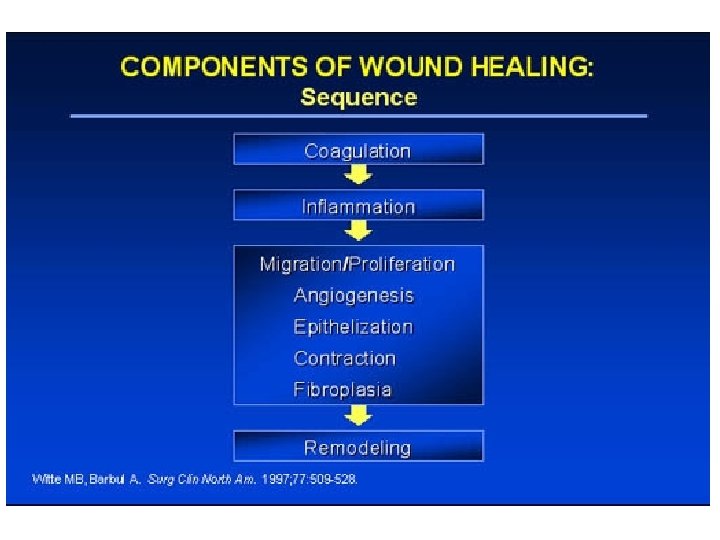
Wounds in General Conflict of Interest Declaration Nothing



_+")



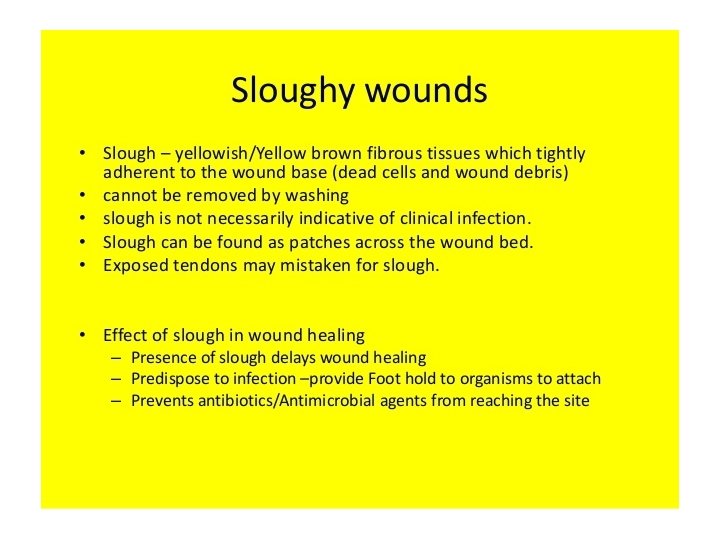
 • FEEL (slough")
 Culture/Investigate/Control/Consult")
---deep tissue/bone cultures. Blood cultures as well • INVESTIGATE (Hgb/WCC/ESR/CRP/Hb.")



")









 What is this? ? What will you")

























")














- Slides: 82
Wounds in General
Conflict of Interest Declaration: Nothing to Disclose Presenter: Dr. Sajay Azad Title of Presentation: Wound Care I have no financial or personal relationship related to this presentation to disclose.
What the mind does not know The eyes do not see
Dermafacta confusiformis What is this? !@£$%^&*()_+
Content-Wound in General • Wound Basics—Theory and Practice • 10 Wound Scenarios—Q&A session • Top Tips for wound management
LFM-CICC Say it as LFM-Kick!!
