WIDE COMPLEX TACHYCARDIA Puja Chopra PGY1 Emergency Medicine
























- Slides: 38
WIDE COMPLEX TACHYCARDIA Puja Chopra, PGY-1 Emergency Medicine May 19, 2011
Objectives Differential Diagnosis of wide complex tachycardia Approach to wide complex tachcardia Examples of wide complex tachycardia Adenosine/ACLS
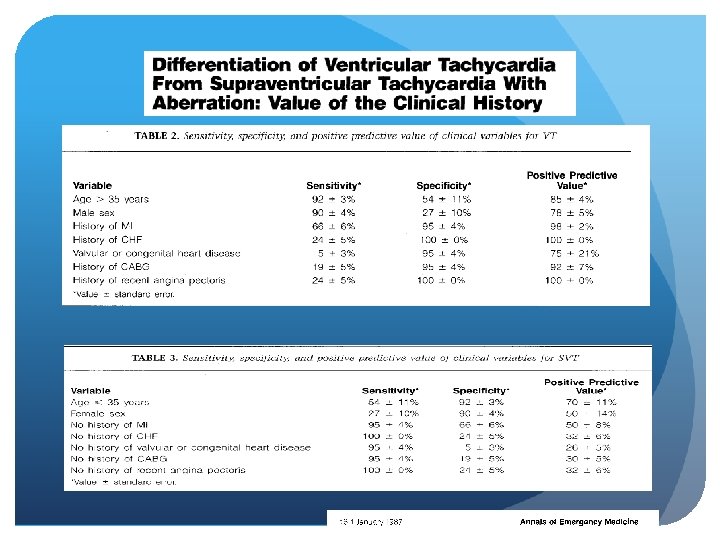
DDx: Ventricular tachycardia SVT with a preexisting bundle branch block or a functional rate related bundle branch block SVT with antegrade conduction via an accessory pathway Drug induced – TCA, Class one antiarryhtmic Electrolyte - hyperkalemia
Wellen’s Criteria RBBB Pattern LBBB Pattern
Sensitivity: 98. 7% Specificity: 96. 5%
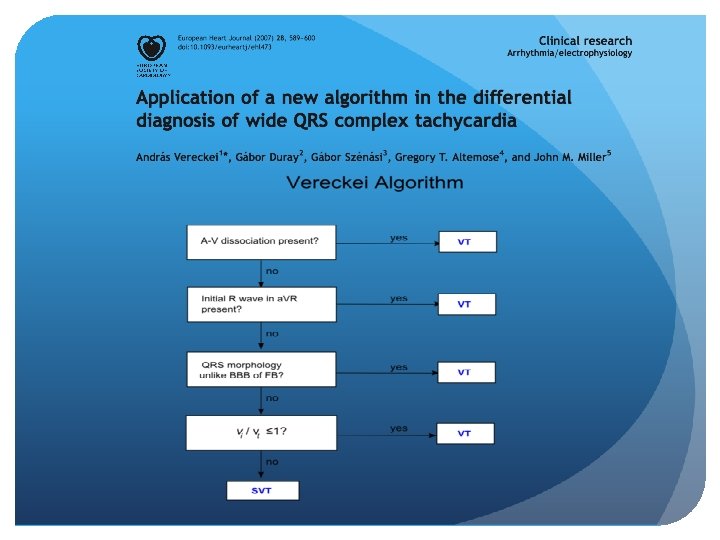
Brugada Criteria: -Sensitivity: 79 to 91% -Specificity: 43 to 70%
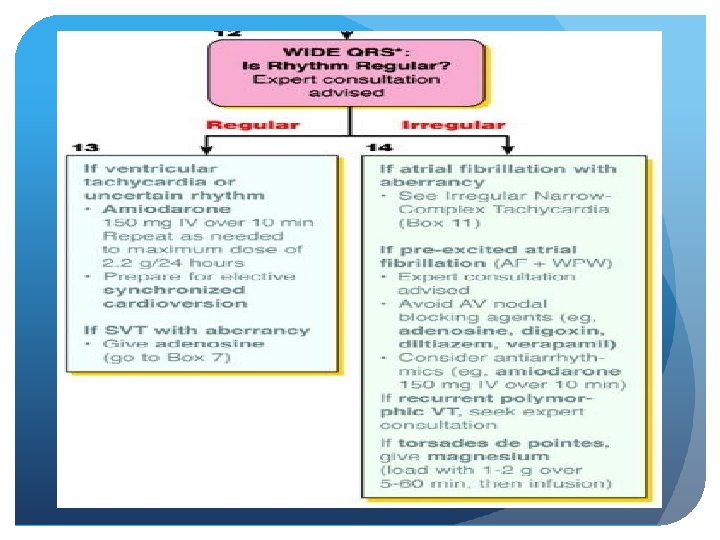
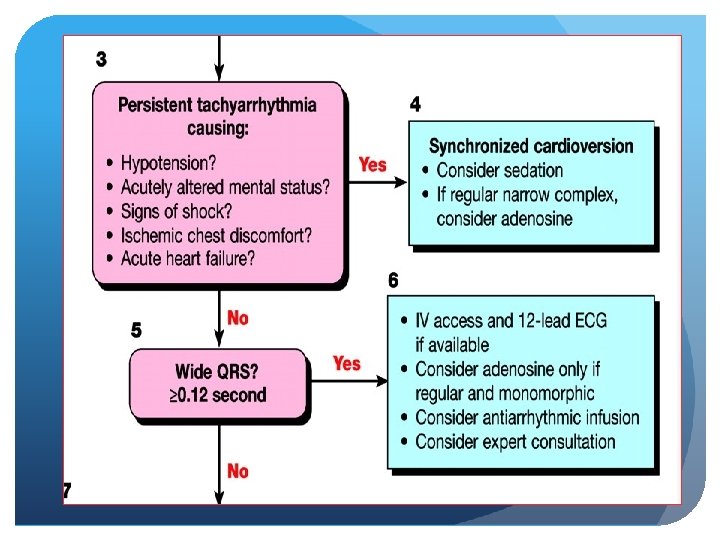
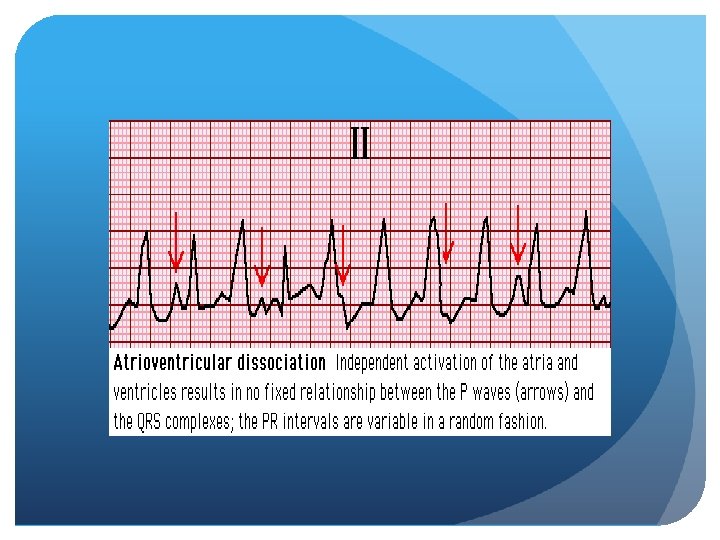
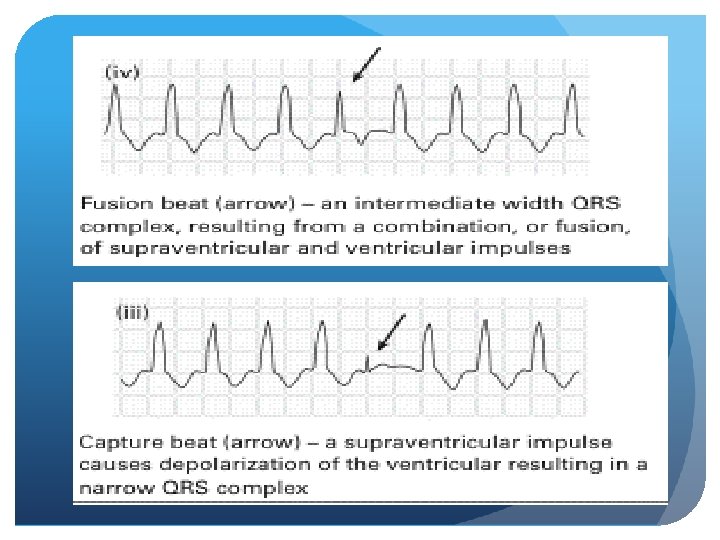
