Year 4 Monash University Bendigo Regional Clinical School

Year 4 Monash University Bendigo Regional Clinical School

� Definition � Assessment � First Aid � Initial management � Long-term management � Non-accidental injury � Prevention of burn injuries

� Be able to assess the extent and thickness of a burn on a child (or an adult) � Know how to dress a burn and provide analgesia appropriately � Know the principles of fluid resuscitation after a burn injury And hopefully a whole lot more!
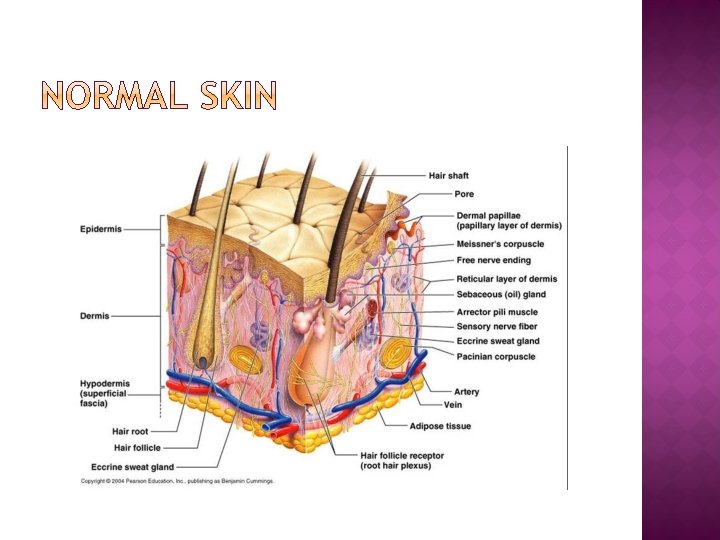

� Loss of Skin or Mucosa due to Thermal, Chemical or Mechanical injury. � May extend to a variable thickness within the skin or mucosa � May extend over a variable extent � May not be visible externally �e. g. Airway burns Oesophageal burns � Outcome at site of burn depends largely on depth of burn

� Superficial Burn �Epidermal loss only �Erythema followed by desquamation � Partial Thickness �Superficial partial Involves dermis Blisters �Deep partial Some deep epithelial elements remain � Full Thickness burn


Red Blistered or shiny and moist Blanches with light touch Painful Heals in <10 days if no infection

Pale or deep red mottled “tartan” appearance Painful Doesn’t blanch with pressure Typically moist
 Leathery and non-blanching")
Pale or charcoal Insensate in the middle (pain at the edges) Leathery and non-blanching to touch Doesn’t bleed on pin prick Constricts deep tissues if circumferential

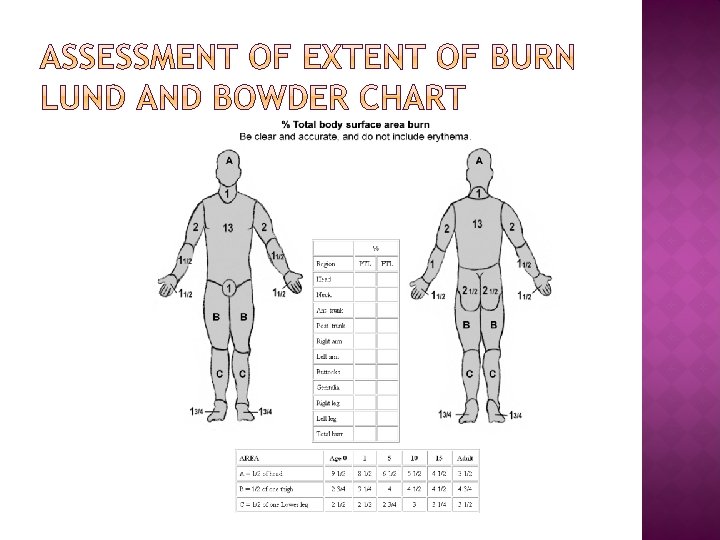
The palm of the patient’s hand is approx 1% of TBSA

� Remove the patient from the source of the burn � Remove hot, burnt, constrictive or contaminated clothing � Cool the burn (keeping the patient warm) � Cover the burn Clean, dry cloth �Glad wrap �

� ABC �Beware stridor in burns to face or chest � Assessment of thickness and extent of burns � ? Escharotomies � Continue First Aid, take “AMPLE” history � Debridement and Dressings � Analgesia � IV access and fluid resuscitation � Tetanus toxoid � Nutrition ? NG tube � ? Transfer to burns centre