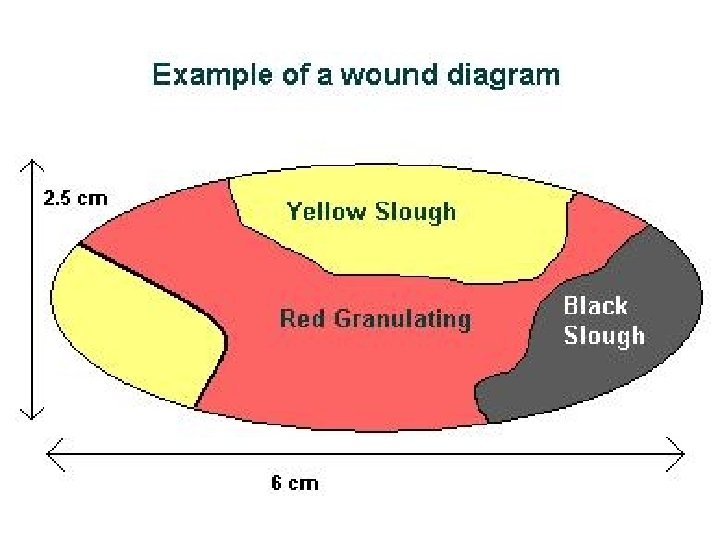
LFM Look, Feel, Measure
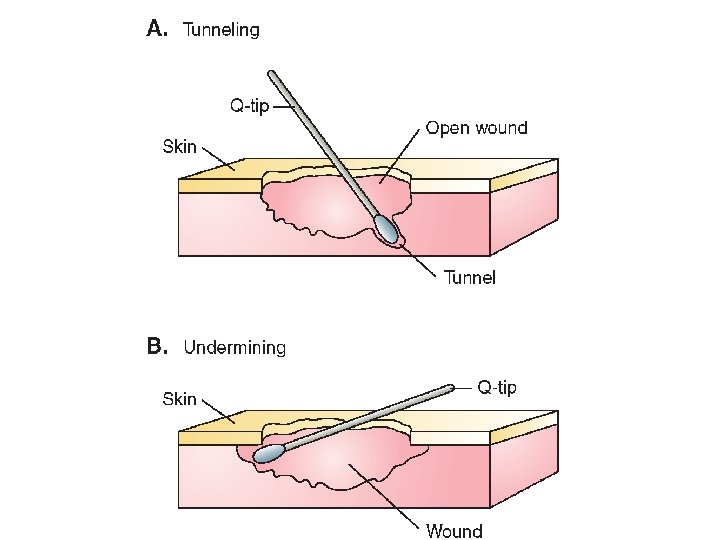
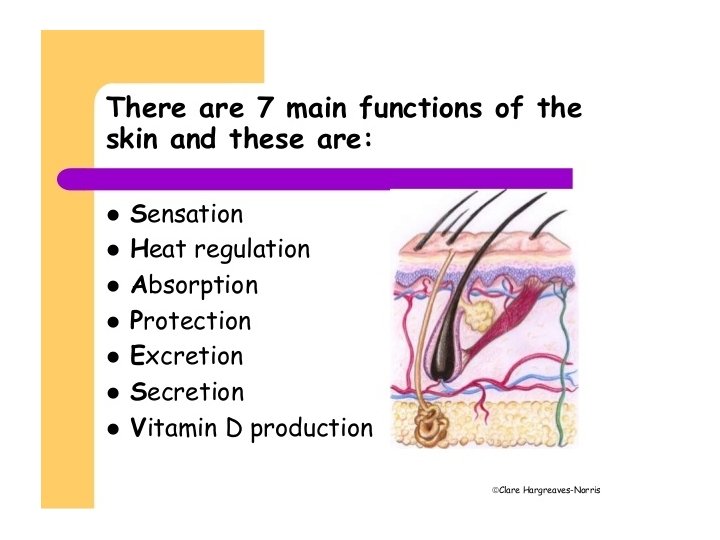
Simple techniques to assess wounds--Skin System First step---LFM • LOOK(site/size/edge/floor/surrounding skin) • FEEL (slough (loose/tough), underminings/suppleness/indur ation/odor/adherence to bone and tendon/ lymphadenopathy/joint mobility/neurovascular status) • MEASURE (length/width/depth)
CICC (Kick) Culture/Investigate/Control/Consult
Second step---CICC • CULTURES (aerobic/anaerobic)---deep tissue/bone cultures. Blood cultures as well • INVESTIGATE (Hgb/WCC/ESR/CRP/Hb. A 1 c/Wound or bone biopsy/CT Scan/MRI scan/Bone scan etc) • CONTROL (DM/smoking/obesity/IVDU/cardiac) • CONSULT (Wound care/ ID/CCDC/Physio/OT/family/Nutritionist/ ICU/Psychologist/Vascular/ortho/plastics/derm)
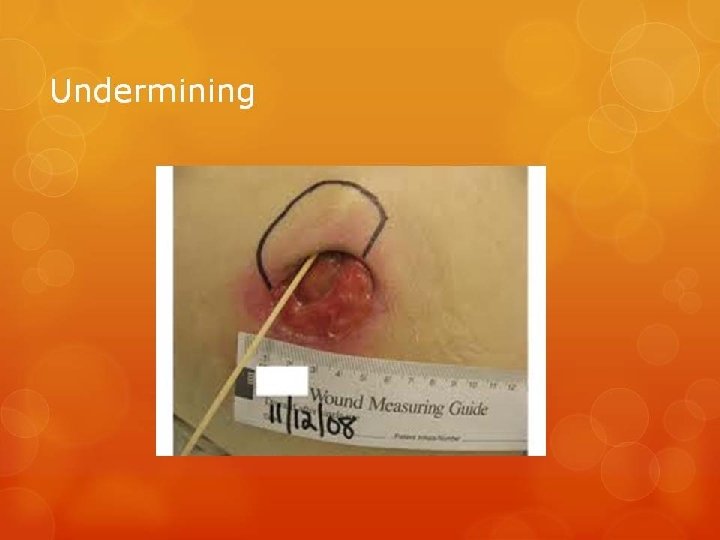
Undermining • Indicate disease process • Need for ‘hidden area debridement’ • Indicates no healing of tissues due to lack of healing potential • More complicated process
CICC “The Kick” Culture, Investigate, Control and Consult
Further imaging • CT scan • MRI • Bone scan/gallium scan
Classify Wounds • Acute • Chronic (>4 wks)
Wound management • • Describe Document Dress appropriately Refer
Key Common Dressings • • • Adaptic Inadine Aquacell Mepilex Honey
Surface wound consider nonadherent dressing
Dressings can cause allergic reactions Watch out for this especially tape which is notorious for blisters and contact allergies
