Where will retinal screening go Graham Leese Ninewells




")

 Pale blue: Type-1 diabetes Dark blue: Type-2 diabetes Duration")



 from baseline “no retinopathy")

 Annual")




")


 Fewer referrals b) Can discharge more from Eye Clinic")
: Licenced Bevacizumab (Avastin): Cheap")































")


- Slides: 61
Where will retinal screening go? Graham Leese Ninewells Hospital Dundee Lead Clinician for DRS in Tayside
Exciting times • • • Screening Intervals OCT in screening Anti-VEGF treatment Automated grading Reaching the unreachable
Why do we screen annually? Always Been so Easy to organise Fits in with Annual visits to Doctor PRACTICAL REASONS Not EVIDENCE BASED REASONS
Retinal Photography Screening IT call/recall systems Chance to change Annual Routine
Wisconsin: Incidence at 4 year from Diagnosis % N=<996 N=<1370 Wisconsin II, IV (1984)
“Reclaim Democracy”
Prevalence of Proliferative Retinopathy (%) Pale blue: Type-1 diabetes Dark blue: Type-2 diabetes Duration Kristinsson et al 1997
1994: National Retinal Screening Scheme Slit Lamp every 2 years if no baseline retinopathy 10 yr review in 2007 of 296 patients: 23 pre-proliferative, 4 proliferative 4 Macular oedema - all in eye clinic before treatment req’d Olafsdottir et al BJO 2007
Progression of Retinopathy: T 2 Diabetes: Newly Diagnosed: No baseline retinopathy UKPDS: n=2316 % needing laser 1. 1% 0. 2% Kohner et al UKPDS 52 Diab Med 2001
Progression of Retinopathy Any Type-2 diabetes: No baseline retinopathy Liverpool Eye Study: n=9890, 20570 screening events % with ST eye disease 1. 4% 0. 5%* 0. 3% ST-retinopathy Younis et al Lancet 2003
Screening Interval: Type-1 Diabetes Incidence of ST eye disease (%) from baseline “no retinopathy ” N=501: 2742 screening events 2. 6% 1. 6% 0. 6%* 0. 3% ST retinopathy Younis et al 2003, Diab Med
Progression at 3 years Type-2 Diabetes: No baseline retinopathy % progressed N=1322 0. 2%* *Only ONE eye required laser Nb: Hb. A 1 c = 46 mmol/mol / 6. 4% Agardh et al Diab Care 2011
Incidence of Retinopathy No baseline Retinopathy: T 2 diabetes N=57, 199 (87% follow-up) Annual Incidence per 100 patients 0. 2 0. 35 Thomas et al BMJ 2012
Incidence of Retinopathy No baseline Retinopathy: T 2 diabetes Outcome at 5 YEARS Incidence per 100 patients N=16, 444 Norfolk 0. 68 Jones et al Diab Care 2012
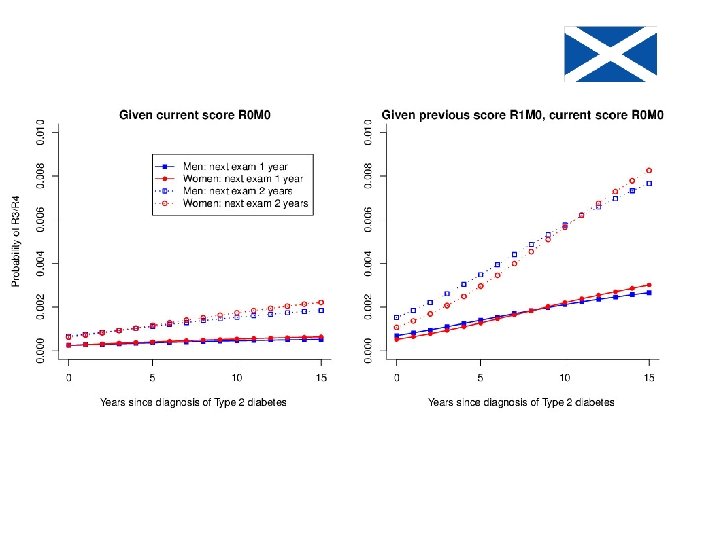
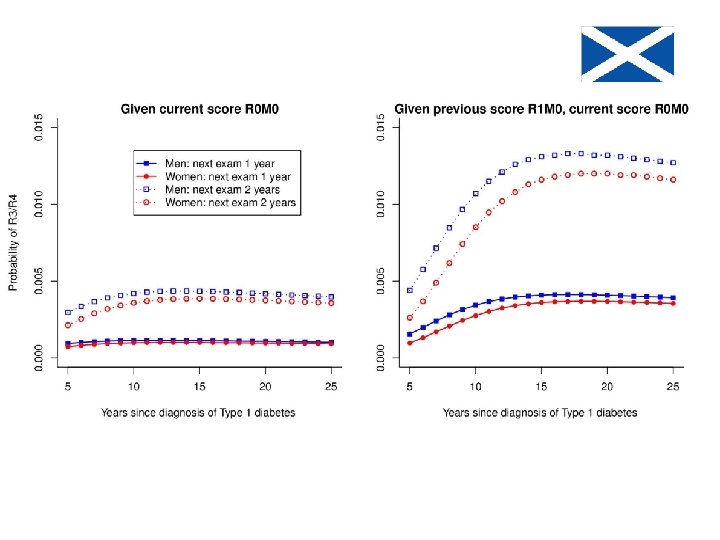
Progression in Type 1 diabetes from no baseline retinopathy: DRS Scotland % N=7869 0. 5 0. 7
Progression in Type 2 diabetes from no baseline retinopathy: DRS Scotland % N=101, 539 0. 13 0. 22
Cost-effectiveness of retinal screening: 1 vs 3 years AGE 45 yr 65 yr Hb. A 1 c 11% (97 mmol/mol) 7% (53 mmol/mol) Days of sight 21 saved (1 vs 3 yr) 3 Cost per QALY £ 27, 000 (1 vs 2 yr) £ 141, 000 Vijan et al JAMA 2000
