Overview of Medical and NonMedical Detox CAPTASA January









































425 -7761")
- Slides: 50
Overview of Medical and Non-Medical Detox CAPTASA January 30, 2015
Practice Gaps- Why are we even talking about this again? v. Medical Detox is severely limited in availability v. Varies greatly in quality and effectiveness v. Some may be appropriate for Non -Medical Detox v. Who ought to get what and why
Objectives of this activity: v Review the options available for Detox v I will provide my experience with Medical detox v Hopefully we can increase the awareness that Detox is essential to prepare a person to receive Treatment v But Detox is not Treatment
“I know I’ve got a tarnished reputation… But Man I can sure think on my toes” Assembly of Dust Bootlegger's Blues
Who Needs Detox? v. Anyone using recently or regularly- who is ready for change v. Using what? - Alcohol, Sedatives and Opiates v. To Start Treatment or Start Over
Some are Ready, Some Not So much
Why bother? v. A Safe Withdrawal from Alcohol and other Drugs v. A Withdrawal that is Humane and Protects Dignity v. Prepare the Patient for Ongoing Treatment Principles of Addiction Medicine 3 rd Ed. Page 612
We do it for them- their the ones with the problem
“Of course an alcoholic ought to be freed from his physical craving for liquor, and this often requires a definite hospital procedure, before psychological measures can be of maximum benefit. ” William D. Silkworth, MD The Doctor’s Opinion
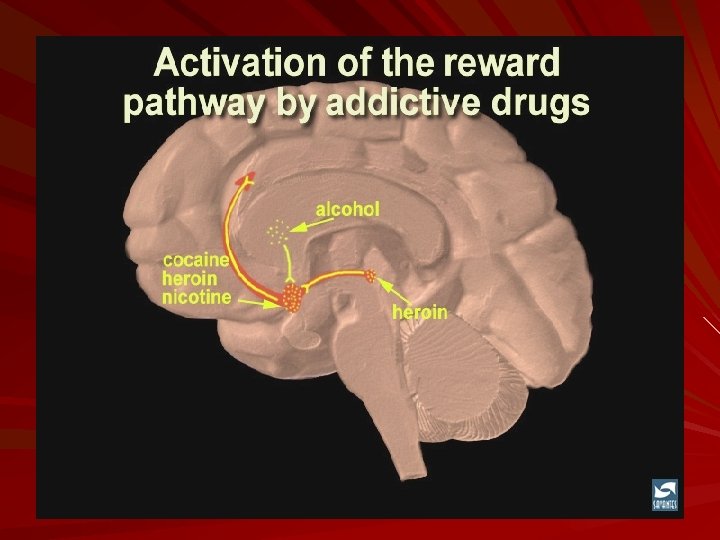
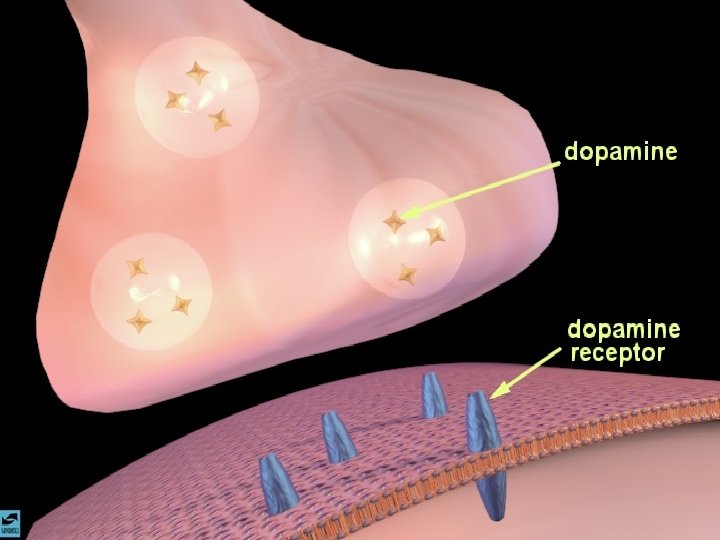
Dopamine Pathways – Pleasure pathways striatum frontal cortex hippocampus alcohol substantia nigra/VTA cocaine nucleus heroin accumbens nicotine amphetamines opiates THC PCP ketamine heroin alcohol benzodiazepines barbiturates
Which drugs need medical detox ? v. Alcohol v. Sedative/hypnotics v. Opiates v. Any that are impacting ability to begin Tx
Most Common forms of Detox v. Nothing v. In a jail cell v. Alone v. Die using v. A few lucky ones get Medical help or a caring Hand
Usual Medical Detox approach v. Benzo’s for Alcohol v. Benzo’s for Benzo’s v. Opiates for opiates
“We live in the age of wonder drugs: first we give the patient the drugs, then we wonder…” Adolph L. Sachs, MD Head of Neurology University of Iowa
Alcoholics Anonymous, page 22 from ‘There is A Solution” Perhaps he goes to a doctor who gives him morphine or some sedative with which to taper off. Then he begins to appear at hospitals and sanitariums. This is by no means a comprehensive picture of the true alcoholic, as our behavior patterns vary. But this description should identify him roughly.