Indications for emergency escharotomy are the presence of a circumferential eschar with one of : • Vascular compromise of the extremities or digits • Respiratory compromise due to circumferential torso burns If unsure, measure compartment pressures Capillary refill in distal limb • Abdominal compartment syndrome If still in doubt DO ESCHAROTOMY Anaesthesia not required Stay in mid-lateral plane
 �Maintain a moist wound")
� Principles �Minimize opportunities for bacterial contamination/growth and invasion (debridement) �Maintain a moist wound environment �Avoid substances which are toxic to tissues which are potentially viable (some historical dressings) �Enable re-evaluation as necessary �Be cost and time effective for both staff and patient

� Minimize opportunities for bacterial growth and invasion � Remove all loose dead devascularised skin at first presentation prior to dressing � Clean with Chlorhexidine to remove gross dirt � De-roof blisters when they are no longer tense � Surgically debride deep partial and fullthickness burns at the earliest convenient opportunity

Braithwaite and Silver’s knives Versajet

� Creams, Solugel – A liquid hydrogel. Needs thorough washing off and reapplication 4 x per day. Used for face and perineum � Low Adherent dressings Mepital (silicone-based dressing) Uni-tulle/Bactigras � Silver Lotions and Gels Products Acticoat/Acticoat 7 (Needs activation by sterile water and cover with Intrasite conformable to maintain moisture) Aquacel Ag with intrasite/tegaderm over it (also needs to be moist) SSD Causes difficulty assessing burn depth and is toxic to the cornea. Appropriate for full-thickness burns (not on face) pending excision � Glad Wrap

� Scalds in children classically get deeper over the first 24 -48 hours. � Once depth is established then care plan can be developed � Assessment of burn depth requires experience and expertise � Photographs can be helpful in ED � When in doubt �Clean, dress simply, admit and review by surgical consultant in am �Call consultant surgeon to review
 � Cover the burn (once it")
� Cool the burn (but not the patient) � Cover the burn (once it has been cleaned and loose skin debrided) � Distraction (play therapist/video games) � Analgesic ladder �Topical Lignocaine gel to aid gentle debridement �Oral Paracetamol +/- codeine or endone �Parenteral IV (Not IM or SC as absorption is unpredictable and risk under and overdose in the same patient)

� Try and avoid burnt tissue �Difficult to secure �Risk of tight bandages with burn swelling � Consider need for “different” routes �Saphenous vein cutdown �Intraosseous needle �Central lines

� � Various “formulas” Maintenance fluid 4 ml/kg/hour to 10 kg � 2 ml/kg/hr 10 -20 kg � 1 ml/kg/hr >20 kg � � Water and sugar and Na and K Replacement of Existing burn losses FROM THE TIME OF THE BURN � Approx 4 ml/kg/%burn/24 hrs (excluding 1 st degree burn) N. Saline or Hartmann’s solution � 50% of replacement given in first 8 hours post-burn, � Remainder over next 16 hours post burn � � Replacement of anticipated on-going burn losses � � Consider possibility of Inc K from burnt tissue Ongoing re-assessment of intravascular volume i. e. IDC and hourly urine measures aim for 1 ml/kg/hr minimum in children � Consider myoglobinuria from burnt muscle in deep burns or ischaemic muscle �

� Tetanus �Burns toxoid are tetanus prone wounds � Nutrition �Nutrition requirements increase according to the size of the burn �For burns >10% will need nutitional supplementation. Consider use of NGT � Maintaining � Role Blood Glucose Levels of Antibiotics �(there isn’t one unless…. . )
 burns over 5% BSA Partial-thickness (second-degree) burns over 10% BSA �")
� Full-thickness (third-degree) burns over 5% BSA Partial-thickness (second-degree) burns over 10% BSA � Any full-thickness or partial-thickness burn involving critical areas (e. g. , face, hands, feet, genitals, perineum, skin over any major joint), as these have significant risk for functional and cosmetic problems � Circumferential burns of the thorax or extremities � Significant chemical injury, electrical burns, lightning injury, coexisting major trauma, or presence of significant preexisting medical conditions � Presence of inhalation injury

� Skin Grafting � Temporary skin substitutes � Skin culture � Scar management � Scar contractures and scar hypertrophy

• A split thickness of skin is taken from a suitable donor site • The skin is meshed in a mesher • Skin placed “shiny-side-down” on the wound • Graft secured • Immobilise and elevate graft with topical pressure 5 – 7 days minimum

� “Classic” Cases �Cigarette burns �Perineal burns �Hot water in the bath �Burns with identifiable “brand” impression e. g. iron � Considerations �Implausible story that is inconsistent �Other signs of injuries of different ages �Other presentations with serious injury/ingestions/drowning etc

� Consider burn demographic � Home safety � Role of change in escalating risk for burn injury �Developmental �Seasonal �Location/Carers

� Electrical burns � Blast injury � Caustic ingestion � Carbon monoxide poisoning

� Burns largely preventable � Early action mitigates the severity of the outcome � Close follow-up and attention to detail is vital � Team care is important � If you don’t know ASK
- Slides: 33