WOMENS HEALTH UPDATE ABNORMAL UTERINE BLEEDING Pamela J

WOMEN’S HEALTH UPDATE ABNORMAL UTERINE BLEEDING Pamela J Keller MSN, CRNP September 29, 2017

BEFORE WE BEGIN- A LITTLE ABOUT ME…. Been a nurse for over 27 years Graduated from University of Pittsburgh 1990 BSN Worked at Children Hospital of Pittsburgh 1989 -1992 in PICU Moved to Harrisburg area, settled in Etters Stared working at HMC in PICU as prn staff nurse, had my son at move Did a lot of office nursing in all realms of primary care till I returned to HMC in 2006

ABOUT ME Started at HMC in May 2006 as Women's Health Care Coordinator and went back to bedside WH nursing, Newborn nursery. Fueled my desire to finally get my NP as I had always wanted to do Graduated from this same program in 2012. Worked as FNP here at HMC with FCM Harrisburg city practice on 3 rd street. Transitioned back to HMC WH in 2014 and work as an NP in Minimally Invasive GYN Surgery Adjunct faculty at HACC Lancaster, OB GYN clinical Clinical preceptor for FNP students for PSU, Millersville, Widener, Walden. I also help teach PA and Med students as they rotate through our division.

FUN FACTS I am an identical twin My sister a nurse, DNP, recently moved to Pittsburgh, VP of Nursing at Allegheny Health Network Daughter Erin Senior PSU studying Kinesiology. . Plans to be a PA Son Adam- graduate of NDSU, won 4 national championships in football, now lives in Philly, works for Financial Equity Company Love Dogs

SORRY PSU…. H 2 P… BUT STILL A FAN

ABNORMAL UTERINE BLEEDING Investigation of AUB has been hampered by confusing and inconsistent nomenclature Lack of standardized methods for investigation and categorization of potential etiologies After extensive discussions, in 2011, FIGO (International Federation of Gynecology and Obstetrics) developed system necessary to diagnose AUB and the Classification AUB.

AUB � Occurs in 10 -25% of women Iron deficiency anemia arises in 21 -67% of case Abnormal uterine bleeding (AUB) has replaced Dysfunctional uterine bleeding (DUB). Acute – usually spontaneously resolves Chronic- lasts > 6 mo Heavy menstrual bleeding (HMB) has replaced menorrhagia
 Heavy bleeding � Should be treated when it")
AUB Heavy menstrual bleeding� Ovulatory (cyclic) Heavy bleeding � Should be treated when it interferes with quality of life � Causes anemia � Need to change pads or tampons frequently � Stains clothing � Soils bedding � Causes avoidance of activities

AUB Intermenstrual bleeding � Occurs in between otherwise regular menses � Primary etiology can be identified and treated � Possible causes Endometrial polyp chronic endometritis � Evaluation needs to identify etiology and exclude malignancy � If no etiology, goal is to relieve symptoms
 � Irregular, non ovulatory (noncyclic) bleeding � May be infrequent,")
AUB Ovulatory dysfunction (AUB-O) � Irregular, non ovulatory (noncyclic) bleeding � May be infrequent, but can be prolonged or heavy, even hemorrhage � Etiology should be identified Example correction of thyroid disease, hyperprolactinemia may restore cyclic menses � Many times PCOS is etiology � Goal is to establish regular bleeding pattern, prevent heavy bleeding, prevent endometrial hyperplasia � Often require fertility treatments to conceive

PALM- COEIN

PALM-COEIN Thorough medical history should be guided by the PALM–COEIN system Focus on details of the current bleeding episode related symptoms past menstrual, gynecologic, and medical history Hx guides appropriate laboratory and radiologic testing. Up to 13% of women with heavy menstrual bleeding have some variant of von Willebrand disease Up to 20% of women may have an underlying coagulation disorder

P=POLYP Endometrial, endocervical polyps � Epithelial proliferations � Compromise a variable vascular, glandular, fibromuscular, connective tissue Often asymptomatic Small minority have malignant potential Polyps either present or absent � Defined by HSC or TVUS imaging Allows for sub classification which may include � Polyp � dimension � Location, number � morphology � Histology

A=ADENOMYOSIS / AUB-A Disorder in which endometrial glands and stroma are present within the uterine musculature- endometriosis in muscle layer of uterus Relationship to bleeding unclear Prevalence from 5 -70% Needs more research US and MRI based diagnostic criteria US-Appearance is related to presence of Heterotopic endometrial tissue in myometrium Diffuse vs focal disease Should also have its own sub classification

L- LEIOMYOMA AUB-L Most commonly known as myoma, or fibroid Prevalence of lesion 70% Caucasians, 80% AA women Deserves own subclass too due spectrum, size, and location Asymptomatic Presence not typically cause of AUB Wide variable of growth