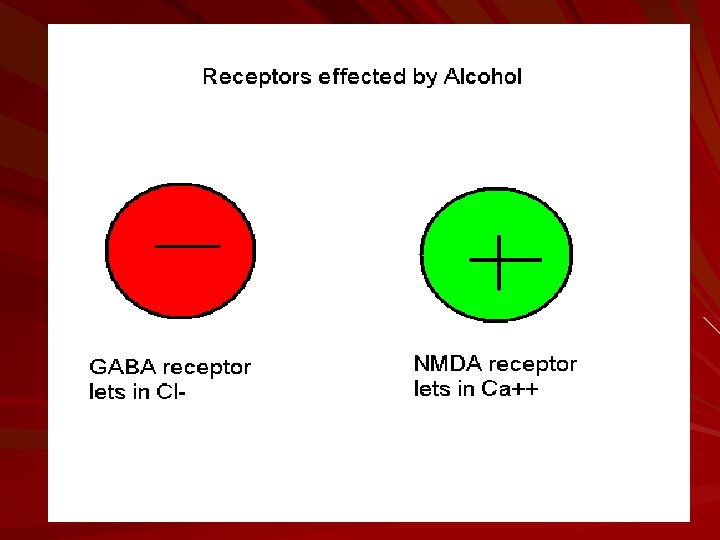
GABA- the down button
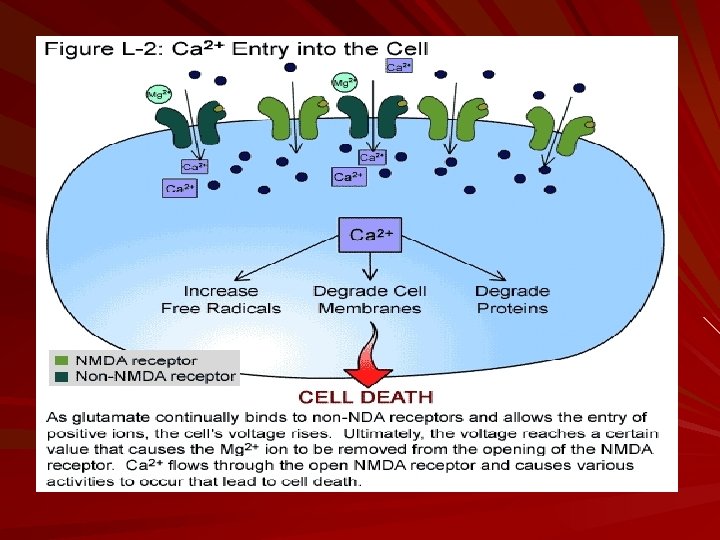
NMDA- the up button
Here’s what I did v. History of Use v. What are they using? How they use it? v. How much, especially in last 7 -10 days v. How long using v. Other medical conditions- High Blood Pressure, Heart Disease, Lung Disease, Seizures, Infections, Past Detox experiences…
My Experience with Benzodiazepines
ASAM Textbook, 3 rd Ed. Page 643 Clinical experience shows that phenobarbital is most useful and effective with polysubstance dependence, high-dose dependence, and in patients with unknown dose or erratic “polyphramacy”
Phenobarb dosage v. Load v. Regular dose taper v. PRN’s based on CIWA score
DAYS 1&2 v Phenobarbital 180 mg PO now, then v Phenobarbital 60 mg PO every 6 hours X 8 doses v Obtain CIWA score every 4 hours v If CIWA score greater than 15, give Phenobarbital 260 mg IM v If CIWA score 8 -15, give Phenobarbital 120 mg PO
DAYS 3&4 v Phenobarbital 60 mg PO every 12 hours X 4 doses v Obtain CIWA score every 6 hours v If CIWA score greater than 15, give Phenobarbital 120 mg PO v If CIWA score 8 -15, give Phenobarbital 60 mg PO
Thiamine is critical for Tx of Alcoholism Thiamine 100 mg IM now, then 100 mg a day x 5 days. Folic acid 1 mg a day for 5 days.
