Wound Healing Tissue injury and response Wound repair


 Simple suturing, skin graft replacement, or flap")


 Inflammatory phase Ø Hemostasis Ø Vascular permeability Ø Cellular recruitment 3 days, except")
 Proliferative phase Ø Angiogenesis Ø Epithelization, first 24 hrs, peak 48 hrs Ø")
 Maturation phase Ø collagen cross-linking Ø collagen remodeling Ø wound contraction")



 Ø Ischemia Circulation Respiration Local")









")
")



- Slides: 31
Wound Healing 林燦勳醫師
Tissue injury and response Ø Wound repair Tissue to restore normal function and structure after injury Ø Regeneration Perfect restoration of the preexisting tissue architecture in the absence of scar
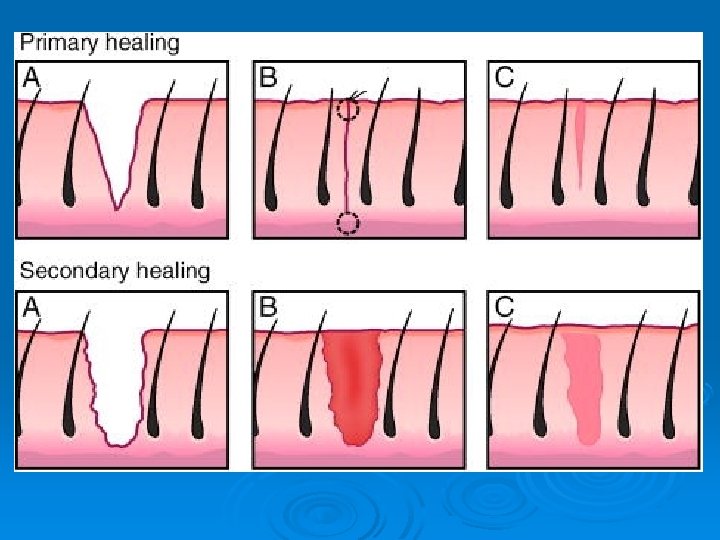
Wound closure type Ø Primary ( first-intension) Simple suturing, skin graft replacement, or flap closure Ø Secondary ( spontaneous-intension) Reepithelization and contracture Ø Tertiary (delayed primary)
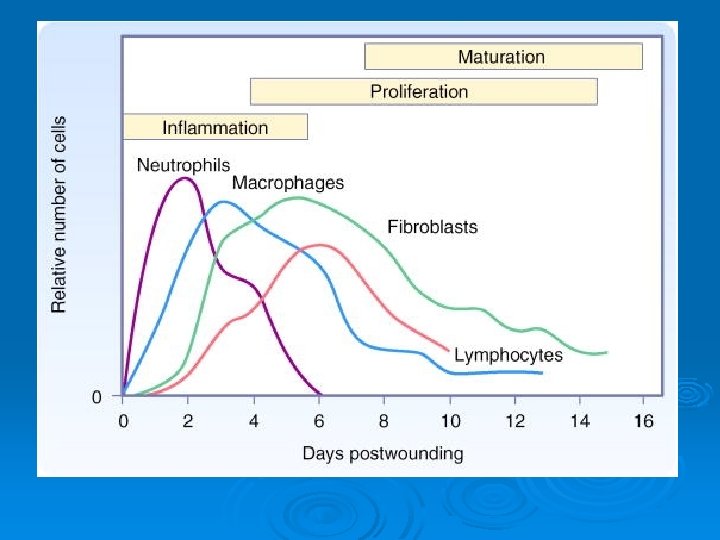
Wound healing phase Ø Inflammatory phase limit damage, preventing further injury Ø Proliferative phase reepithelization, matrix synthesis, neovasculation Ø Maturation phase Scar contraction with collagen cross-linking, shrinking, and loss of edema
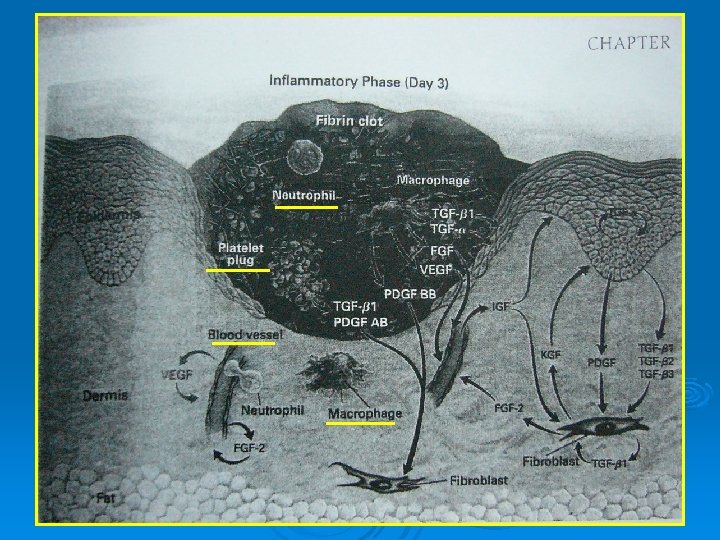
(一) Inflammatory phase Ø Hemostasis Ø Vascular permeability Ø Cellular recruitment 3 days, except infection
(二) Proliferative phase Ø Angiogenesis Ø Epithelization, first 24 hrs, peak 48 hrs Ø Fibroplasia, day 5 ~ 6 weeks Ø Formation of granulation tissue
(二) Maturation phase Ø collagen cross-linking Ø collagen remodeling Ø wound contraction
III
Ø Wound contraction , 1 wk Fibroblast and ECM interaction Centripetal movement of skin Reducing the amount of scar Ø Wound contracture Excess scar Physical constriction & limit function
Type of cutaneous wound Ø Full-thickness wounds deeper than the adnexa heal by contraction , granulation tissue formation and reepithelialization. Contraction, 40% decrease in the size Ø Partial-thickness wounds.
