Work up Hepatitis B andor C Bilirubin transaminase

診斷 • Work up – 肝炎檢查 • Hepatitis B and/or C – 是否轉移 • 最常轉移的地方 : 肺、腹部淋巴結、骨頭。 – 肝功能 • Bilirubin, transaminase, ALP, LDH, albumin • Child-Pugh classification to compensated (class A) or decompensated cirrhosis (class B or C) • 臨床是否有肝門靜脈高壓 – PT/INR, CBC, renal function 2020/11/4 3

BCLC 分期與治療策略 Stage 0 Stage A-C Stage D PST 0, Child-Pugh A Okuda 1 -2, PST 0 -2, Child-Pugh A-B Okuda 3, PST > 2, Child-Pugh C Early stage (A) Intermediate stage (B) Advanced stage (C) Very early stage (0) Single or 3 nodules Multinodular, PST 0 Portal invasion, Single < 2 cm < 3 cm, PST 0 N 1, M 1, PST 1 -2 Carcinoma in situ Single 3 nodules ≤ 3 cm Portal pressure/bilirubin Increased Normal Resection Terminal stage (D) Associated diseases No Liver transplantation (CLT/LDLT) Yes PEI/RFA Curative treatments 50% to 75% at 5 yrs Llovet JM et al. Lancet. 2003; 362: 1907 -1917. Systemic treatment Randomized controlled trials 40% to 50% at 3 yrs vs 10% at 3 yrs Chemoembolism Symptomatic treatment
 • BCLC分期與治療策略: 1. Stage 0 (very early), PST 0,")
肝部分切除 ( Partial hepatectomy ) • BCLC分期與治療策略: 1. Stage 0 (very early), PST 0, Child-Pugh A Single < 2 cm, carcinoma in situ 2. Stage A (early), PST 0, Child-Pugh A-B, single, portal pressure/bilirubin (normal) 2020/11/4 6
 • BCLC分期與治療策略: 1. Stage A (early), PST 0, Child-Pugh A-B, single, portal")
肝臟移植(Liver transplantation) • BCLC分期與治療策略: 1. Stage A (early), PST 0, Child-Pugh A-B, single, portal pressure/bilirubin (Increased), associated diseases (No) 2. Stage A (early), PST 0, Child-Pugh A-B, 3 nodules ≤ 3 cm, associated diseases (No) 2020/11/4 8
 單一腫瘤<5 cm 三顆腫瘤都少於 3 cm + 沒有血管入侵與肝外擴散")
肝臟移植 Milan Criteria (Stage 1 and 2) 單一腫瘤<5 cm 三顆腫瘤都少於 3 cm + 沒有血管入侵與肝外擴散 • 移植後,5年存活率超過70%。 • ‘rule of seven’ (最大腫瘤的長度[cm] +腫瘤數目 ≤ 7) : 5年的存活率可達 71%. • 5 -yr 復發: < 15% Mazzaferro V, et al. N Engl J Med. 1996; 334: 693 -699. Llovet JM. J Gastroenterol Hepatol. 2002; 17(suppl 3): S 428 -S 433.
/RFA(無線電頻率繞 灼治療術) • BCLC分期與治療策略: 1. Stage A (early), PST 0, Child-Pugh A-B, single, portal")
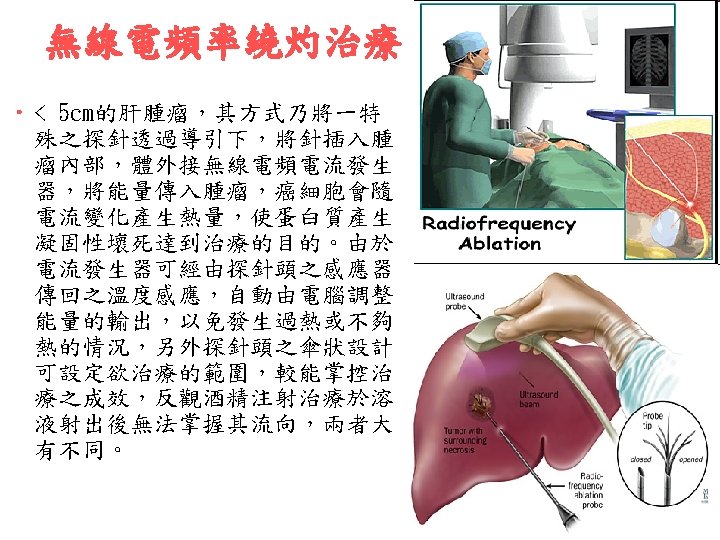
PEI(經啤酒精注射)/RFA(無線電頻率繞 灼治療術) • BCLC分期與治療策略: 1. Stage A (early), PST 0, Child-Pugh A-B, single, portal pressure/bilirubin (Increased), associated diseases (Yes) 2. Stage A (early), PST 0, Child-Pugh A-B, 3 nodules ≤ 3 cm, associated diseases (Yes) PEI: percutaneous ethanol injection RFA: radiofrequency ablation 2020/11/4 10
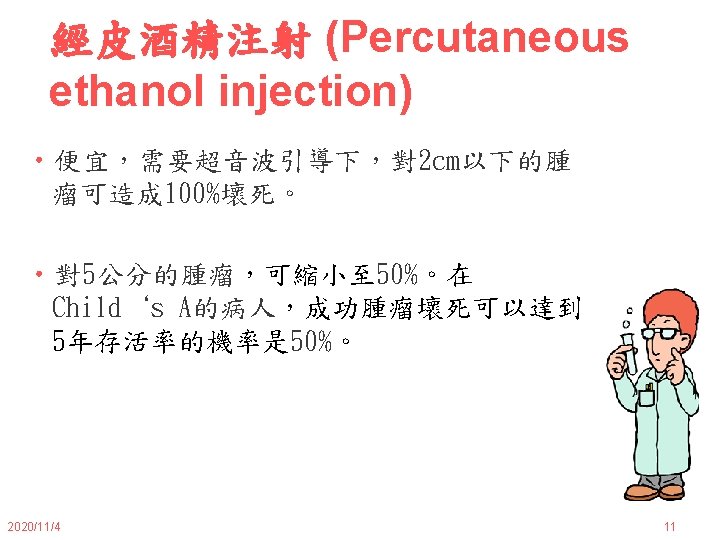