Dressings Wet to dry dressings---defunct Packing---deeper cavity wounds? Adherence control---Adaptic/Inadine Exudate control--Alginates/Hydrogel/Hydrocolloid • Smell control---Metronidazole gel • Healing…………. . Hopefully • •
Frequency of dressings Infected/oozy/smelly-Daily Not overtly infected wound---Alternate day dressings Burn/Stable wound---twice a week
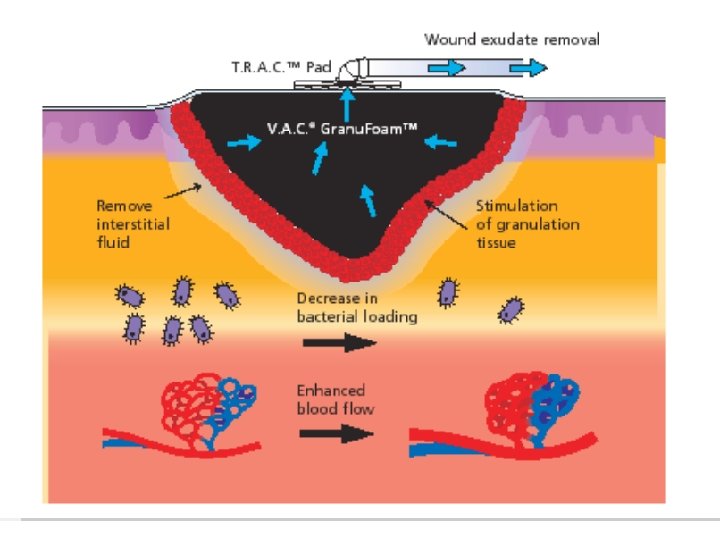
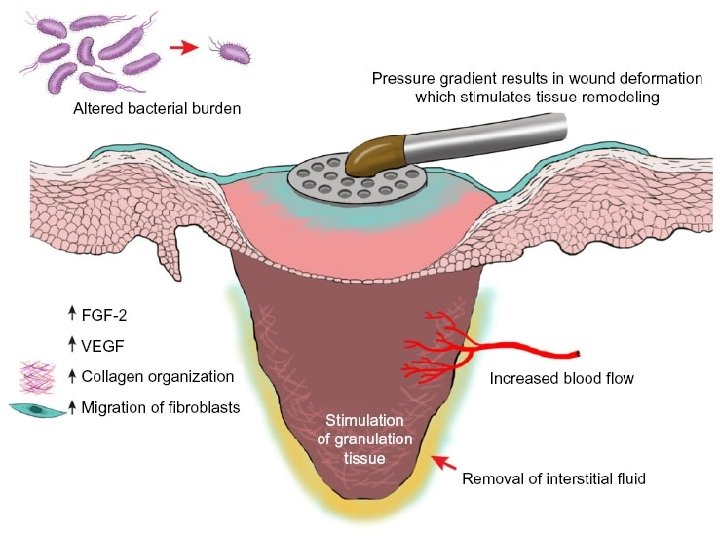
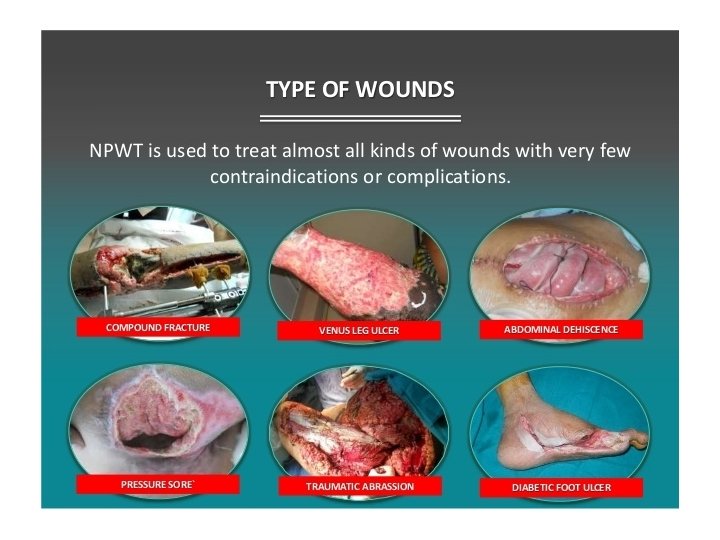
NPWT Not the answer to every wound Not substitute for flap Best in deeper wound with discharge Cannot remove deep slough
NPWT No concrete evidence to suggest type of sponge/pressure/mode makes any difference. No evidence to support use of antibiotic infusion or irrigation modes
10 Wound Scenario Quiz (Brief history provided) What is this? ? What will you assess? ? What will you do? ?
Case 1
Cases • • • Diabetic foot Pyoderma gangrenosum Pressure ulcer Necrotic skin cancer Cellulitis of the hand Leg ulcer Granulating wound Deep sloughy wound Bruised hand due to thin skin Necrotizing soft tissue infection
Top tips for Wounds in General
Any wound not healing after 3 -4 wks should be considered a problem wound Why is it not healing
Never forget the ‘Skin system’ in your regular clinical examination Twice a week on rounds Highlight to residents/nurses/therapist THIS PATIENT HAS A SKIN SYSTEM PROBLEM!!
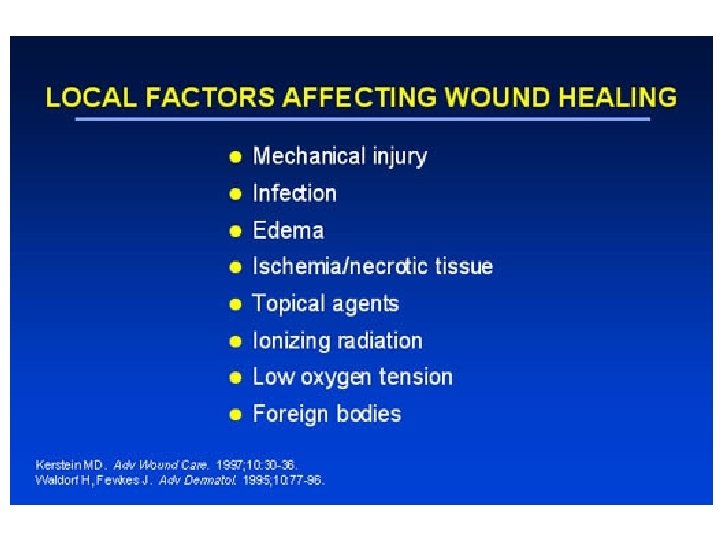
Factors worth addressing • • • Personal hygeine Smoking Diabetes Substance abuse Vascular issues Foreign body in wound (retained stitch) Positioning issues Family support Educating the patient regarding the wound
When in doubt perform a punch biopsy
