WOUND CLOSURE VECTOR ANALYSIS PHACO VERTICALLY APPLIED IOP
 PHACO • VERTICALLY APPLIED IOP AND TISSUE FORCES IN OPPOSITE")







 ü 2.")
 ü A 15° freehand/preset depth (300 micron")
 INCISION ü Peritomy and cautery ü Grooving")
 • • • Well suited for topical anesthesia lesser risk")

 • • • limbal groove Straight")












- Slides: 33
WOUND CLOSURE (VECTOR ANALYSIS) PHACO • VERTICALLY APPLIED IOP AND TISSUE FORCES IN OPPOSITE DIRECTION ECCE • HORIZONTALLY APPLIED SUTURE FORCE
DYNAMICS OF SUTURELESS CATARACT INCISIONS THEORY • Corneal flap mechanism • Square incisional geometry
SQUARE INCISIONAL GEOMETRY üEXTERNAL INCISION üINTERNAL INCISION üTUNNEL SIZE
astigmatically neutral funnel ücorneal astigmatism is directly proportional to the cube of the length of the incision üinversely related to the distance from the limbus •
SELF-SEALING WOUND DEPENDS ON üThe architecture of the wound üDelicate handling of tissue edges üAdequate intraocular pressure
PHACO INCISION GOALS üINTRAOPERATIVELY üPOSTOPERATIVELY
INTRAOPERATIVE ü Allow Easy Entry Of The Phaco Needle ü Allow Ease Of Mobility Of The Phaco Needle ü Minimize Incision Leak ü Prevent Incision Burn.
POSTOPERATIVE ü Self Sealed ü Astigmatically Neutral ü Both In Short Term And Longterm
vital statistics of a phaco incision ü 1. Site (limbal or …) ü 2. Placement (time of incision!) ü 3. Style(mood of the incision!) ü 4. The length of the external incision ü 5. Length of the sclerocorneal tunnel ü 6. Depth of tunnel dissection ü 7. Size of initial opening for phacoemulsification 8. Size of incision for IOL insertion ü 9. Paracentesis opening
INSTRUMENTS REQUIRED FOR THE PHACO INCISIONS(sclera tunnel) ü A 15° freehand/preset depth (300 micron ü A 2. 0 mm broad crescent blade ü A suitable breadth keratomewith a 90 degrees angle at the tip (bevel up) ü A 0. 6 to 1. 0 mm broad blade for the paracentesis ü A blunt tipped extender blade (bevel down) ü A caliper