Factors that inhibit wound healing Infection(>105, any B-hemolytic strptococcus) Ø Ischemia Circulation Respiration Local tension Ø Diabetes mellitus Ionizing radiation Ø Advanced age Ø Malnutrition (albumin<2) Ø Vitamin deficiencies Vitamin C Vitamin A Ø Mineral deficiencies Zinc Iron Ø Exogenous drugs Doxorubicin (Adriamycin) Glucocorticosteroids Ø
Wound dressing Ø Antimicrobial salves Ø Antimicrobial soaks Ø Synthetic coverings Ø Biological covering (within 72 hrs, before high bacteria colonization)
Wound dressing
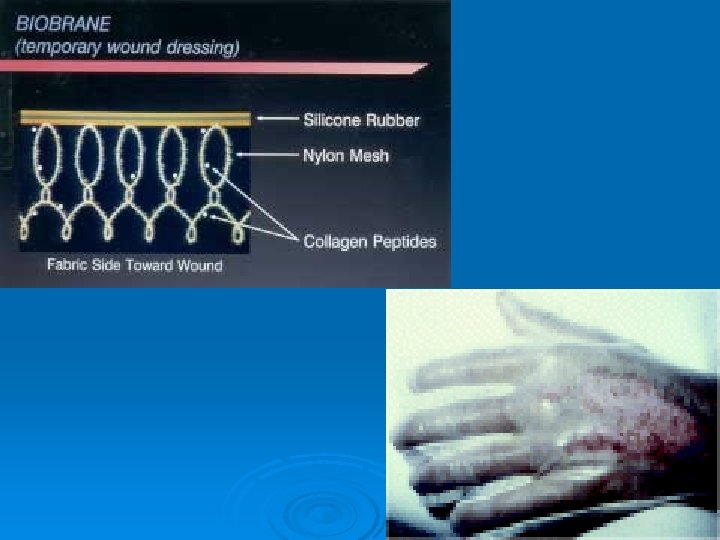
Synthetic coverings Ø Withour painful dressing changes, barrier, decrease pain, not inhibit epithelization Ø Op. Site Ø Biobrane Ø Transcyte Ø Integra
Biobrane Ø Ø Ø 1979 collagen-coated silicon in a sheet adherent in 24 -48 hours a barrier of moisture loss relative painless wound not require change dressing Ø Ø impermeable to bacteria complicated by exudate accumulation risking invasive wound infection
Ø Clinical Indications: Ø superficial to mid-partial thickness burns Ø excised burn wound with or without meshed autografts Ø donor sites Ø partial thickness skin slough disorders
Duoderm Ø Pectin, gelatin: absorption of exudate, activate PMN, macrophage Ø Polyurethane foam: negative pressure, angiogenesis Ø PH: 6. 2
Occlussive dressing
Ø Reepithelization Dry wound < moist wound Open wound < occlusive wounds
Faster healing Neovasculation within granulation tissue is stimulated by hypoxia Prevent crust formation and dry of wound bed Wound fluid – fibroblast proliferation Not applied to inflammed eczematous skin and border of stasis ulcer
VAC (Vacuum-Assisted Closure)
VAC (Vacuum-Assisted Closure)
Principal indications for the use of the mains powered VAC Ø Acute and traumatic wounds Ø Subacute wounds (i. e. dehisced incisions) Ø Pressure ulcers Ø Chronic open wounds (stasis ulcers and diabetic ulcers) Ø Meshed grafts Ø Flaps
Small ambulant unit is recommended Ø Venous stasis ulcers Ø Lower extremity diabetic ulcers Ø Pressure ulcers Ø Lower extremity flaps Ø Dehisced incisions Ø Grafts
Contraindications for VAC Ø Fistulas to organs or body cavities Ø Necrotic tissue in eschar Ø Osteomyelitis (untreated) Ø Malignancy in the wound