Magnesium Sulfate v Based on Alcohol use and age of Patient v 1 Gm IM every 8 hours v At least 2 doses v Up to 4 for high volume drinkers and those with seizure Hx* v PO Magnesium oxide is poor alternative, limit is 400 mg BID *Magnesium is not for seizures
Clonidine dosage v Clonidine 0. 1 mg PO now, then v Clonidine 0. 1 mg PO every 6 hours X 8 doses, then v Clonidine 0. 1 mg PO every 8 hours X 3 doses, then v Clonidine 0. 1 mg PO every 12 hours X 2 doses v Hold Clonidine if BP less than 90/55
Buprenorphine for High Dose Opiate W/D v Buprenorphine 4 -8 mg SL, on day 2 or 3 v Can repeat dose in 12 hours v Cramps, Sweats and Diarrhea are good guides to effect v Rarely use more than 12 mg in 24 hours v Rarely use more than 4 days v Always use plain Buprenorphine and use SL observed doses
Phenobarb equivalents v 30 cc 100 proof alcohol = 30 mg v. Xanax 1 mg = 30 mg v. Ativan 2 mg = 30 mg v. Klonopin 2 mg = 30 mg v. Valium 10 mg = 30 mg v. Librium 25 mg = 30 mg
What about Delirium? v. This is where dehydration is important v. First load with Phenobarb and push dose v. Avoid anticholenergic drugs v. Risperdal 2 mg + Ativan 2 mg PO v. Haldol 5 mg +Ativan 2 mg+ Benadryl 50 mg all IM
“The Art of Medicine consists in amusing the Patient while Nature cures the Disease. ” Voltaire
Non-Medical Detox v Works for a motivated individual v Need informed, caring staff v Need quick Medical help if things go sideways v But it’s a viable option and many do get well this way
Non-Medical Detox v Individuals undergoing detoxification are in the midst of a personal and a medical crisis v That can facilitate a real opportunity for them to acknowledge their problem and become willing to consider a change v Research indicates that detoxification is often followed by reduced drug-use and treatment-seeking behavior
Social Detox Pluses v Costs! Much less than Medical Model Detox v But that does not mean lower rates of effectiveness or lower standards of care v The level of personal care by staff at a social model detox program is frequently found to be higher because most people working in these facilities are also in recovery v So they can empathize with the people in treatment.
Here’s what they do… v. History of Use v. What are they using? How they use it? v. How much, especially in last 7 -10 days v. How long using v. Other medical conditions- High Blood Pressure, Heart Disease, Lung Disease, Seizures, Infections, Past Detox experiences…
What about Seizures? v Don’t panic v Most likely with Benzo’s and/or Alcohol v Can occur up to a week after last use, but usually in first 72 hours v Rarely life threatening v Get them safely to floor or in bed v On side, either is fine v Time it and watch their breathing
What are the DT’s v They aren’t what most folks think. v Most of the time when someone says they have or have had DT’s they didn’t v DT’s are fatal 10% of the time, even with treatment at a hospital v They are most common with Alcohol, but occur with mixtures as well v Change in Mental Status, plus unstable vital signs
What Delirium Is v. This is important! v. Confused v. Combative v. Unstable Vital signs v. Need Medical Care quickly
When would transfer to Medical Detox be needed? v Change in mental status v Hallucinations v Fever or rise in temperature v Significant dehydration v Significant increases or decreases in blood pressure and heart rate v Upper and lower gastrointestinal bleeding
Alcoholics Anonymous, page 64 from “How It Works” …for we have been not only mentally and physically ill, we have been spiritually sick. When the spiritual malady is overcome, we straighten out mentally and physically.
Neurophysiology of Recovery v. Extended withdrawal for weeks v. Structural and functional brain abnormalities v. Gradual normalization over first recovery decade v. Addiction may sensitize for mental dysfunction
Greg L Jones, MD Kentucky Physicians Health Foundation gregj@kyrecovery. org (502)425 -7761