Radiological Category Thoracic Cardiovascular Principal Modality 1 CT
: CT Principal Modality (2): None Case Report")










- Slides: 13
Radiological Category: Thoracic Cardiovascular Principal Modality (1): CT Principal Modality (2): None Case Report #0277 Submitted by: Supreet Singh, M. D. Faculty reviewer: Chitra Chandrasekar, M. D. Date accepted: 06 March 2006
Case History 56 year old female with metastatic non-small cell lung cancer presented to the ED with progressive facial and bilateral upper extremity edema, cough, hoarseness and dysphagia.
CT Chest
Test Your Diagnosis Which one of the following is your choice for the appropriate diagnosis? After your selection, go to next page. • Bulky lymphadenopathy • Pulmonary Embolism • Superior Vena Cava Thrombosis • Superior Vena Cava and Azygous Vein Thrombosis
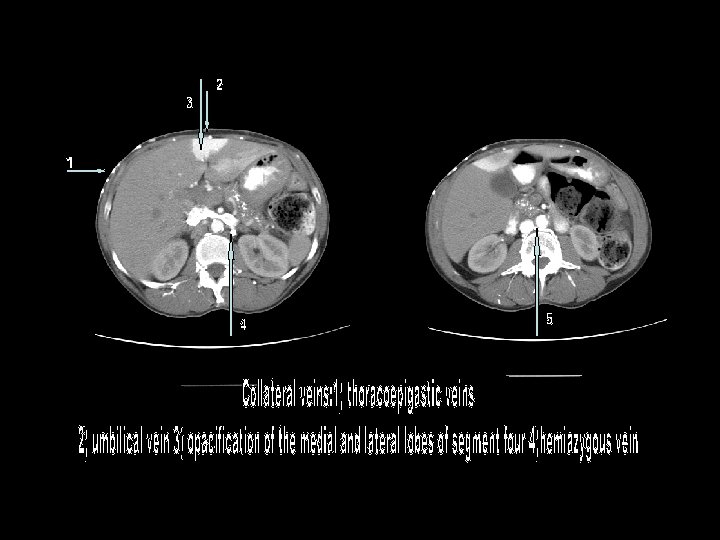
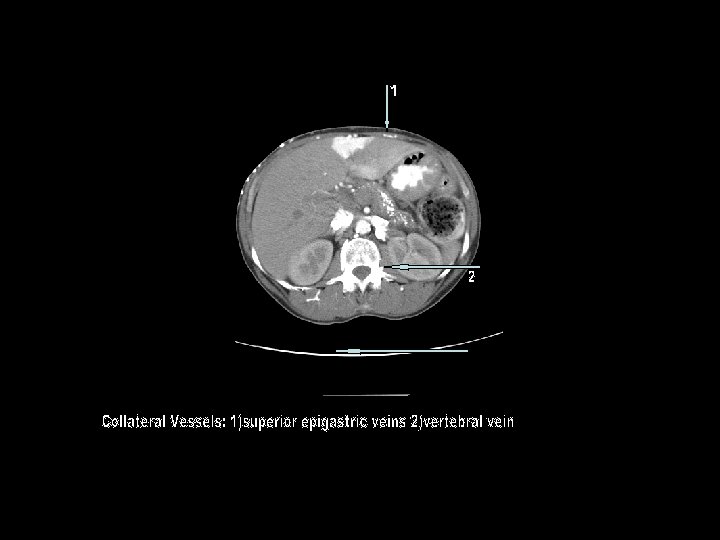
Findings and Differentials Findings: Contrast enhanced CT of chest with intraluminal filling defect in the superior vena cava and the azygous vein. Numerous collateral vessels are seen channeling blood flow from the upper body to the inferior vena cava and the portal system. Differentials: No Differential: SVC and Azygous Vein Thrombosis
Venous Collaterals 1
Venous Collaterals Recruited to Bypass SVC and Azygous Veins 1 1
Diagnosis SUPERIOR VENA CAVA AND AZYGOUS VEIN THROMBOSIS
Discussion Obstruction of the superior vena cava is complication of multiple benign and malignant etiologies, which compress, occlude or invade the SVC. Mediastinal masses, lymphadenopathy, hypercoagulabity of malignancy or other blood dyscrasias are common causes. Benign etiologies include thrombosis from indwelling catheter, fibrosing mediastinitis, vasculitides, benign mediastinal tumors are less common (<20%). Symptoms depends on the acuity of onset and development of collaterals and include facial and upper extremity swelling, cough, hoarsness and dysphagia. Standford et al. propsed classification system (AJR, 1987; 148: 259 -62) for SVC thrombosis. Type 1: Partial occlusion of SVC with patent azygous vein Type 2: Complete occlusion of SVC with patent azygous vein Type 3: Complete occlusion of SVC with reversal of flow in azygous vein Type 4: Complete occlusion of SVC, azygous vein and one or more major caval tributaries
This case represents a Type 4 SVC obstruction, and demonstrates the collateral venous anatomy when the SVC is obstructed below the level of azygous insertion. With a patent azygous vein and the obstruction above the level of the azygous, collateral flow can travel retrograde into the left brachiocephalic vein to accessory hemiazygous vein to azygous vein and then flow antegrade through the distal SVC. With the Type 4 obstruction the collateral circulation is routed to the inferior vena cava or portal circulation by multiple venous plexuses, including: thoracoepigastric vein, mediastinal vein, internal mammary vein, hemiazygous vein, lateral thoracic vein, pericardiophrenic vein, paravertebral vein, intercostal vein, capsular /surface liver vein, bilateral phrenic veins, thoracodorsal scapular vein, superior/inferior epigastric vein, accessory hemiazygous vein. Another intriguing pathway illustrated in this example is the cavo-portal pathway associated with intense opacificaton of the quadrate lobe– a sign with high specificity for SVC obstruction. It is associated with communication of the internal mammary veins with the epigastric veins, which then anastomoses with the peri-umbilical venous channels. Through the recanalized umbilical vein in the falciform ligament, blood flows retrogradely into the left portal vein. The resultant flow and venous stasis is believed to result in the characteristic focal hepatic enhancement. Similar findings are observed nuclear imaging with Tc-99 m sulfur colloid scans, the so-call focal hepatic hot spot sign.
References 1. Collateral Pathways in Superior Vena Caval Obstruction as Seen on CT, Journal of Computer Assisted Tomography, 2001, 25(1): 1 -8 2. Multi-detector row and volume-rendered CT of the normal and accessory flow pathways of the thoracic systemic and pulmonary veins, Radiographics, 2002, 22: S 45 -60 3. The Focal Hepatic Hot Spot Sign, Radiology, 2005; 237: 647 -648. 4. Focal Hepatic Enhancement on Computed Tomography in a patient With a Non-Small Cell Lung Carcinoma, Oncology Imaging, 2001; 184: 189 -191.