Shallow slough versus deep, adherent slough When deep it probably needs surgical debridement
Deep yellow or black tissue requires debridement Thin yellow tissue on wound should be ok, but always think of Biofilm
Always consider doing culture swabs or tissue culture where possible
When in doubt consider using nonadherent dressing like Adaptic or Jelonet
Wound washing Desirable---clears surface debris, promotes hygiene, facilitates healing
Pain relief critical To aid compliance To facilitate dressing changes Must be non-addicting Facilitates mobilization Overall better healing plan
Wound treatment Establish boundaries of care Compliance is critical to improvement
Deep wound Complex wound, vital structures involved, probably plastic surgery intervention for closure
Any wound without exposed deeper structures and less than a ‘looney size’ will heal typically with good wound care
Exposed bone/tendon/cartilage/nerve/blood vessel/joint Flap---piece of tissue with its own blood supply
Rapid disease progression Necrotizing soft tissue infection--NSTI (Nec Fasc)
Raised, heaped edge Consider Skin cancer
Frequency of labs Twice a week adequate for most Hgb/Albumin/ESR/CRP/WCC Cultures at most dressing changes
Urgency of specialist review NSTI---Immediate Infected and discharging wound---Urgent Gr A strept---Urgent Chronic wound/leg ulcers---Non-urgent (23 days) • Pressure ulcers---Non-urgent (2 -3 days) • Large wound---review in ambulatory care by specialist • •
Streptococcus spells trouble and must be cleared before any reconstruction Because of fibrinolysis, ability to spread infection, high graft and flap failure