Use of Optical Coherence Tomography (OCT)
Macular Disease • 80% of referrals are for maculopathy • 80%+ of these do not require treatment (at time of referral) • At least 65% of referrals unnecessary • Eye Clinics overloaded • ISMO trial – looking at the use of OCT in screening
Retinal Screening M 2 result 100% Retinal Screening M 2 Result OCT screening 20% Eye Clinic Incorporation of OCT step within screening programme
Double Benefit a) Fewer referrals b) Can discharge more from Eye Clinic
Intra-vitreal VEGF therapy Ranibizumab (Lucentis): Licenced Bevacizumab (Avastin): Cheap
Diabetic Macular Oedema • Proven benefit in clinical trials • NICE reviewing use of Lucentis (31/10/12) - 400μm central thickness - company discount - ? For 6/18 vision
BACKGROUND • New Treatment option • 5 maculopathy referrals for 1 proliferative QUESTIONS • More important to look for maculopathy? - more treatable • Less important to look for maculopathy? - becomes a symptomatic condition
AUTOMATED GRADING
Automated Grading EQA results Q 3 2012 Centres Autograder Sensitivity 88. 6 -95. 5% Specificity 87. 0 -97. 8% 34. 8%
What are we trying identify? What are we expected to identify? Non-diabetic pathology? Who does what?
ANNUAL
AUTOGRADING ………. and its getting better all the time!
Sensitivity / Coverage • • • Screening Intervals OCT in screening Anti-VEGF treatment Automated grading Reaching the unreachable
Number of people with Diabetes in Tayside 1. 8% 2. 9% 4. 0% Numbers doubling every 9 -10 years 4. 8%
NUMBER OF PATIENTS RECEIVING LASER IN TAYSIDE Number of patients receiving laser 62% reduction Number of patients with diabetes (x 100) 60% increase Vallance et al Diab Care 2008
PERCENTAGE OF PATIENTS RECEIVING LASER % of patients receiving laser 2. 5 fold reduction for both % of patients receiving incident laser Vallance et al Diab Care 2008
Prevalence of Blindness in Scotland due to Diabetes Rate per 10, 000 Scottish Diabetes Survey Figures
Prevalence of Blindness in Scotland due to Diabetes Rate per 10, 000 Fife Scottish Diabetes Survey Figures
Visual Outcomes • One episode of missing eye screening: 3. 1 x increased risk of laser Leese et al Diab Care 2008 • From 1990 -1995 16/17 Diabetes related blindness was due to poor attendance Rhatigan et al Eye 1999 • From 1990 -1999 the majority of blindness due to diabetes related to poor attendance Cormack et al BJO 2001
RISK FACTORS FOR NON-ATTENDANCE
Geography & Screening Uptake BACKGROUND • Tayside, Scotland • Community retinal photography from 1990 • Digital screening from 2000 • Comprehensive annual screening from ~ 2002 • 4. 2% diabetes STUDY • 2004 -2006 • 15, 150 patients, 32, 621 screening episodes • Age 63 years • 7. 3 yrs of diabetes • 54% male • 12% DNA rate Leese et al Diab Care 2008
