Zen Ahmad dr Sp PDKP TempatTanggal Lahir Palembang

Zen Ahmad, dr. , Sp. PD-KP Tempat/Tanggal Lahir : Palembang, 8 Maret 1962 Pekerjaan : Staf Penyakit Dalam RS Dr. M. Hoesin/FK UNSRI Riwayat Pendidikan : Internis tahun 2000 Konsultan Paru tahun 2005 Bandung Integrated Respiratory Care IV | 16– 18 September 2016

Update management patient with cough Zen Ahmad FK UNSRI/RSMH Palembang

Defenition and terminology �Cough is a forced expulsive manoeuvre, usually against a closed glottis and which is associated with a characteristic sound �Acute cough and Chronic cough • Acute: a cough lasting less than 3 weeks • Chronic: a cough lasting more than 8 weeks �Dry cough and Productive cough
")
Mechanism of cough Stimulation of mechano-or chemoreceptors respiratory passages or stretch receptors in lungs) (throat, Afferent impulses to cough centre (medulla) Efferent impulses via parasympathetic & motor nerves to diaphragm, intercostal muscles & lung Increased contraction of diaghramatic, abdominal & intercostal (ribs) muscles noisy expiration (cough)

Diagnostic of cough �Anamnestic �Physical examination �Radiologic § § § Chest radiograph CT scan Sinus imaging �Bronchoscopy �Spirometry �Bronchial provocation testing �Echocardiogram � 24 th esophageal p. H monitoring

Acute cough � Acute cough is the commonest new presentation in practice care, most commonly associated with viral URTI � Acute cough is normally benign and self-limiting � It is the commonest symptom associated with acute exacerbations and hospitalisations with asthma and COPD � Indications for further investigation include haemoptysis, prominent systemic illness, suspicion of inhaled foreign body, suspicion of lung cancer. � Patients report benefit from various over-the-counter preparations; there is little evidence of a specific pharmacological effect

Acute cough

Acute cough

Treatment of acut cough Viral infection Inflamation Airway sensory receptors Central Nervous system Antiviral • Neuramidase inhibitors • Amantadin Anti inflamatory • NSAID • Corticosteroid Peripherally acting • Local anaesthetic • Demulcents • Expectorants, mucolytics • Cooling, warming agents • VR 1 antagonist Centrally acting • Opioids • Dextromethorpan • Sedatives Respiratory muscle Cough

Chronic cough �Cough accounts for 10% of respiratory referrals to secondary care. �Most patients present with a dry or minimally productive cough �Decrement in quality of life is comparable with severe COPD �The presence of significant sputum production usually indicates primary lung pathology �In chronic cough a heightened cough reflex is the primary abnormality

Chronic cough

Chronic cough �Commonest causes of chronic cough in adults § UACS due to a variety of rhinosinus conditions § Asthma § GERD § NAEB �In 5 prospective studies from the western, these 3 diseases singly/combination caused 92 -96% of the chronic coughs in non-smokers who were not on ACE inhibitors and who had normal CXR �The prevalence of NAEB as a cause outside of the western hemisphere has ranged from 0 to 33%

Investigative protocol management of chronic cough Initial clinical assessment History; PE; Spirometry; Reversibelity; CXR Yes Possible diagnosis ? Sequential 8 week trial for the commonest causes of cough 8 week trial of appropriate th/ Treatment successful No No Other possible diagnosis No Yes Continue th/ 8 week trial of appropriate th/ Yes Th/ trial success No Investigational protocol

Treatment of chronic cough � 1 st generation antihistamine-decongestant �Inhaled bronchodilator �Inhaled corticosteroid �A leukotriene receptor antagonist �Anti-reflux therapy • Acid suppression therapy • Pokinetic therapy

