Surgical Care Improvement Project Prevention of Postoperative Venous

 is the")




- Slides: 7
Surgical Care Improvement Project Prevention of Post-operative Venous Thromboembolism Team Membership Department of Surgery, Nursing, General Medicine, Pharmacy, CCE
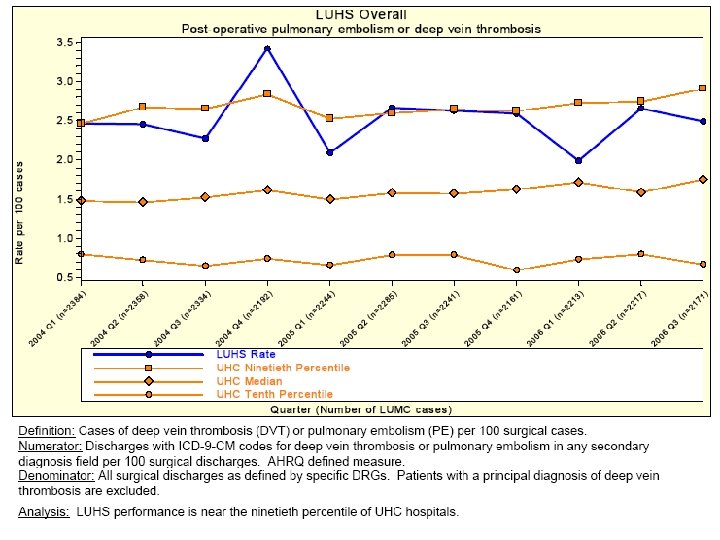
Opportunity Statement • Venous thromboembolism (VTE- deep vein thrombosis and pulmonary embolism) is the most common preventable cause of death following surgery. • The rate of post-operative VTE at LUMC (2 -3%) is at the 90 th percentile compared to other Academic Medical Centers (UHC data)
Project Goals • Achieve a 50% reduction in the occurrence rate of post-operative venous thromboembolism
Most Likely Causes for Current Opportunity • Surgical patients are not routinely assessed and stratified for VTE risk • Wide variability in use of prophylactic methods • Variable awareness of national, evidence-based guidelines* • Under utilization of pharmacologic prophylaxis (heparin) * Geerts, WH et al. Prevention of venous thromboembolism: The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004; 126: 338 s-400 s.
Solutions Implemented • Developed and piloted Risk Assessment Tool in the Department of Surgery • Developed guideline for selection of appropriate VTE prophylaxis for surgical patients • Revised current standing post-operative orders in the Department of Surgery, Orthopaedics and Neurosurgery to include heparin or enoxaparin.
Next Steps • Ongoing monitoring of risk assessment tool use • Continued education of physicians and nursing staff • Continue comparison with UHC data