L= LEIOMYOMA AUB-L Classification system considered � Relationship to endometrium and serosa � Location � Size � Amount � Secondary system requires identification of where they are submucosal, or others � Tertiary system is design for sub endometrial, and submucosal
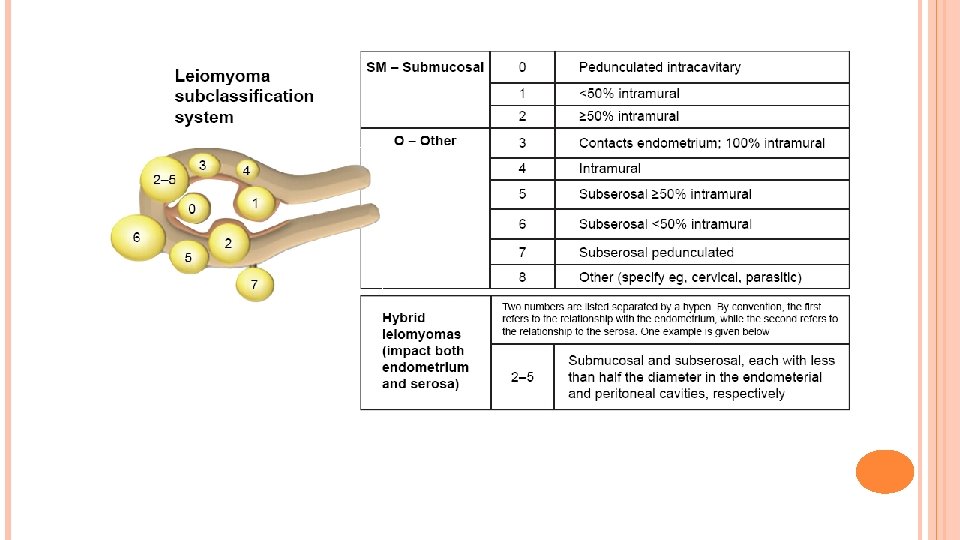

LEIOMYOMA AUB-L

M= MALIGNANCY AND HYPERPLASIA Relatively uncommon Important causes of or finding associated with AUB Must be considered in all reproductive age women AUB-M

COAGULOPATHY- AUB-C Encompasses a spectrum of systemic disorders of hemostasis that may be associated with AUB 13% of women with AUB most often have Von Willebrand Not clear how they cause or contribute Chronic anticoagulation can undesirable side effect of AUB, most often HMB. Could be classified as AUB/HMB-C

OVULATORY DYSFUNCTION AUB-O Contributes to AUB by manifesting as a combination of unpredictable timing of bleeding and variable amount of flow Ovulatory disorders used to comprise DUB Disorders of ovulation can present in many menstrual abnormalities from amenorrhea, to light and infrequent bleeding to extreme HMB requiring medical or surgical intervention From absence of predictable cyclic progesterone production from corpus luteum day 22 -25

OVULATORY DYSFUNCTION AUB-O Many related to “endocrinopathies” PCOS � Hypothyroidism � Hyperprolactinemia � As well as � Mental stress obesity Anorexia Weight loss Extreme exercise Drugs Gonadal steroids Phenothiazine's Tricyclic antidepressants Extremes of age- adolescence to Menopause

ENDOMETRIAL- AUB-E If AUB occurs in context of predictable and cyclic menstrual bleeding, typical ovulatory cycles and no other cause identified, mechanism is likely Disorder of endometrium Can be deficiencies in molecular mechanism of endometrial repair Endometrial inflammation Endometrial infection Abnormality in local inflammatory response Abnormality in endometrial vasculogenseis

IATROGENIC- AUB-I Medical interventions Medical devices IUD Pharmacologic agents � directly impact the endometrium � Interfere with coagulation � interfere with systemic control of ovulation BTB – unscheduled endometrial bleeding that occurs during use of gonadal steroid medication � is a major component of this classification

MEDICATION COMPLIANCE ROLE IN AUB-I Missed, erratic, delayed use of pills, patch, ring Additional and irregular stimulation of endometrium Production of endogenous estrogen Reduces suppression of FSH Effects the development of Follicles

AUB-I Reducing circulating levels of Estrogens, progestin � Anticonvulsants � Anticoagulants � Antibiotics � Smoking � Tricyclic Antidepressants � Phenothiazines � Any med that interferes with dopamine metabolism LNG-IUD- common in first 6 months of use Disorders of hemostasis should be classified in the AUB-C category

NOT YET CLASSIFIED AUB-N Chronic endometritis Arteriovenous malformations Myometrial hypertrophy Poorly defined and examined

