WHY In lowtech area However newer technology doesnt














 – Non adherence to standards")
 Non adherence to standards and procedures this")
 Unawareness - this can include breakdown of")




, the biggest challenge to")




 • 醫療不良事件(Medical adverse event) • 警訊事件(Sentinel event) 醫策會2005")




















- Slides: 62
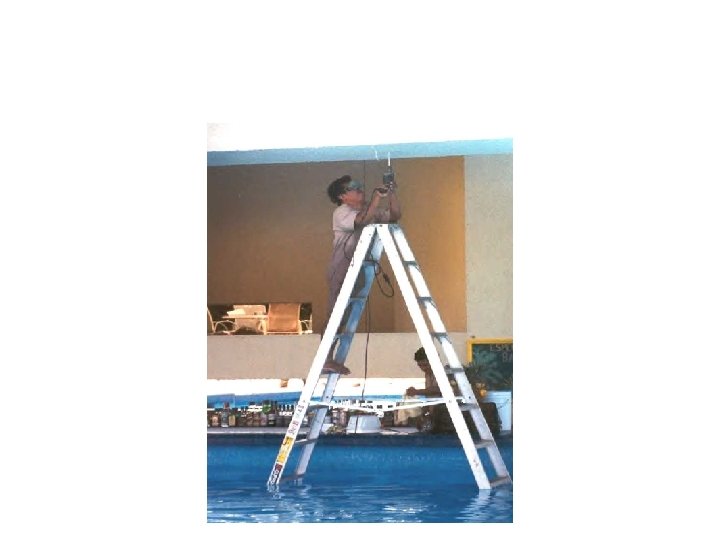
WHY ?
In low-tech area. . .
However, newer technology doesn’t eliminate error
Nor does even newer technology
What is CRM? Using all the available resources – information, equipment, and people – to achieve safe and efficient flight operations” John Lauber(1977)
What is CRM Training ? CRM training provides a set of countermeasures against human error ; it is based on the premise that human error is ubiquitous and inevitable. (透過訓 練杜絕以往認為是不可避免、比比皆是的人為疏失) Dr. Helmreich (1996)
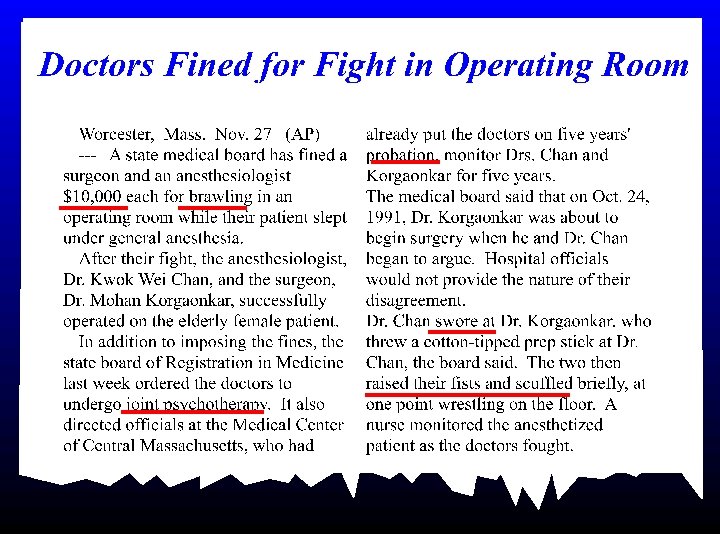
AVIATION vs. MEDICINE 當白袍映上藍天… So different, yet so similar
Detroit News and Free Press. Sunday, February 6, 2000.
RAND Study: Quality of Health Care Often Not Optimal Patients’ care often deficient, study says. Proper treatment given half the time. On average, doctors provide appropriate health care only half the time, a landmark study of adults in 12 U. S. metropolitan areas suggests. Medical Care Often Not Optimal Failure to Treat Patients. Fully Spans Range of What Is Expected of Physicians and Nurses Medical errors corrode quality of healthcare system Study: U. S. Doctors are not following the guidelines for ordinary illnesses The American healthcare system, often touted as a cutting-edge leader in the world, suddenly finds itself mired in serious questions about the ability of its hospitals and doctors to deliver quality care to millions.
To make people change … YOU MAKE ERRORS !
Human Error Type • H 1 - Active Failure-(Aware) – Non adherence to standards and procedures – 明知故犯 • H 2 - Passive Failure-(Unaware) – breakdown of coordination, misunderstanding, communication failures, lack of expected support – 無心之過 • H 3 - Proficiency Failure – Inappropriate handling of its systems – 力有未逮 • H 4 – Incapacitation – physical or psychological inability – 失能
H 1 - Active Failure 明知故犯 (Aware) Non adherence to standards and procedures this can include non adherence to SOP, law violations, failure to follow written instructions, failure to manage cockpit resources, gross lack of appropriate vigilance, laziness.
H 2 - Passive Failure 無心之過 (Unaware) Unawareness - this can include breakdown of coordination, misunderstanding, communication failures, lack of expected support, - it can be exacerbated by high workload, distraction, complacency, forgetfulness, boredom, low arousal level.
H 3 - Proficiency Failure 力有未逮 Inappropriate handling of aircraft or its systems - this can include misjudgment, making an incorrect decision - it can be exacerbated by lack of experience, lack of training or simple incompetence.
H 4 – Incapacitation 失能 Flight crew member unable to perform his/her duty due to physical or psychological inability.
