Anorexia, nausea, vomiting and diaphoresis. 2 -3 days 3 -5 days. 7 -10 days Rt upper abdominal pain and hepatic tenderness. liver enzymes, bilirubin and prolongation of prothrombin time. Severe toxicity Hepatic necrosis, coagulation Death Cause of death: defects, jaundice, renal faiure and encephalopathy are present. Hepatic failure
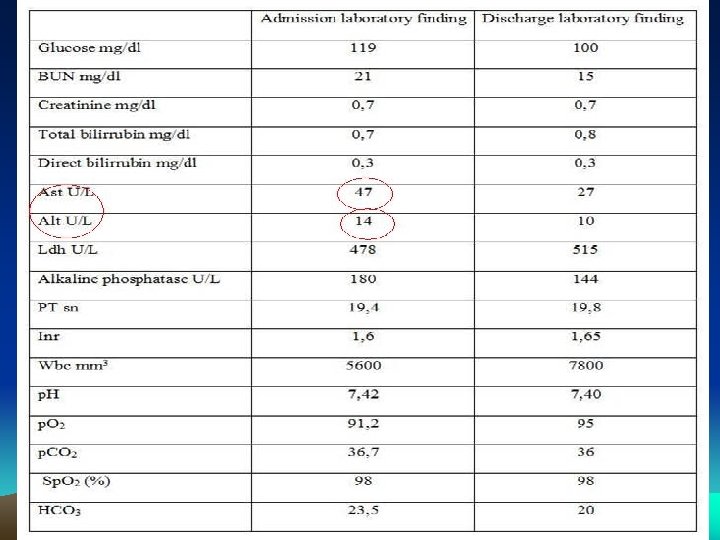
LABORATORY INVESTIGATIONS Assessment of severity of acetaminophen overdose is achieved using Rumack. Mattew nomogram 1. The measured serum acetaminophen level at 4 hours or longer following an acute ingestion predicts the possibility of hepatic injury and it determines the need to treat a patient using its specific antidote. 2 -Aspartate and Alanine transaminase plasma levels. 3 -Coagulation profile 4 -Glucose level 5 -Bilirubin level 6 -Renal function tests 7 -Acid- base status and electrolytes
Management Investigation Toxicological: Non-toxicological serum acetaminophen level Peak level of acetaminophen is achieved 4 -6 hours after ingestion. Liver function tests Renal function tests Blood glucose level Prothrombin time Treatment general supportive specific antidote ABCD by liver support: N-acetylcysteine Emesis or a)5%dextrose (NAC) = Mucomyst gastric I. V. in the first It is in the form of lavage 10 hours 20% solution which followed by must be given within activated b)Blood or 8 -10 hurs of charcoal fresh plasma ingestion of the transfusion. overdose. Dose : c)Clotting 140 mg/kg factors, 70 mg/kg every 4 vitamin K. hours for 3 days. It is given orally in fruit juice. Action: t act as glutathione substitute,
Patients who have serum acetaminophen levels above the treatment line in the nomogram should receive the first dose of NAC within 8 -10 hours of the ingestion. Mechanism of NAC action I-It increases the synthesis of glutathione. II- Increases other route of metabolism of acetaminophen and reducing the amount of NAPQI formed. III- Glutathion substitute: The sulfur group of NAC can also bind and detoxify NAPQI 4 - Fresh frozen plasma or clotting factor (to maintain prothrombin time within safe limit) 5 -Vitamin K. 6 -I. V Glucose administration • Liver support. • Liver transplantation may be life-saving for patients with fulminant hepatic failure. 9 - Treatment of renal failure
THANK YOU