Why do we have emotions What purposes do


")










- Slides: 14
Why do we have emotions? What purposes do they serve?
Emotions – feelings; also: • Physiological: internal physical changes • Brain: cerebral cortex, limbic system, amygdala • Autonomic Nervous System: heart rate, breathing, trembling, stomach • Cognitive: thoughts, values, expectations influence type & intensity • Behavioral: (non verbal) expressions, body position, touch, eye gaze, tone
Primary Emotions (universal)
We are born with the ability to mimic facial expressions
Emotional Display • Complex emotion requires experience & brain development • Birth - 6 months • Display interest, distress, disgust, contentment • Respond to happy, angry, sad faces of others • 7 months - 1 year • More emotions, social referencing • 1 - 3 years • Secondary emotions (envy, embarrassment), empathy, sharing • 3 - 6 years • Masking emotions, cultural display rules
Theories of Emotion • James-Lang: physiological arousal -> reaction • Ex. Feel sad because we are crying • Schachter’s Two Factor: 1) physical arousal 2) cognitive labeling • Ex. Dentist • Cannon-Bard: simultaneous arousal, behavior, and emotion • Ex. Shark
Dislike • Think about the last time that you met someone and disliked them. What didn’t you like about them? • Impressions, reactions are almost entirely emotional
Emotion - Application • First impressions • Teachers • Employment • Pain • • Broken leg Broken heart Wisdom tooth surgery Death of a loved one • Love • Drugs & Emotion
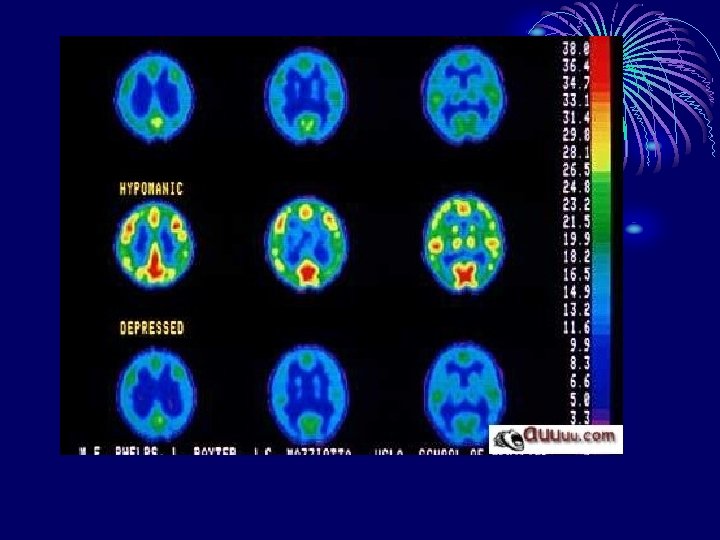
Mood Disorders • Major Depression • Recurrent episodes of 5+ of despair, hopelessness, worthlessness, loss of interest in activities/people, negative self-evaluations, guilt, suicidal thoughts, loss of appetite, sleep disturbances, bodily pain • Episodic Depression • 1 episode of 2+ weeks of depressive symptoms • Bipolar Disorder • cycles of mania & depression: mania = inappropriate emotion, euphoria, extreme irritability, extreme anxiety, grandiosity, flight of ideas, goal-directed activity, impulsivity, excessive talkativeness, high risk pleasurable behavior
Mood Disorders • Biological Factors: disordered frontal lobe or gray matter, genetic predisposition, NT imbalance (depression: too little SE, DA, NE, mania: too much SE, DA) • Environmental Factors • Depression: learned helplessness, internal, stable, and global attributions, role transitions, grief • Bipolar Disorder: stress • Treatment • Mood stabilizers, (extreme) exercise, diet, stress management, cognitive restructuring, interpersonal or family therapy, ECT (rare), deep brain stimulation
Normal Depressed
Mania “When I'm manic, I'm so awake and alert, that my eyelashes fluttering on the pillow sound like thunder” – Andy Behrman Those who enjoy or are productive with manic symptoms likely to stop treatment More mania = more depression, more likely to commit suicide
Prognosis Major Depression Untreated likely to have symptoms for life Drugs short-term then stop 80% relapse Maintenance drugs 50% relapse Drugs + psychotherapy 35% relapse Psychotherapy effective in 16 weeks Bipolar Disorder Maintenance drugs or symptoms for life Psychotherapy to reduce episodes, severity, manage relationships