AUB General assessment Assess bleeding to make sure its not coming from other source Pregnancy? Cervical lesion? Assess for anemia � CBC with PLT

AUB Determine ovulatory status- regular menses Y/N? � If uncertain- Day 21 , mid luteal progesterone Screening for Coagulopathy Endometrial sampling- based on risk factors Infectious cause- screening for chlamydia Evaluation for structural abnormalities- polyp, fibroid � TVUS � HSC

AUB Treatment- reproductive age women with benign etiology Based on � Etiology � Severity of bleeding Anemia Interference with ADL’s � Associated symptoms Pelvic pain Infertility � Contraceptive needs and fertility � Underlying risk factors for thromboembolic disease � Patient preference, access to therapy

AUB TREATMENT Treatment should not be initiated until AUB has been evaluated, and malignancy excluded Goal of therapy is to control bleeding Treat anemia Restore quality of life Some satisfied to continue medical treatment Some desire definitive therapy

AUB TREATMENT Treatment is stepwise Primary etiology should be treated Initial approach is pharmacologic treatment Secondary is for those who fail or who cannot tolerate medical therapy � Done childbearing? � Level of invasiveness � Risks of procedure � Surgical intervention options

AUB TREATMENT Ovulatory Dysfunction. Few studies have addressed efficacy of Treatment of AUB-O First line � COCP- 35 -69% reduction � Oral progestin-87% reduction � Contraceptive and regulates bleeding Medroxyprogesterone 10 mg daily for 10 -14 to create predictable withdraw bleed LNG IUD- most effective 71 -95% reduction Creates amenorrhea or scant bleeding Provides contraception Reduce bleeding � Decrease risk of endometrial hyperplasia/cancer � Endometrial ablation not recommended due to risk of hyperplasia with anovulation

AUB TREATMENT Hormonal Treatment COCP first line management � Well tolerated � Few side effects � Regulates bleeding � Lighter flow � Reduction of dysmenorrhea � Contraception Fewer pill free days per pill pack, or continuous cyclic use more effective Can increase risk of Unscheduled or BTB Assess for contraindications of use

AUB TREATMENT LNG-IUD-Levonorgestrel IUD Highly effective Easy to use First line in women who do not desire pregnancy Not effective in women with AUB-O, as does not result in regular bleeding But does reduce risk of hemorrhage, provides protection against hyperplasia Creates amenorrhea or scant bleeding Approved by FDA for HMB

AUB TREATMENT LNG-IUD Cost can prohibit use Reduces blood loss by 71 -95% In studies, it has been found to improve quality of life Long adjustment period- especially with women with adenomyosis Consider expulsion rate Congenital or acquired endometrial distortion is a contraindication for placement

UTERINE ABNORMALITIES

AUB TREATMENT DMPA- Depo Provera Used for women with AUB who have contraindications or prefer to avoid use of estrogen Not an option for women trying to conceive Become amenorrheic after 4 injections = 1 year

AUB TREATMENT High Dose Oral Progestins Used in women who have contraindications to or prefer to not use estrogen � Norethindrone Acetate- 5 mg 1 -3 tablets daily � Medroxyprogesterone Acetate- 5 -30 mg daily Contraception required with these doses Can cause bloating, dysphoria, increased appetite Taper dose of norethindrone after no bleeding Norethindrone has more potent endometrial suppression Mini Pill or Nor QD 0. 35 mg has not been studied for effectiveness Continuous dosing more effective than cyclic dosing

AUB TREATMENT Tranexamic Acid Option for women who don’t want hormones, or has contraindication to them Antifibrinolytic agent that competitively blocks conversion of plasminogen to plasmin reducing fibrinolysis. Approved by FDA for treatment in 2009 May be used while attempting fertility

AUB TREATMENT Tranexamic acid Cost and availability varies- US expensive, Sweden available over the counter Risks for thrombosis Anemia already present due to bleeding is thought to play a role regardless of medication use Dosing � 1300 mg (2) 650 mg tablets three times a day for as long as 5 days during menstruation � Dose needs adjusted with impaired renal function

AUB TREATMENT NSAID’s � Nonhormonal � Noncontraceptive � Reduction of menstrual blood loss by causing a decline in the rate of prostaglandin synthesis in the endometrium, leading to vasoconstriction, therefore reducing bleeding Advantage � Do not increase risk of thrombosis � Low risk of SE � Reduction of dysmenorrhea � Low cost, Available OTC � Not needed daily

AUB TREATMENT NSAID’s Best if started a few days prior to menses and continued through menses Mefenamic Acid- Ponstel 500 mg TID Naproxen 500 mg BID Ibuprofen 600 mg TID Other NSAID”S Diclofenac Meloxicam