TECHNIQUE OF MAKING A PHACO (Scleral Tunnel) INCISION ü Peritomy and cautery ü Grooving ü Tunnel dissection ü Stab incisions and AC viscoinjection ü AC entry
clear corneal incision (advantages) • • • Well suited for topical anesthesia lesser risk of bleeding better accessibility better red reflex eliminates the conjunctival incision minimal or no effect on astigmatism
disadvantages of clear corneal incision • • technical difficulty lack of forehead support need to enlarge for use of nonfoldable IOLs difficulty in converting to a ECCE potential for greater endothelial cell loss. possible corneal thermal burns. higher incidence of endophthalmitis in some studies
Proposed incision for begginers (changing ECCE to phaco) • • • limbal groove Straight or Parallel to limbus Biplanar Slightly wider than phaco tip
PARACENTESIS OPENING ü required for bimanual techniques ü Usually on the left side (30 -90 degree) ü 0. 6 to 1. 0 mm in breadth ü simple stab or shelved
Clear Cornea Incision üWith initial partial thickness vertical incision üWithout an initial incision
ASTIGMATIC INDUCERS ü 1. Longer incision. ü 2. Corneal incision. ü 3. Limbus parallel incision. ü 4. Uniplanar incision. ü 5. Sutured incision
The caliper is set at 2. 8 mm.
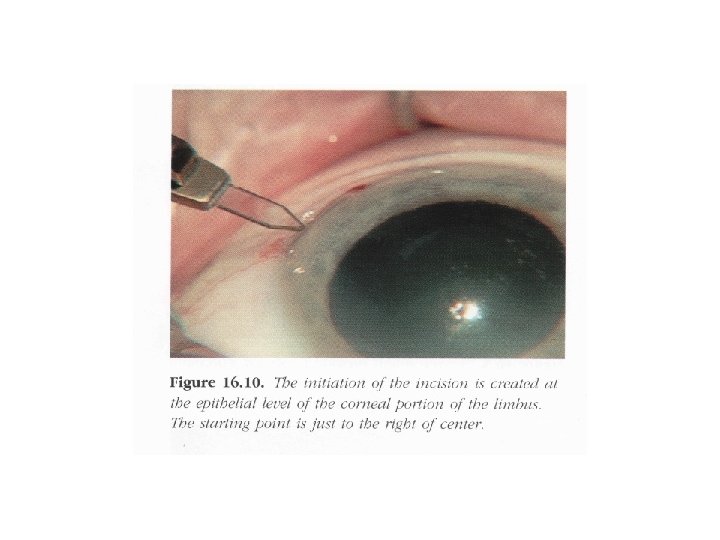
A light indentation on the peripheral corneal surface is created with the pointed ends 0 f the caliper.
A 150 -300 -um-depth groove is created
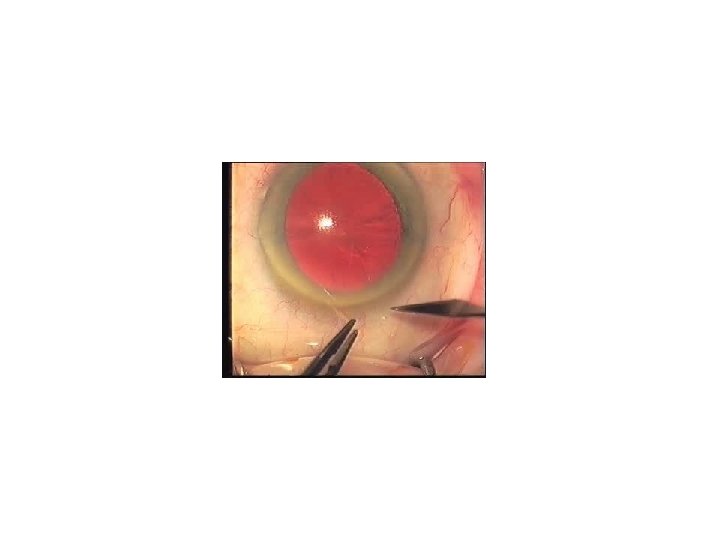
A paracentesis incision is created with the diamond blade fully extended
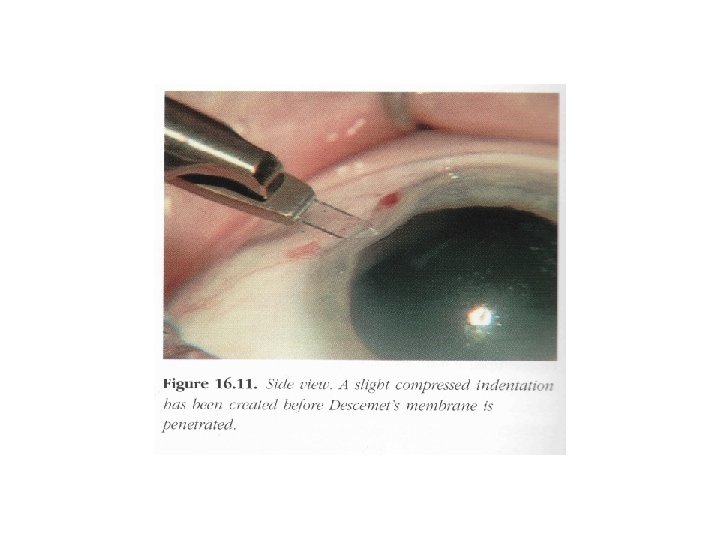
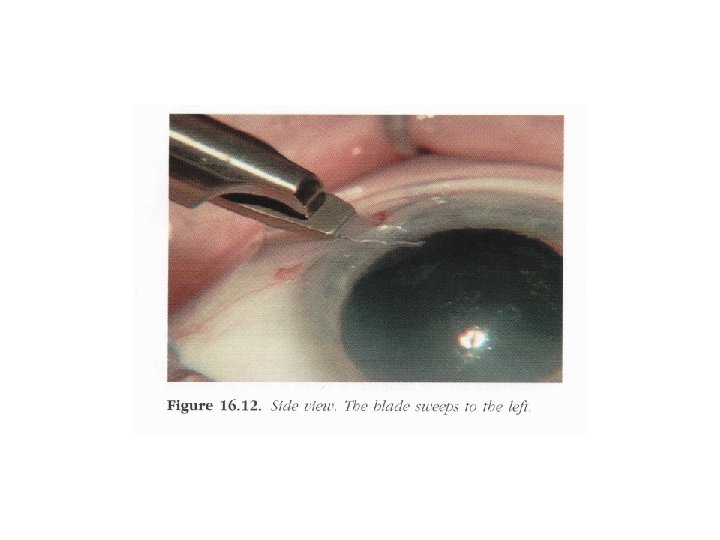
An oblique entry is created as the blade not only driven through the corneal stroma to Descemet 's level. but also slices to the surgeon 's left. Notice the compression of tissue being created because ofthe relatively dull blade
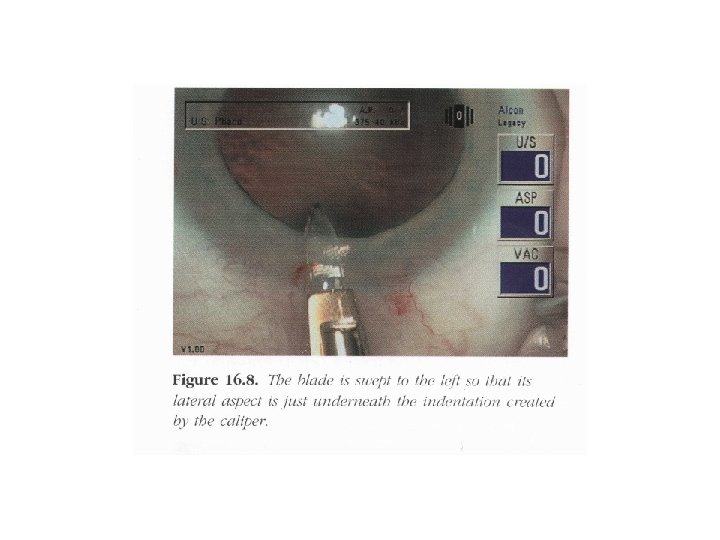
Descemet's level is entered 1. 75 mm from the epithelial level as the blade is swept to the left.