YAKIMA NEIGHBORHOOD HEALTH SERVICES OUR MISSION IS TO

YAKIMA NEIGHBORHOOD HEALTH SERVICES OUR MISSION IS TO PROVIDE ACCESSIBLE, AFFORDABLE, QUALITY HEALTH CARE, PROVIDE LEARNING OPPORTUNITIES FOR STUDENTS OF HEALTH PROFESSIONS, END HOMELESSNESS AND IMPROVE QUALITY OF LIFE IN OUR COMMUNITIES.

YAKIMA NEIGHBORHOOD HEALTH SERVICES PARTNERING IN OUR COMMUNITIES YNHS – Sunnyside Campus Henry Beauchamp Community Center Comprehensive Health Services Neighborhood Connections Medical/Dental Granger Dental Supportive Housing Neighborhood Connections HRC Granger Medical Sunnyside Walmart Plaza Lower Valley Mobile Unit

Homel 2018 PROFILE HEALTH CARE AND HOUSING 2018 Homeless Profile 2018 ALL YNHS Patients ess Se rvic 14% of es = ou 90% of r Business our Tim e! All Primary Care Patients 23, 514 Homeless Patients Primary Care Visits (medical, dental, mental health) 91, 734 Primary Care Visits (medical, dental, mental health) Permanent Supportive Housing Youth Served at The Space Enrolled WIC Clients Affordable Care Act Applications 68 7, 046 4, 433 Medical Respite (Average 19. 7 days each) 3, 221 16, 517 77 households 120 people 72 People 1, 418 nights Housing & Essential Needs (HEN) 278 households Basic Needs (Employment, 884

HOW YNHS ENTERED THE HOUSING WORLD Ø YNHS PROVIDERS SPEAK – “IF YOU WANT US TO MAKE A DIFFERENCE IN THE HEALTH OF THESE PATIENTS, YOU NEED TO HELP GET A ROOF OVER THEIR HEADS… “ 2006 – CONTINUUM OF CARE RESTRUCTURE Ø SHELTER AND HOUSING PROVIDER DISSOLVES Ø HUD MCKINNEY PROVIDERS WITHDRAW Ø NEED FOR MEDICAL RESPITE CARE EMERGES

Yakima County Homeless Trends - Housed and Unsheltered 1400 1200 1000 1168 1108 Housed 827 943 852 712 800 616 600 516 410 400 228 83 Unsheltered 60 53 47 47 72 64 79 2012 2013 2014 2015 2016 2017 0 2011 2018 • No single cause of homelessness – other than a lack of stable housing • A strong continuum of services includes: • Street outreach and services • Emergency Shelter (including DV) and Supportive Housing • Permanent Supportive Housing • Medical Recuperative Respite Care • Medical, dental, behavioral health services • Supportive Housing and Supportive Employment 5

(slid e Hom courtesy e of Ya less Net of wo kima Cou rk nty)

(slid e Hom court e of Y eless N sy of akim e a C twork oun ty)

2011 HHS PROMISING PRACTICE YAKIMA’S SUPPORTIVE HOUSING COLLABORATION • YNHS • Triumph Treatment Services • YWCA • Yakima Housing Authority • Building Changes • County Government • Private Landlords SHARED LEARNING TRAUMA INFORMED CARE / HOUSING FIRST / HARM REDUCTION/ MOTIVATIONAL INTERVIEWING • STANDARDIZED INTAKE • ASSESSMENT TOOL • REGULAR INTERVALS • IDENTIFIES BARRIERS • DEVELOPS PLAN

Housing & Health Partnerships Continuum of Care / Coordinated Entry SAMHSA Grant to Benefit Homeless Individuals Supportive Housing / Supported Employment HCH Street Outreach Primary Care *Medical *Dental *Behavioral Health *Pharmacy HEN / ABD Health Home

Drink the Kool-Aid Housing is Health Care Improving rate of successful connection to primary care Outcomes Tied to the IHI Triple AIM Increasing rate of compliance with care plans Improvement in chronic disease measures (e. g. A 1 c scores, BP measure) Reduction in communicable disease (e. g. TB, STDs, Hep C) Reduction in behavioral health crisis episodes Medications are better managed More likely to obtain and maintain employment or education Greater success for recovering SUD recovering patients in supportive housing
 Medically fragile as determined")
Chronically homeless YNHS Supportive Housing Eligibility criteria (very health focused) Medically fragile as determined by PRISM scores or health home eligibility AND Capable of activities of daily living CONTRIBUTING FACTORS Dx of mental health, sud, or co-occurring disorder Staff knowledge from additional medical or social determinants assessments