AUB TREATMENT Surgical Approach � Provides long term efficacy � Definitive therapy � Avoid medication side effects Adenomyosis and fibroids most common reason for definitive surgery If preservation of fertility desired, myomectomy can be performed Will likely need C Section for delivery after myomectomy
")
AUB TREATMENT Endometrial ablation- pregnancy contraindicated after ablation, contraception required ( BTL, Spouse vasectomy) Uterine artery embolization- option with fibroids Safety for pregnancy after this procedure not established Hysterectomy � Definitive surgery � High rate of satisfaction � Curative � Performed after failure of medical management and no future fertility desires

ADOLESCENT AUB First year, 50% of cycles are anovulatory Due to endometrium lacking stabilizing effect of progesterone Due to this, the endometrium becomes excessively thickened The endometrium proliferates beyond the ability of estrogen to maintain its integrity

ADOLESCENT AUB Most common cause � Anovulatory cycles, related to immaturity of the hypothalamic-pituitary- ovarian axis � Pregnancy � Bleeding disorders � PCOS � Thyroid dysfunction � Hypothalamic dysfunction- stress, exercise excess, acute weight loss or obesity � Hormonal , intrauterine contraception � Infection

ADOLESCENT AUB Assessment Hemodynamic stability Urine pregnancy test History Menstrual History � � Age of menarche Menstrual pattern Symptoms Events leading to change of bleeding Sexual Hx PMH- medications ROS- wt change, acne, hirsutism, HA, galactorrhea Social Hx Family Hx

ADOLESCENT AUB Physical exam Body type- turner syndrome Androgen excess- hirsutism, acne Optic exam- pituitary tumor Sexual maturity- tanner staging Skin- acanthosis nigricans, ecchymosis, petechaie Abdomen- Mass, pregnancy External genitalia Pelvic exam- with caution and need Pelvic US Labs

ADOLESCENT AUB Diagnostics FSH TSH Prolactin Testosterone PCOS lab CBC Consider Endometriosis Bleeding disorders

Abnormal Uterine Bleeding Risk Factors Excessive Estrogen: 1. Obesity – BMI >35 2. PCOS 3. Anovulatory menstrual cycles 4. Tamoxifen 5. Any unopposed estrogen Abnormal Uterine Bleeding No or >12 months since previous sample >/= 45 yo 35 -45 yo Office endometrial biopsy Insufficient cellularity Adequate pipelle without tissue return Intra-op gross with frozen if indicated With risk factors Failed Bx Normal/atrophic office hysteroscopy Further sampling not required D&C hysteroscopy Same as >45 yo <35 yo Without risk factors Routine sampling not required

Failed Endometrial Ablation No or >12 months since previous sample Without Vaginal Bleeding With Vaginal Bleeding >/= 45 yo 35 -45 yo Office endometrial biopsy With risk factors Failed/Insufficient cellularity Intra-op gross with frozen if indicated Office endometrial biopsy Failed/insufficient cellularity Intra-op gross with frozen if indicated <35 yo Routine sampling not required Without risk factors Routine sampling not required >/= 45 yo Intra-op gross with frozen if indicated 35 -45 yo With risk factors Intra-op gross with frozen if indicated <35 yo Without risk factors Routine sampling not required

Uterine Fibroids Do not send gross specimen Morcellation anticipated Intact specimen anticipated Follow AUB guidelines for sampling D&C frozen preferred Consider endo bx pipelle for frozen Remove and send cervix as separate specimen Intra-op gross with frozen if indicated
. Management of abnormal uterine bleeding. Retrieved September")
REFERENCES Kaunitz, A. M. (2017, June 7). Management of abnormal uterine bleeding. Retrieved September 9, 2017, from www. uptodate. com De Silva, N. K. , M. D. (2017, June 12). Abnormal uterine bleeding in adolescents: Evaluation and approach to diagnosis. Retrieved August 8, 2017, from www. uptodate. com Sweet, M. D. (2012, January 1). Evaluation and Management of Abnormal uterine bleeding in premenopausal women. American Family Physician, 81(1), 35 -43. Munro, M. G. , Critchley, H. O. , Broder, M. S. , & Fraser, I. S. (n. d. ). FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in non gravid women of reproductive age. International Journal of Gynecology and Obstetrics, 113, 3 -13. doi: 10. 2016/j. ijgo. 2010. 11. 011

REFERENCES Management of acute abnormal uterine bleeding in nonpregnant reproductive-aged women. Committee Opinion No. 557. American College of Obstetricians and Gynecologists. Obstet Gynecol 2013; 121: 891– 6 Denyer, R. (204, September 16). Menstruation, Ovulation and ovulatory Dysfunction. Retrieved September 21, 2017, from http: //omega-labs. co. za/menstruation-ovulatorydysfunction/
- Slides: 55