With venous TOS and subclavian vein thrombosis For

With venous TOS and subclavian vein thrombosis. For the majority of the patients thrombolytics are of no benefit. How the condition should be treated. George Geroulakos Professor of Vascular Surgery, National and Kapodistrian University of Athens, Greece

Congenital abnormal lateral insertion of the costoclavicular ligament and hypetrophy of the scalenous anterior in the Paget-Schroetter syndrome. (Urschel , 2008)

• A recent Cochrane data base systemic review determined that there is currently insufficient evidence from which to draw conclusions on the benefits or harms of thrombolysis in the treatment of individuals with acute UEDVT Cochrane Database Syst Rev 2017 Dec 11; 12: CD 012175

Despite of this conclusion a series of recent articles and reviews suggests that in acute cases of UEDVT immediate thrombolysis should be performed: • Kair G, Blair M. Management strategy for patients with chronic subclavian vein thrombosis. Ann Thorac Surg 2017; 103: 672 -5 • Ozcinar E, Yaman ND, Cakici M, Baran C, Inan MB, Durdu S, Akar R, Sirlak M. Pharmacomechanical thrombectomy of upper extremity deep vein thrombosis. Int Angiol 2017; 36: 275 -280. • Mahmoud O, Vikatmaa P, Räsänen J, Peltola E, Sihvo E, Vikatmaa L, Lappalainen K, Venermo M. Catheter-Directed Thrombolysis vs. Pharmacomechanical Thrombectomy for Upper Extremity Deep Venous Thrombosis: Cost-Effectiveness Analysis. Ann Vasc Surg. 2018; 51: 246 -253

• Therefor thrombolysis remains a controversial issue and a reappraisal on the place of thrombolysis for the management of patients withprimary UEDVT is clinically relevant.

In a case control study 45 consecutive patients who had been treated for primary UEDVT received either • oral anticoagulant therapy only (n=14, group 1); • thrombolysis followed by anticoagulant therapy (n=14, group 2); • or thrombolysis, transaxillary first rib resection and anticoagulant therapy (n=17, group 3)7. Endpoints were persisting symptoms and quality of life (Qo. L).

• Patients in groups 2 and 3 had significantly less pain, swelling and fatigue in the afflicted limb at six weeks. • There was no difference in pain (P=0. 90), swelling (P=0. 58), fatigue (P=0. 61), functional impairment (P=0. 61), recurrence (P=0. 10) or Qo. L (P=0. 25) between groups at the end of follow-up (mean follow-up 57 months [range 2 -176, SD± 46]). Treatment strategy was not predictive of Qo. L (P=0. 91, analysis of variance). • No differences in long-term symptoms or Qo. L between patients with successful and unsuccessful thrombolysis were present. Bosna et al; Vascular 2011

• In a retrospective analysis of 103 patients who had 110 first rib resections, 45 subclavian veins underwent thrombolysis with or without venoplasty prior to first rib resection and were compared to 65 subclavian veins on preoperative anticoagulation alone. Guzzo et al; J Vasc Surg 2010
 were patent with")
• Of the veins that underwent endovascular treatment 91% (41/45) were patent with improvement of symptoms at one year. In the group of veins that underwent anticoagulation alone prior to first rib resection at follow up 91% (59/65 ) were patent with symptomatic improvement. Guzzo et al; J Vasc Surg 2010

Risk of bleeding Using data from 29 studies and a total of 2000 patients showed that major bleeding (MB) was similar amongst patients treated with anticoagulation alone, compared to patients treated more aggressively with thrombolysis and/or surgery (i. e. thoracic outlet decompression). The pooled proportion for MB was 5. 0% (95% CI 0. 3– 9. 7) after anticoagulation alone and 3. 8% (95% CI: 2. 4– 5. 8%) after thrombolysis and/or surgery. Thiyagarajah et al, Thromb Res 2019

• 54 patients with primary UEDVT who were treated with anticoagulation alone and were seen in an 18 year period. 49 patients who attended a follow up visit underwent ultrasonography (mean follow up 5 years). • Scores of severity of postthrombotic symptoms were graded in a numerical scale ranging from 1 to 10 and correlated to u/s findings graded from 0 to 2. • There was no relation between the severity of symptoms and ultrasonographic findings. Heron et al; Ann Int Med 1999

Conclusions • It seems that the use of thrombolysis in UEDVT should be used with caution in carefully selected patients till level I evidence determines the validity of this approach in the management of the full spectrum of patients with UEDVT.

