z Dr Abeera SarfrazDr Muhammed Zubair URETER SUPRA

z Dr Abeera Sarfraz/Dr Muhammed Zubair URETER & SUPRA RENAL GLANDS

z Introduction § The two ureters are muscular tubes that extend from the kidneys to the posterior surface of the urinary bladder. The urine is propelled along the ureter by peristaltic contractions of the muscle coat, assisted by the filtration pressure of the glomeruli. Each ureter measures about 10 in. (25 cm) long and resembles the esophagus (also 10 in. long) in having three constrictions along its course: where the renal pelvis joins the ureter, where it is kinked as it crosses the pelvic brim, and where it pierces the bladder wall.
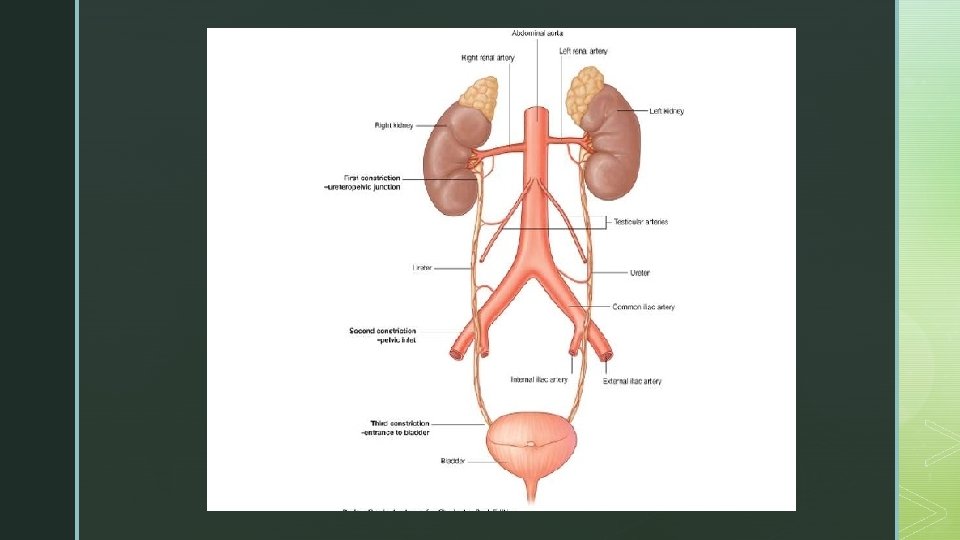

z Description & Course § The renal pelvis is the funnel-shaped expanded upper end of the ureter. It lies within the hilum of the kidney and receives the major calyces. The ureter emerges from the hilum of the kidney and runs vertically downward behind the parietal peritoneum (adherent to it) on the psoas muscle, which separates it from the tips of the transverse processes of the lumbar vertebrae. It enters the pelvis by crossing the bifurcation of the common iliac artery in front of the sacroiliac joint. The ureter then runs down the lateral wall of the pelvis to the region of the ischial spine and turns forward to enter the lateral angle of the bladder.

z Relations, Right Ureter § Anteriorly: § The duodenum, the terminal part of the ileum, the right colic and ileocolic vessels, the right testicular or ovarian vessels, and the root of the mesentery of the small intestine. § Posteriorly: § The right psoas muscle, which separates it from the lumbar transverse processes, and the bifurcation of the right common iliac artery

z Relations, Left Ureter § Anteriorly: The sigmoid colon and sigmoid mesocolon, the left colic vessels, and the left testicular or ovarian vessels. § Posteriorly: The left psoas muscle, which separates it from the lumbar transverse processes, and the bifurcation of the left common iliac artery. § Medially: The inferior mesenteric vein

z Blood Supply § The arterial supply to the ureter is as follows: § upper end, the renal artery; § middle portion, the testicular or ovarian artery; § and in the pelvis, the superior vesical artery. § Venous blood drains into veins that correspond to the arteries. § Lymph Drainage

z Lymphatic Drainage § § § The lymph drains to the lateral aortic nodes and the iliac nodes. Nerve Supply The nerve supply is the renal, testicular (or ovarian), and hypogastric plexuses (in the pelvis). Afferent fibers travel with the sympathetic nerves and enter the spinal cord in the first and second lumbar segments.

z Clinical Notes § Traumatic Ureteral Injuries to the ureter are rare because of its protected position and small size. Most injuries are caused by gunshot wounds and, in a few individuals, penetrating stab wounds. Because the ureters are retroperitoneal in position, urine may escape into the retroperitoneal tissues on the posterior abdominal wall. § Ureteric Stones There are three sites of anatomic narrowing of the ureter where stones may be arrested, namely, the pelviureteral junction, the pelvic brim, and where the ureter enters the bladder. Most stones, although radiopaque, are small enough to be impossible to see definitely along the course of the ureter on plain radiographic examination. A CT scan and an intravenous pyelogram are usually necessary. The ureter runs down in front of the tips of the transverse processes of the lumbar vertebrae, crosses the region of the sacroiliac joint, swings out to the ischial spine, and then turns medially to the bladder.