局部治療 • 病人選擇與禁忌 – PEI • • 2020/11/4 腫瘤 <2 cm,但無法開刀。如果腫瘤在肝臟穹 窿地方,也不考慮。 禁用於有肝外轉移( extrahepatic disease), 肝門 靜脈栓塞( portal vein thrombosis), Child-Pugh class C cirrhosis with a prothrombin time >40 % of normal, or a platelet count <40, 000/micro. L。 12
 • BCLC分期與治療策略: 1. Stage B (intermediate), PST 0, Child-Pugh A-B, multinodular TACE :")
化療栓塞(Chemoembolism) • BCLC分期與治療策略: 1. Stage B (intermediate), PST 0, Child-Pugh A-B, multinodular TACE : Transcatheter arterial chemoembolication 2020/11/4 16
 • Doxorubicin, cisplatin , mitomycin • 適應症 – 治療無法手術 HCC – 切除前或無線電頻率繞灼治療前,用於縮小腫瘤 (Prior")
TACE(經肝動脈化學栓塞) • Doxorubicin, cisplatin , mitomycin • 適應症 – 治療無法手術 HCC – 切除前或無線電頻率繞灼治療前,用於縮小腫瘤 (Prior to resection or radiofrequency ablation) – 進行同位肝移植前,縮小腫瘤 (Prior to orthotopic liver transplantation) 2020/11/4 17
 Random Effects Model,")
Arterial Embolization for HCC Meta-analysis of 6 RCTs (2 -Yr Survival) Random Effects Model, OR (95% CI) Author, Journal Yr Patients, n 0. 01 Lin, Gastroenterology 1988 63 GETCH, NEJM 1995 96 Bruix, Hepatology 1998 80 Pelletier, J Hepatol 1998 73 Lo, Hepatology 2002 79 Llovet, Lancet 2002 112 Overall 503 Median survival: ~ 20 mos Llovet JM, et al. Hepatology. 2003; 37: 429 -442. 0. 1 0. 5 1 2 10 100 Z = -2. 3 P =. 017 Favors Treatment Favors Control
 (Child-Pugh class C) –Biliary obstruction (Bilirubin")
TACE • 禁忌 –肝門靜脈栓塞, 有些資料,在安全嚴格選擇或 局部TACE,還是可進行。 –肝昏迷 (Encephalopathy) (Child-Pugh class C) –Biliary obstruction (Bilirubin >3) 2020/11/4 19

TACE • 相對禁忌,非絕對 – Serum bilirubin >2 mg/d. L – LDH >425 units/L – AST >100 units/L – Tumor burden involving >50 % of the liver – Cardiac or renal insufficiency – Ascites, recent variceal bleed, or significant thrombocytopenia 2020/11/4 20
 • BCLC分期與治療策略: 1. Stage C (advanced), PST 1 -2, Child-Pugh A-B, N")
全身治療(Systemic treatment) • BCLC分期與治療策略: 1. Stage C (advanced), PST 1 -2, Child-Pugh A-B, N 1, M 1 • Systemic treatment for advanced HCC ➤ Systemic chemotherapy (化療) ➤ Molecular target therapy (分子標靶治療) 2020/11/4 21
. 劑量越低 ,效果越差。")
化療Chemotherapy • Doxorubicin and mitoxantrone – 反應率 20% ( 75 mg/m 2). 劑量越低 ,效果越差。 • 5 - Fluorouracil – 毒性低,肝功能不全時,劑量不需調整。 – 與 leucovorin 共用,反應率可達 28%。 – 口服 Capecitabine 反應率 25%。 • Gemcitabine, irinotecan, and thalidomide – Gemcitabine (1250 mg/m 2 once weekly) 效果 維持較長,中位數是 13星期。 – Irrinotecan : 腫瘤穩定。 2020/11/4 23
 – Cisplatin plus doxorubicin — 18% and 49% –")
合併化療 • Cisplatin-based (反應率 %) – Cisplatin plus doxorubicin — 18% and 49% – Cisplatin/ mitoxantrone/ infusion 5 -FU — 24% and 27%。 – Cisplatin, epirubicin and infusional 5 -FU — 15% – Cisplatin, doxorubicin plus capecitabine — 24% – 接續低劑量 infusional cisplatin plus infusional 5 -FU — 47% – Cisplatin plus capecitabine — 6% and 20% 2020/11/4 24