• Eligibility Criteria for Medical Respite: • Acute medical condition • Living on Streets or in Emergency Shelter • Independent in Activities of Daily Living (ADLs) • Continent • No IV Lines Medical Recuperative Respite Care for homeless not sick enough to be in the hospital, and for those being discharged from the hospital but not well enough to be back on the streets. • Can administer own medications
")
72 patients stayed 1, 418 Days- Here’s Why (Average 19. 7 days per Patient) Length of Stay People Reason for Respite One Week or Less 15% Flu, Cellulitis, Pneumonia, Bronchitis, Acute Asthma, COPD One to Two Weeks 28% Wound care, Gunshot wound, Esophageal varices, Hip Replacement, Uncontrolled Diabetes Three to Four Weeks 22% Medication Assisted Treatment Induction (Suboxone), Neck Wound, Gunshot Wound, Abdominal Abscess, Hernia Repair Four Weeks or Longer 35% Adult Failure to Thrive, Dementia, Acute Liver Failure, Frostbite, Abscess, Diabetic Foot Ulcers, Cellulitis

2018 PSH and Respite Participants • Housing: • 123 Participants • Average Length of Stay • 565 (leavers) • 567 (stayers so far) Why they Left Us: • 73% left for permanent housing • 6% died • 20% returned to homelessness • Medical Respite Care: • 72 Patients • Average Length of Stay 19. 7 Days • Range 3 – 90 days Why they Left Us: • 20% left for permanent housing • 3% died • 69% returned to homelessness

Respite staff closely aligned with CHC staff • Respite Staff: • Registered Nurse • Behavioral Health Specialist • Case Manager • Housing Specialist • Neighborhood Connections (HCH Clinic): • Family Nurse Practitioner • Dentist • Health Insurance Navigator • Health Home Care Coordinator • Supportive Housing / Supported Employment Specialists

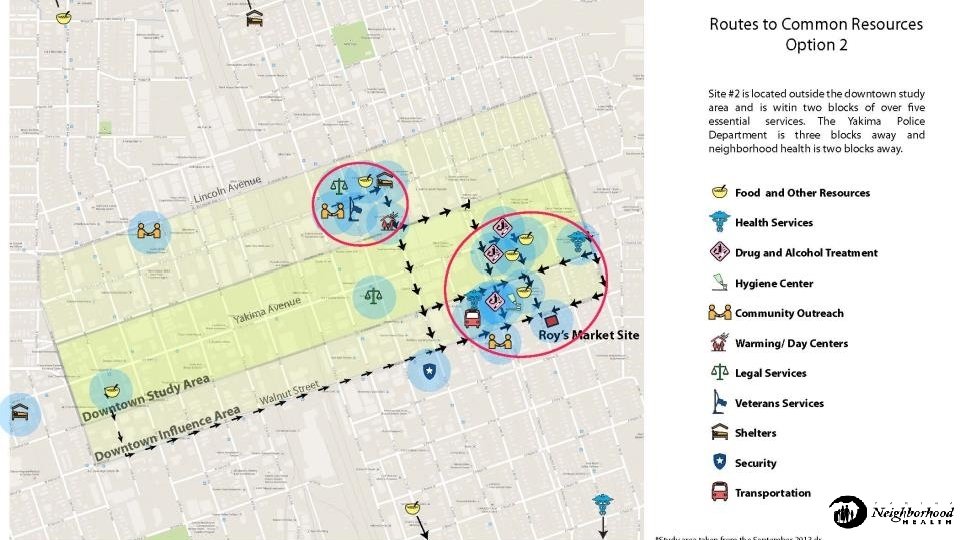
Families ls a u d i v i d n I Location, Location! s t l u d A g n u o Y “Everybody Loves Us Until…. ” Marty Miller, ORFH Inherit, Buy, Lease, or Build ? Respit e

RDH Center Opens March 2019 22 Unit s 37 Indi viduals 6 dedic at 3 dedic ed for familie s ated fo r Veter ans

• Five “Dwelling Units” • 4 -5 individual units • Shared kitchenettes • Shared restroom and shower • Public / Visitor Center 9 am -10 pm • Enrichment / Learning Center and resident’s storage area. • Private open-air courtyard access from interior only for residents. • Resident laundromat accessible from inside. • Public Laundromat accessible from outside (open daytime hours). Enter Here • Resident Manager 24/7. • Contracted Security.

Back to the Kool-Aid Housing is Health Care Outcomes tied to the IHI Triple AIM Improving rate of successful connection to primary care Increasing rate of compliance with care plans Improvement in chronic disease measures (e. g. A 1 c scores, BP measure) Reduction in communicable disease (e. g. TB, STDs, Hep C) Reduction in behavioral health crisis episodes Back to our Providers’ Request… Medications are better managed More likely to obtain and maintain employment or education Greater success for recovering SUD recovering patients in supportive housing

Increasing Access to Care 2018 Health Coverage 100% 89% 90% 85% 77% 80% 73% 70% 60% 50% 40% 30% 20% 10% 0% Universal Homeless PSH Repite