z § The renal pelvis and the ureter send their afferent nerves into the spinal cord at segments T 11 and 12 and L 1 and 2. In renal colic, strong peristaltic waves of contraction pass down the ureter in an attempt to pass the stone onward. The spasm of the smooth muscle causes an agonizing colicky pain, which is referred to the skin areas that are supplied by these segments of the spinal cord, namely, the flank, loin, and groin. When a stone enters the low part of the ureter, the pain is felt at a lower level and is often referred to the testis or the tip of the penis in the male and the labium majus in the female. Sometimes, ureteral pain is referred along the femoral branch of the genitofemoral nerve (L 1 and 2) so that pain is experienced in the front of the thigh. The pain is often so severe that afferent pain impulses spread within the central nervous system, giving rise to nausea.

z § Bifid Ureter In bifid ureter, the ureters may join in the lower third of their course, may open through a common orifice into the bladder, or may open independently into the bladder. In the latter case, one ureter crosses its fellow and may produce urinary obstruction. The cause of bifid ureter is a premature division of the ureteric bud. Cases of double pelvis and double ureters may be found by chance on radiologic investigation of the urinary tract. They are more liable to become infected or to be the seat of calculus formation than a normal ureter. § Megaloureter may be unilateral or bilateral and shows complete absence of motility. The cause is unknown. Because of the urinary stasis, the ureter is prone to infection. Plastic surgery is required to improve the rate of drainage. § Postcaval Ureter The right ureter may ascend posterior to the inferior vena cava and may be obstructed by it. Surgical rerouting of the ureter with reimplantation of the distal end into the bladder is the treatment of choice.

z SUPRARENAL GLAND § The two suprarenal glands are yellowish retroperitoneal organs that lie on the upper poles of the kidneys. They are surrounded by renal fascia but are separated from the kidneys by the perirenal fat. Each gland has a yellow cortex and a dark brown medulla. § The cortex of the suprarenal glands secretes hormones that include mineral corticoids (concerned with the control of fluid and electrolyte balance), glucocorticoids (concerned with the control of the metabolism of carbohydrates), fats, proteins, and small amounts of sex hormones (which probably play a role in the prepubertal development of the sex organs). The medulla of the suprarenal glands secretes the catecholamines epinephrine and norepinephrine.

z § Location and Description The right suprarenal gland is pyramid shaped and caps the upper pole of the right kidney. It lies behind the right lobe of the liver and extends medially behind the inferior vena cava. It rests posteriorly on the diaphragm. The left suprarenal gland is crescentic in shape and extends along the medial border of the left kidney from the upper pole to the hilus. It lies behind the pancreas, the lesser sac, and the stomach and rests posteriorly on the diaphragm.

§ z. Blood Supply § Multiple arteries supply each gland. The three typical vessels are a superior suprarenal artery (a branch of the inferior phrenic artery), a middle suprarenal artery (a branch of the aorta), and an inferior suprarenal artery (a branch of the renal artery). A single vein emerges from the hilum of each gland drains into the inferior vena cava on the right and into the renal vein on the left. § Lymph Drainage § The lymph drains into the lateral aortic nodes. § Nerve Supply § Preganglionic sympathetic fibers derived from the splanchnic nerves supply the glands. Most of the nerves end in the medulla of the gland.

z Clinical Notes § Cushing Syndrome Suprarenal cortical hyperplasia is the most common cause of Cushing syndrome, the clinical manifestations of which include moon-shaped face, truncal obesity, abnormal hairiness (hirsutism), and hypertension. If the syndrome occurs later in life, it may result from an adenoma or carcinoma of the cortex. § Addison Disease Adrenocortical insufficiency (Addison disease), which is characterized clinically by increased pigmentation, muscular weakness, weight loss, and hypotension, may be caused by tuberculous destruction or bilateral atrophy of both cortices.

§z Pheochromocytoma, a tumor of the medulla, produces a paroxysmal or sustained hypertension. The symptoms and signs result from the production of a large amount of catecholamines, which are then poured into the bloodstream. Because of their position on the posterior abdominal wall, few tumors of the suprarenal glands can be palpated. CT scans can be used to visualize the glandular enlargement. However, when interpreting CT scans, remember the close relationship of the suprarenal glands to the crura of the diaphragm. § Surgical Significance of Renal Fascia The suprarenal glands, together with the kidneys, are enclosed within the renal fascia. However, the suprarenal glands lie in a separate compartment, which allows the two organs to be separated easily at operation.
- Slides: 16