Approach to WCT 1. History 2. Physical Exam 3. ECG Regular: VT, SVT with aberrancy, SVT with accessory pathway, Electrolyte abnormalities, Medications Irregular: a fib + pre-excitation, a fib + BBB, a flutter + BBB, MAT + BBB, polymorphic Vtach (torsades) ? AV dissociation, Fusion beats, capture beats 4. Adenosine (? Diagnostic, ? therapeutic)
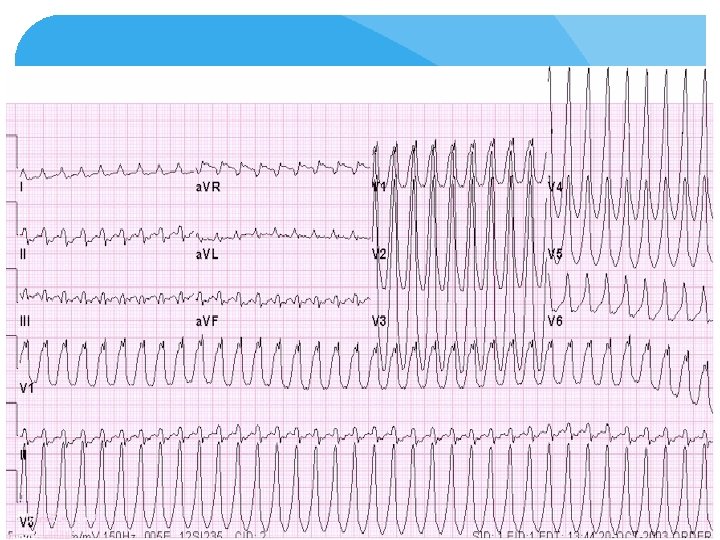
70 yo male with palpitations and history of angina
61 yo male with productive cough and fever
65 yo male with syncope, PMHx: DM
30 yo female with palpations
30 yo female with palpations
28 yo male, altered and agitated after an unknown overdose
45 yo male, previously healthy, with palpitations
44 year old chronic alcoholic male with persistent vomiting and becomes unresponsive
65 yo female with palpations
48 yo male with palpitations
Adenosine in the Diagnosis of Broad Complex Tachycardia - Griffith et al. The Lancet March 1988 89% Sensitivity, 95% specificity, 92% predictive accuracy for SVT origin Broad Complex Tachycardia SVT VT 8/9 1/17 Atrial Fibrillation with WPW 0/6 No change in mean RR
Intravenous Adenosine Triphosphate During Wide QRS Complex Tachycardia: Safety, Therapeutic Efficacy and Diagnostic utility - Sharma et al. The American Journal of Medicine, April 1990 Sensitivity: 70%, Broad Specificity: 92%, PPV: 85% Complex Tachycardia SVT not requiring the AV node 1/10 Significant shortening of RR interval VT SVT requiring the AV node 1/14 7/10
Adenosine for the Management of Patients with Tachycardias – A new Protocol - Domanovits et al. European Heart Journal, 1994 Wide Complex Tachycardia SVT VT Afib/Aflutter with aberrancy 17/22 0/4 0/3
Adenosine For Wide Complex Tachycardia: Efficacy and Safety - Marill et al. Critical Care Medicine, 2009 Regular Wide Complex Tachycardia Primary outcome: termination of tachycardia with adenosine, AV block allowing rhythm identification - The odds of SVT increase by a factor of 36 after a positive response to adenosine SVT VT 104/116 2/81 - Odds of VT increase by factor of 9 after a negative response to adenosine
Thanks! Questions?