Wound Healing Dr Ashraf Abu Karaky The University

Wound Healing Dr Ashraf Abu Karaky The University Of Jordan

Chapter 4 Contemporary Oral and Maxillofacial Surgery.

Causes of tissue damage Physical Chemical Incision Agents with Crushing unphysiologic PH Agents with unphysiologic tonicity Proteases Vasoconstrictors Thrombogenic agents Overheating Overcooling Desicciation Irradiation Compromised blood flow

Epithelialization Establish the integrity of injured epithelium Proliferation, migration and contact inhibition No blood vessels, subepithelial tissues, vascularized tissue bed. Oro-antral fistula: contact inhibition


STAGES OF WOUND HEALING Inflammatary Fibroplastic Remodiling

Inflammatary stage Begins the moment of tissue injury 3 to 5 days in absence of factors prolong inflammation Also called Lag stage. No collagen. Two phases: vascular and cellular

Vascular phase Starts during inflammation Vasoconstrection Blood coagulation WBCs; histamine, PG E 1 and E 2; vasodilation; open spaces in endothelial cells; plasma and leukocytes into interstitial tissues; plasma produce fibrin; fluid accumulation EDEMA

Cellular phase: Triggered by activation of serum complement by tissue trauma; chemotactic factors; neutrophils (migration), vessels (diapedesis). Neutrophils; contact bacteria and foreign bodies; lysosomes (Proteases); degranulation Monocytes (e x macrophages); clearance of debris; phagocytosis Lymphocytes: B lymphocytes antibodies T lymphocytes stimulate B cell proliferation and differentiation

Fibroplastic stage Fibrin; crisscross wounds; latticework; fibroblasts lay down ground substance and tropocollagen Ground substance; mucopolysacharides, cement collagen fibers Fibroblasts transform pluripotential mesenchymal cells; tropocollagen formation at 3 rd and 4 th day.

Fibroblasts also secrete fibronectin; stabalize fibrin, assist recognition of foreign material, chemotatic for fibroblasts, guide macrophages. Fibrin network; used by new capillaries which bud from vessels along the margin of wound. New capillaries bring plasmin; fibrinolyses.

Fibroblasts; tropocollagen; cross-linking to produce collagen Collagen is produced in large amount; poor orientation of fibers; decrease effictiveness. Fibroblastic stage 2 to 3 wks. At the end; wound is stiff (large amount of collagen), erythematous (vessels) Withstand 70 to 80% of normal tension.

Remodeling stage Known also as wound maturation Continues indefinitly Random collagen and excessive vessels destroyed Wound never reach more than 80 to 85% of strength No Elastin Wound contraction; start early in remodeling phase

Surgical significance of wound healing Adherence to surgical principles facilitates optimal wound healing No healing without scaring, not prevent but reduce scar.

Factors impair wound healing Foreign materials; bacteria, dirt, suture material… Necrotic tissues; barrier, bacteria, hematoma Ischemia Tension

Healing by primary and secondary intention Slower, more scar. Extraction socket, poor reduced fractures, avulsive injuries Tertiary intention, use of flaps that heals with secondary intention.


Healing of extraction socket first week The removal of a tooth initiates inflammation, epithelialization, fibroplasia and remodeling. Extraction; blood clot, inflammatory stage (1 st wk). WBCs inter the socket (bacteria, debris, bone fragments. . ) Fibroplasia: ingrowth of fibroblasts and capillaries; epitheluim migrate down the socket to epitheluim from other side or granulation tissue under the blood clot. Osteoclasts accumilate along the crestal bone

Second week Large amount of granulation tissue fills the socket Osteoid deposition Small sockets; epitheluim fully intact 4 to 6 wks; epitheluim 4 to 6 month cortical bone resorbed, new bone X-ray One year; scar tissue

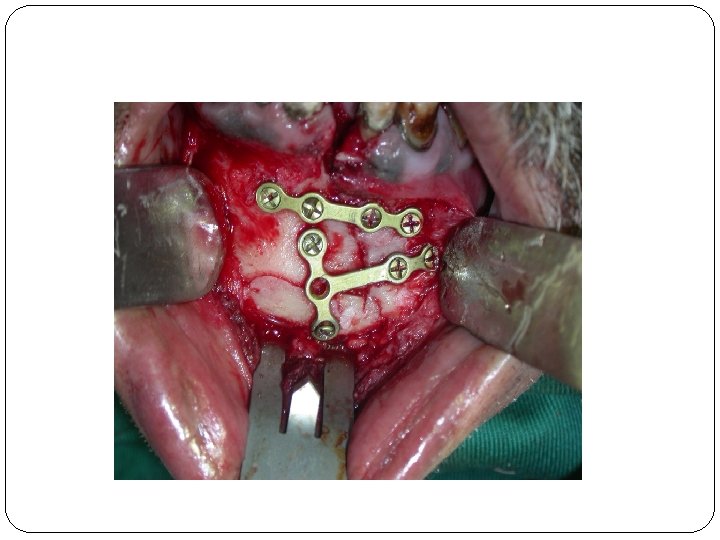
Bone healing Inflammation, fibroplasia, remodeling. Osteogenic cells; Osteoclasts, osteoblasts. Periosteum, endosteum, mesenchymal cells. Osteoclasts; funx? Osteoblasts; funx? Osteoid, immobile. Callus Primary and secondery intention (1 mm or more)
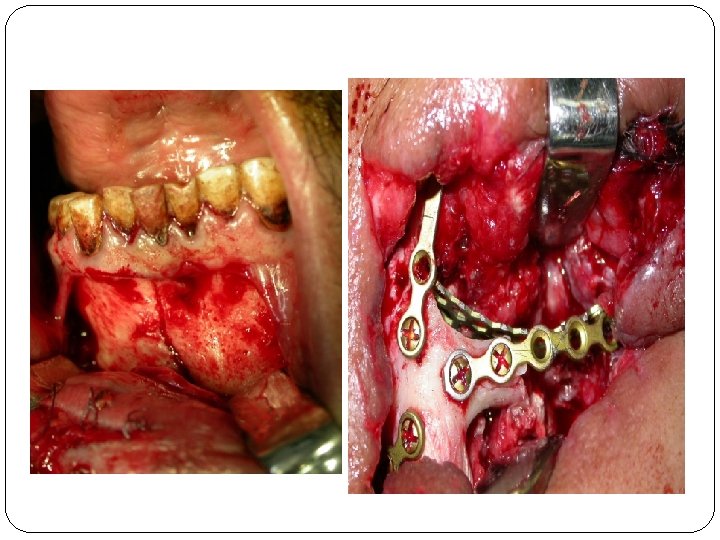

Two main factors in bone healing: 1 - vascularity 2 - immobility Functional matrix concept. Contaminated fractures.

Nerve healing Usual causes of nerve injury: Mandibular body fractures Preprosthetic surgery Sagittal split osteotomy Jaw resections Removal of impacted teeth



Classification: Neuropraxia, axon and epineural sheath maintained, inflammation and ischemia, few days to weeks. Axonotmesis : axons continuity disrupted, 2 to 6 months (but not always) neurotmesis: axon and epineural sheath disrupted.

Nerve healing has 2 stages; degenration and regeneration. Degeration 2 types: Segmental demyelination; slow conduction and might prevent some nerve impulses, paresthesia, dysesthesia, hyperesthesia. Wallerian degeration; interruption of axons and myelin sheath; stops all nerve conduction.

Regeneration ; 1 to 1. 5 mm a day. Abnormal; Continuity disrupted by connective tissue; find a way around it or Neuroma.

Thank you
- Slides: 33