Thalidomide • 對一些悪性腫瘤,可能有不正常血管增生。 在一些小型試驗,單一藥物治療用於肝癌。 – 整體反應率 overall response rates of 3%-7% – 穩定 stable disease rates of 6%-33% – 存活期中位數median overall survival times of 0. 8 -6. 8 months – 一年存活率 14%-27. 3% 2020/11/4 26

2020/11/4 28

Signal transduction by PDGFRfamily kinases and BRAF 2020/11/4 29

治療 • 分子標靶治療 Molecular target therapy – EGFR: Erlotinib, cetuximab – VEGFR: Sorafenib, bevacizumab, sunitinib – The Raf/MAP kinase-ERK kinase (MEK)/extracellular signal regulated kinase (ERK) pathway: Sorafenib 2020/11/4 30

2020/11/4 31

2020/11/4 32
 – 多標靶口服小分子 small molecule tyrosine kinase inhibitor")
Systemic molecular target therapy • Sorafenib (Nexavar®) – 多標靶口服小分子 small molecule tyrosine kinase inhibitor (TKI) that inhibits Raf kinase 與阻斷細胞內 VEGFR, FLT 3, PDGFR, and fibroblast growth factor receptor-1. – 適應症 • 無法切除 HCC • 晚期腎癌 (Advanced RCC) 2020/11/4 34

標靶治療 • Dosing information of sorafenib – 400 mg 口服一天 2次,空腹。飯前一小時或飯 後兩小時。 – 降低 sorafenib 濃度, concomitant use with strong CYP 3 A 4 inducers (eg, St John‘s Wort, dexamethasone, phenytoin, carbamazepine, rifampin, rifabutin, phenobarbital) 應避免。 2020/11/4 35
![晚期肝癌的治療 • 新標靶藥物[1, 2] – – – – Brivanib Erlotinib Linifanib Sunitinib Bevacizumab Ramucirumab](http://slidetodoc.com/presentation_image/4fc2f0b94b08914d547d4fff769fd940/image-37.jpg "晚期肝癌的治療 • 新標靶藥物[1, 2] – – – – Brivanib Erlotinib Linifanib Sunitinib Bevacizumab Ramucirumab")
晚期肝癌的治療 • 新標靶藥物[1, 2] – – – – Brivanib Erlotinib Linifanib Sunitinib Bevacizumab Ramucirumab Everolimus • Sorafenib combination therapy[1] – Sorafenib + chemotherapy – Sorafenib + another targeted agent 1. Finn RS. Clin Cancer Res. 2010; 16: 390 -397. 2. Tanaka S, et al. J Gastroenterol. 2011; 46: 289 -296.

個案一 • 46歲男性有 2型糖尿病, 高血壓, 和慢性B型肝炎,最近被 診斷有肝癌,而且侵犯至右心房。在 1/27/2010住院做 TACE*1。3月因 12指腸潰瘍腹痛住院。給了PPI與 tramadol 後。病人體重增加,尿量減少。雙腳水腫、腹漲,右心功 能變差,只能走幾步路,懷疑腫瘤吃進右心房。 • 3/16接受TACE,病人家屬了解治療的風險。 • Dull pain over epigastric area was also complained and controlled with morphine 5 mg q 6 h and q 4 h prn. • BUN/Cr=43/2. 2, total bilirubin=3. 7, got/gpt=103/69 General condition: better spirit than yesterday Vital signs: fever to 38. 5'C last night without chillness Mental status: alert and oriented Heart sound: tachycardia, murmur(+) Abdomen: soft, tenderness(-), guarding(-) Extremities: swelling and pitting edema of bilateral legs Urine output: 1430 ml, I/O=+730 ml 2020/11/4 39

個案一 : Problem list • HCC 腫瘤破裂 s/p TACE on 3/16,腫瘤入侵至右心房, 內視鏡 有輕微食道靜脈瘤。 • 發燒, post-TACE related, 注意感染症狀。 • 追蹤 liver function and Hb/Hct • 懷疑右心臟衰竭 –體重增加 (81. 4 -> 92. 8 in 8 days), 肺音乾淨 –不要給水,續用利尿劑 • Acute on chronic renal failure, partial improved after hydration –BUN/CRN=33/2. 34 checked on 3/18, recheck renal function after three days of hydration • Duodenal ulcer, A 2 : continue PPI using • Type 2 DM and hypertension : AC sugar=185, BP=120/80 mm. Hg 2020/11/4 40
- Slides: 42