Amputation versus salvage for Diabetic foot Amputation • Hind foot bone involvement • Multiple deep plane involvement • Severe N-V compromise • Smoker • Diabetes ++ • Lack of compliance • Failure of trial of limb salvage for 3 months Limb salvage • Forefoot and mid foot involvement • Non smoker • Well controlled DM • Motivated and compliance receptive • Contralateral limb amputation
Special wounds • Diabetic • Pressure ulcers • Necrotizing soft tissue infections
If no suspected cancer or deep slough in a deeper wound Black sponge NPWT at pressure of 75100 mm. Hg at either Continuous/Intermittent mode is better when wound is starting to granulate
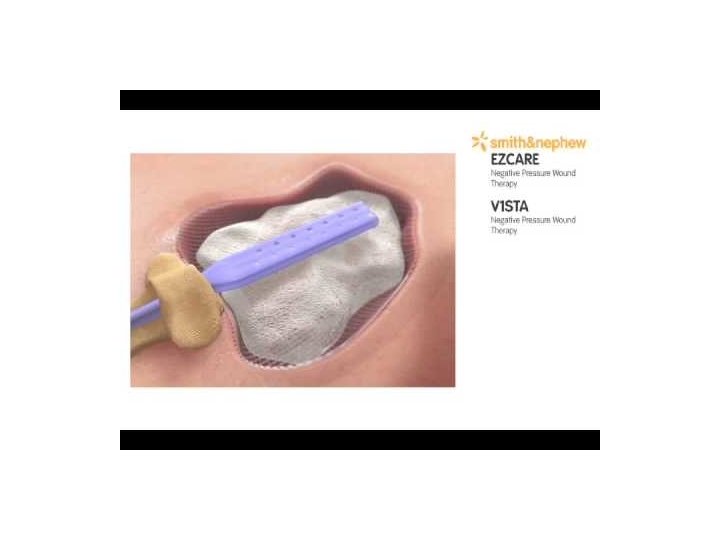
Cavity wound consider NPWT
All specialists feel that it is not their total domain? Wound care would be useful to consult to direct patient care
MRP status issue? Specialist find it useful to have FP/Internal medicine input as MRP status requires that broad expertise
Dry, shrivelled toe or finger? ? Betadine application daily Natural autoamputation Proximal infection---Surgical removal and drainage Significant chance of Whole Limb Loss
Vascular intervention? ? Good for macroangiopathy Will not address microangiopathy
Wound healing not complete? ? Complete wound healing is aim but partial wound healing is reality and should be emphasized to patient and family
Is this wound palliative? ? Frail/elderly/severe cardio-pulmonary disease/DM++/protein deficient despite full intervention/smoker/non compliant/IVDU/2 failed major reconstructions/lack of family support