Clinical Risk Factors Associated with Non-attendance • • • Young age Long diabetes duration High Hb. A 1 c High BP Smoker
Geography and Non Attendance • • GIS: looking at distance and time Average distance to screening 3. 3 miles Average time 11. 7 min (0 - 87. 2 min) Distance or Time NOT associated with attendance • Appointments to mobile Unit: 2. 9 (2. 5 - 3. 4) x more likely not attend eye screening than Static Unit (p<0. 01).
Deprivation as a risk of Non. Attendance * * p<0. 01 * Relative Risk SIMD Deprivation Category Leese et al 2008
Lothian DRS Survey 2011 Interview of 20 DNAs Unaware of Importance 5 Transport problems 4 Other health problems 4 Work 3 Previous negative experience 3 Lack of mobility 2 Caring for others 2 Bereavement 1
Barriers to accessing Eye Care Services: RNIB 2011 Focus Group • Limited awareness of eye health • Symptom led demand for eye examinations • Worry and confusion about costs (what is free and what is not? ) • Services fragmented • Poor interaction with clinicians Bradford, Cwm Taf, Glasgow, Hackney, West Belfast
WHAT MIGHT HELP IMPROVE ATTENDANCE?
Telephone Reminders • Gastroenterology clinic. Call 1 wk prior 25. 3% to 5. 7% DNA rate Scott et al JRSoc. Med 2009 • Rheumatology clinic Gauthier et al J Clin Rheu 2012 72% wanted reminder 1 -4 d before 52% phone call most popular, Unless <28 yr: text was most popular • Four RCTs with 3547 participants Additional phone calls reduce DNA Text as good as phone call Car et al Cochrane Rev 2012
Reducing DNA in General Practice Patients given code to record, made to make verbal or written reminders. Poster with frequency of attendees (not DNAs). Martin et al JRSoc Med 2012
Patient suggestions to improve • • • Evening appointments Link with other appointments Telephone reminders Text reminders Short time scales Patient comments • Confusion with Optician role • Busy people • Local provision valued Lothian DRS survey 2011
Solutions to accessing DRS in Glasgow: RNIB 2011 Focus Group • Screening liked • Confusion about roles of Optometry/GPs/DRS/Eye Clinics • Use local centres e. g. Community Hall • Want general support for Diabetes Care (ie integrate care) • Solutions should build on existing services • Help with language barriers
Are we looking in the right direction for solutions? . . .
Summary: Who is High Risk of Non Attendance?
Summary: What might help? • Telephone and Text reminders • Integrate with other diabetes appointments • Patient to give verbal or written confirmation • • Evening appointments Opportunistic (IP/ OP/ Transition) Local Provision (Mobile unit/Community Hall) Help with Language barriers
IMPACT OF REDUCE UNNECESSARY REFERALS Optical Coherence Tomography (OCT)
Impact of Increased Screening Intervals on Attendance
THANK YOU FOR LISTENING Tayside, Scotland