2018 Improving Connection to Primary Care Medical Visits Per User

Improvement in Chronic Disease Measures Controlled Diabetes Controlled Hypertension 92% 100% 80% 90% 80% 73% 70% 60% 70% 52% 50% 60% 50% 40% 30% 20% 20% 10% 0% 0% Universal PSH Respite

Flu Vaccine 84% 90% 80% 70% 60% 50% 40% 30% Reduction in Communicable Disease 26% 25% 18% 20% 10% 0% Universal Homeless PSH Respite

Patients with at Least One Mental Health Diagnosis 80% 73% 70% 60% Reduction in Behavioral Health Crises Inter-Disciplinary Teams Serve High Needs Individuals and Families: 50% 44% 38% 40% 30% 20% 10% 0% Universal Homeless PSH Respite

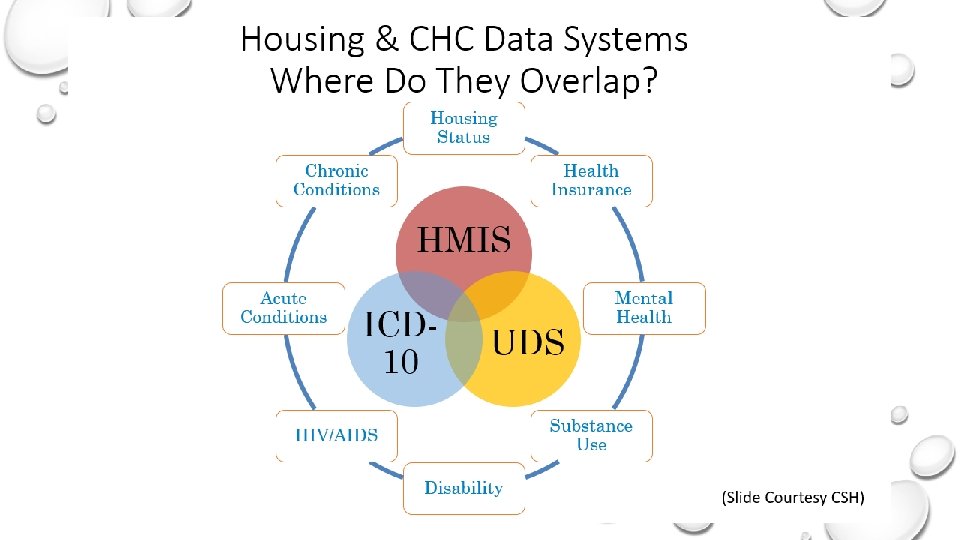
Multi-Disciplines – One Record

Foundational Community Supports 2018 Supportive Housing / Supported Employment Literally Homeless 38% Average Age 42 Many HEN Clients Integrated Services Supportive Housing 25% Housed 35% Bus passes Hygiene Packs Housing Referrals Care Coordination (Health Home) Most Common Qualifying Risk Factors: v 2 or more stays in adult residential care setting (Supportive Housing); PRISM Score > 1. 5, Homeless at least 12 months. v Disruptive Behavior, previous terminations, mental health issues (Supported Employment)

Medical Respite Care Saves $$ Hospital Staff Report a Saving of 53 Inpatient Days in 2018 ($65, 773 for Depression or Respite care reduces public costs associated with frequent hospital utilization. $190, 800 for Rehab) Average Hospital Charge for Depression* Average Hospital Charge for Rehab* Average Respite Program Average Length of Stay 13 days 8. 1 days 20 days Average Charge Per Patient $16, 133 $29, 166 $2, 191 (not including primary care) Average Charge / Cost per Day $1, 241 $3, 600 $111. 28 (not including primary care) *WSHA Hospital Pricing –www. wahospitalpricing. org

Medical Respite Outcome – Reduce Admissions/ Readmissions to hospitals RTN to hospital in 30 days 29% No hospital 71%
 8 visits to E. R. (avg $600")
Since January 2018 30 days Inpatient (rehab) 8 visits to E. R. (avg $600 e) 48 days in respite = = = $37, 230 $ 4, 800 $ 5, 330

• Average PSH Cost Per Chronic Disabled at YNHS: $13, 244 • Housing ($7, 644 for 1 br. unit @$637/mo) • Case management and Supportive services ($5, 600)

“We Know a Thing or Two Because We’ve Seen a Thing or Two” 01 02 03 04 05 Participants may say “No” today, and “Yes” tomorrow ! Trauma Informed Care / Harm Reduction / Motivational Interviewing works but takes time (more time) ! Work vs Disability Benefits – Sometimes Work Wins ! Recovering clients are less likely to relapse when housed ! Families reunify successfully as housing stabilizes and health improves

Rhonda Hauff, COO / Deputy CEO, Yakima Neighborhood Health Services Chair, Respite Care Provider Network, National Health Care for the Homeless Council rhonda. hauff@ynhs. org
- Slides: 34