• This cautious approach is also adopted by the 2012 ACCP guideline that has averted clinicians from performing routine thrombolysis in patients with primary UEDVT and should be restricted to very few cases if any. Our reappraisal of the most recent literature suggests that this guideline is still valid. Guyatt et al, Chest 2012

• Thrombolysis may be considered in young and active patients within the first 2 weeks from upper extremity deep vein thrombosis, who have severe symptoms and attach high value in the prevention of post thrombotic syndrome and understand the complexity and complications of thrombolysis. • All patients should receive anticoagulation for at least 3 months


Does the first rib routinely need to be removed after thrombolysis?

In a mataanalysis of 12 series patients following thrombolysis within the first 2 weeks were divided in 3 groups: • First rib resection n=448 • First rib resection and venoplasty n=68 • Thrombolysis with no first rib resection n=168 Lugo et al; Ann Vasc Surg 2015

• Symptom relief at last follow up was significantly more likely in the first rib resection group (95% ) and the first rib resection and venoplasty group (93%) rather than the rib not removed group (63%). • 40% of the patients in the rib not removed group eventually required surgery for recurrent symptoms. Lugo et al; Ann Vasc Surg 2015

• First rib may be considered following upper extremity deep vein thrombosis in patients who remain symptomatic following anticoagulation for 2 -3 months, if positional venography demonstrates narrowing of the subclavian vein.
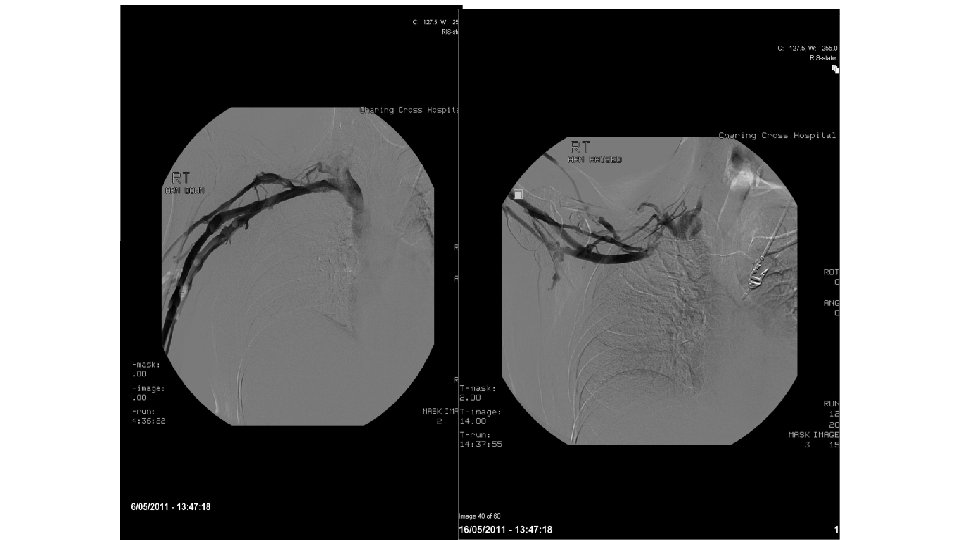

Paget-Schroetter syndrome therapy: failure of intravenous stents. • 22 patients had intravenous stents placed post-thrombolysis for Paget-Schroetter syndrome. All had post stent anticoagulation. In all patients the subclavian vein reoccluded 1 day to 6 weeks after stent insertion. Urschel HC et al, Ann Thorac Surg. 2003

• Primary subclavian vein stents are not recommended for venous thoracic outlet syndrome before surgical decompression by first rib resection due to a high risk of fracture because they are compressed between the clavicle and first rib.

Leandro Barreras Molinelli, José N. Allende European Journal of Vascular and Endovascular Surgery Volume 55, Issue 2, (February 2018) DOI: 10. 1016/j. ejvs. 2017. 09. 006 European Journal of Vascular and Endovascular Surgery 2018 55, DOI: (10. 1016/j. ejvs. 2017. 09. 006)
- Slides: 23