To make people change , what we need is … SAFETY CULTURE • It is the mindset & commitment to pursuit safety, which requires nonstop efforts. (心態、承諾、契而不捨的追蹤)
Culture Definitions • Usually based upon a blend of visionary ideas, corporate culture appears to reflect shared behaviors, beliefs, attitudes and values regarding organisational goals, functions and procedures which are seen to characterise particular organisations – Furnham, A. , Gunter, B. , 1993. Corporate Assessment. Routledge, London.
Culture and Safety According to the Institute of Medicine (IOM), the biggest challenge to moving toward a safer health system is changing the culture from one of blaming individuals for errors to one in which errors are treated not as personal failures, but opportunities to improve the system and prevent harm
A Safety Culture is…… • Constant awareness of potential for things to go wrong(持續 監察潛在性問題進展為錯誤) • Culture that is open and fair(文化是開放和公平的) • Culture that encourages people to speak up about mistakes(文化是讓人有有勇氣說出錯誤) • Able to learn about what is wrong and then put things right(是爲了學習作對的事) NPSA
Swiss Cheese Model If all the barriers are failed. . providers patients Procedure policy Peripherals products Accident The truth is…. . ↗醫療事件錯誤事件是一連 串疏失所造成 ↗ 多半的醫療不良事件並 非個人疏忽或缺乏訓練 ↗ 75%的醫療問題來自系 統的錯誤
Stop the error ! defences, barriers and safeguards providers patients Procedure policy Peripherals products Active failures Latent failures
Patient Safety: Leadership Role • Our systems are too complex to expect merely extraordinary people to perform perfectly 100 percent of the time. We as leaders have a responsibility to put in place systems to support safe practice. ” * • . 90 X. 90 =. 65 or 65% ** Leadership Guide to Patient Safety, Institute for Healthcare Improvement, 2005
醫療異常事件 • 醫療錯誤(Medical error) • 醫療不良事件(Medical adverse event) • 警訊事件(Sentinel event) 醫策會2005
Patient Safety is No Accident
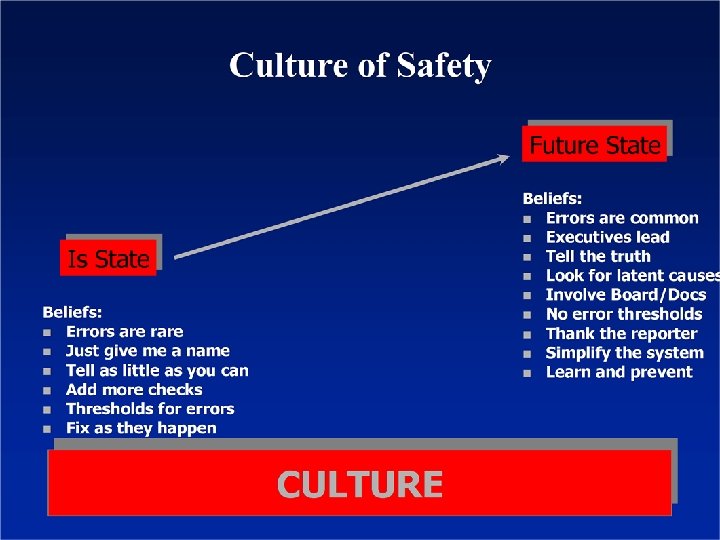
Creating a Culture of Safety
如何提昇安全文化� 四要素� • Reporting culture 建立信任的機制 • Justice culture 懲罰與歸責的拿捏 • Flexible culture 面對改變能及時與有效的應對 • Learning culture 觀察、反應與分析、創新、行動 Source: James Reason, managing the risk of organizational accidents
Safety – Comprised of Many Pieces Educate Report Analyze Trust Inform
Safety – Putting it All Together Educate Inform Trust Analyze Report More than a program… Safety is a way of life
改變安全文化的要點 • • TEAM WORK LEADER SHIP WORKLOAD MANAGEMENT COMMUNICATION
The Role of the Patient Safety Manager
Seven steps to patient safety
Step One Build a safety culture 建立開誠佈公的病安文化
Create a culture where safety is considered in everything they do
Step Two Lead and support staff 領導者對病安的堅持與支持
Lead and support your staff
Step Three Integrate your risk management activity 整合風險管理
Step Four Promote Reporting 鼓勵通報
Spot and report mistakes when they happen
Step Five Patient And Public Involvement 鼓勵民眾共同參與病安 作
Step Six Learn and share safety lessons 學習並分享病安 作成效 Root Cause Analysis
Step Seven Implement solutions to prevent harm 提供解決方案避免病安傷害
Make solutions simple and intuitive