Treatment of chronic cough �Antitussive, incorporates with mucolytic and/or inhibitory effects on the cough reflex itself § § This therapy only reduce the frequency/intensity of coughing on a short-term basis These drugs do not resolve the underlying pathophysiology responsible for the coughing “There is no evidence that this therapy can prevent coughing” �Because of the success of specific therapy, suppressant therapies are necessary only in specific situations § § § When the etiology of cough is unknown When specific therapy requires a period of time before it can work When specific therapy will be ineffective (ex: inoperable lung cancer)

Treatment of chronic cough � Some protussive agents are effective in increasing cough clearance (amiloride in CF; hypertonic saline in bronchitis) but their longterm effectiveness has not been established � In acute or chronic cough not due to asthma, albuterol is not recommended � In patients with neuromuscular impairment, protussive pharmacologic agents are ineffective and should not be used � In chronic bronchitis, agents that have been shown to alter mucus characteristics are not recommended for cough suppression. � In cough due to URI or chronic bronchitis, the only inhaled anticholinergic agent that is recommended for cough suppression is ipratropium bromide

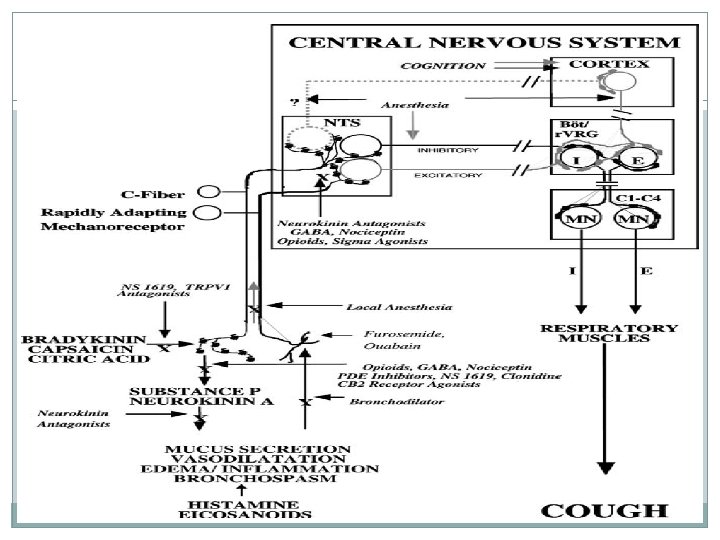
Action of Antitussives at the cough receptor RAR, rapidly adapting receptor; NK, neurokinin; LTD 4, leukotriene D 4; VR 1, vanilloid receptor; GABA, g-aminobutyric acid; NTS, nucleus tractus solitarius.

Mucolytic and expectorant � 95% water, 2% glycoproteins Mucolytic Expectorant � Gel layer-high viscosity from goblet cells � Sol layer – low viscosity from sub mucosal glands � Goblet and sub-mucosal glands increase secretion when irritated � Vagal stimulation will also increase sub-mucosal gland secretion

Mucolytic • Increased Mucus Production § § § Viscosity of mucus Ciliary effectiveness Mucus plugs Airway Resistance Infections • Mucolysis is needed in diseases in which there is increased mucus production § § Cystic Fibrosis COPD; Asthma Bronchiectasis Pneumonia

Mucolytic � � � � N-Acetlycysteine Erdosteine Carbocistein Bromheksin Ambroxol Pulmozym (Dornase Alpha or DNAse) Sodium bicarbonat

Mucolytic Sodium Bicarb N-Acetylcysteine Sodium Bicarb

Mucolytic Erdostein Vestein + Vostrine + Vectrine + Woods expec Bromhexine Ambroxol + + Bisolvon extra + Broncholit N-acetyl cystein + + + Epexol + Fluimucil Mucohexin Guaiphe nesine + Transbroncho Edotin Carbo cistein + +

Side effect of mucolytic Rare �Nausea �Vomiting �Stomach pain �Diarrhea �Headache �Vertigo �Allergic reaction

Expectorant �Guaifenesin �Terpin hydrate �Gliseril guaikolat �Ammonium klorida �Succus liquiritiae �Ipekak

Antitussive � Obat penekan atau penghambat batuk � Central antitussive Dependent � Opioid Codeine Independent � Levorphanol drivat: Dextromethorphan � Amido: Pentoxyverine � Piperidin: Cloperastine � Morpholine: fominoben , Promolate � Eprazinone , zipeprol � Peripheral antitussive local anesthesia action: narcotine, benzonatate Alleviative action: extractum glycyrrhizae liquidum

Treatment of chronic cough �Relatively few drugs are effective for non-specific suppression of cough �It is recommended that suppressants be guided by specific knowledge of the disorder causing cough § § § Mucolytic agents are not consistently effective to ameliorate cough in patients with bronchitis Zinc preparations are not recommended for cough due to cold Peripheral (levodropizine, moguisteine), central antitussive (codeine, dextromethorphan) can be useful in chronic bronchitis but have little efficacy in patients with cough due to URI In patients with chronic or acute bronchitis, peripheral cough suppressants, are recommended for the short-term symptomatic relief of coughing Opioids are useful in lung cancer

Codeine �One of the strongest cough suppressants known �It suppresses coughing by direct action on the cough centre in the medulla oblungata, and also decreases the rate and/or tidal volume of respiration. �Increases tolerance to pain, decreasing discomfort, but the pain still is apparent to the patient �Is combined with acetaminophen (Tylenol) or aspirin for more effective pain relief.

Codeine �Dangerous side effects can occur when alcohol is combined with codeine Codein Phenyltoloxamine Guaiphenesin Codipront + + Codipront cum expec + + Coditam + Paracetamol + +

Codeine; side effects � Light-headedness � Dizziness � Nausea � Vomiting � Respiratory depression � Sedation � Tolerance and physical dependence with frequently repeated administration � Euphoria � Allergic reactions, constipation, abdominal pain, rash and itching � Suppress secretion of bronchial gland movement of cilia

Dextromethorphan �Non-sedating opiate and has been shown to suppress acute cough �Suppresses the cough reflex by a direct action on the cough center in the medulla �There is a dose response, and maximum cough reflex suppression occurs at 60 mg and can be prolonged �Care must be taken in recommending dextromethor- phan at higher doses since some combined preparations contain other ingredients such as paracetamol

Dextromethorphan � Onset and duration of action: Usually within one-half hour, after 10 - to 20 -mg doses every 4 hours or 30 mg every 6 to 8 hours � Elimination: Primarily renal (excreted as unchanged dextromethorphan and demethylated metabolites, including dextrorphan) � Risk-benefit should be considered in this conditions § Asthma (impair expectoration; increase airway resistance) § COPD, Productive Cough (inhibition of cough reflex may lead to retention of secretions ) § DM (some DXM products contain sugar and impair blood glucose control) § Hepatic function impairment (metabolism of DXM may be impaired) § Respiratory depression (DXM may make this condition worse)

Dextromethorphan: Side effect �Dizziness �Drowsiness �Nervousness �Restlessness �GI problems: Nausea; Vomiting; Stomach pain; Constipation �Headache �Toxic psychosis (hyperactiv, visual/auditory hallucinations) has been reported after ingestion of 300 mg or more �Respiratory depression (very high doses) �DXM dependence, especially in high doses prolonged use }

Dextromethorphan Dextro metorpha n Phenylpro panolamin e Actiped + Alpara + Alco plus DMP + Valved DM + Tuzalos + + Sanaflu + + + Brompheni ramine Pseudo Triproli epedrin dine + Chlorphe Parase niramin tamol + + + + + Decolgen Panadol + Lacoldin + + + Dextral + + +

Sedative antihistamines �First generation antihistamines with sedative properties suppress cough but also cause drowsiness �They may be a suitable treatment for nocturnal cough �Brompheniramine �Difenhidramin

Bromhe xine Bromph enirami ne Actiped Dextro Pseudoe Triproli metorph phedrin dine an e + Actiped expec Alco plus DMP Woods expec Benadryl DMP Bisolvon Decolgen + + + + Guaiphe nesine +
- Slides: 36