When Postvention Becomes Prevention Suicide Surveillance and Fatality

When Postvention Becomes Prevention: Suicide Surveillance and Fatality Review to Transform Suicide Victims’ Stories into Stronger Community Responses Debra Darmata, M. S Suicide Prevention Coordinator Washington County Adam Knapp Deputy Medical Examiner Washington County Public Health Kimberly Repp, Ph. D, MPH RAID (Research, Analytics, Informatics, Data) Program Supervisor Washington County Public Health Galli Murray, LCSW Suicide Prevention Coordinator Clackamas County
 Deputy Medical Examiner (DME) Suicide Prevention Coordinator Context:")
Suicide Fatality Review perspectives: Epidemiologist (Epi) Deputy Medical Examiner (DME) Suicide Prevention Coordinator Context: Suicide in Washington County, Oregon Collaboration formation Development of Suicide Fatality Review (SFR) SFR Process SFR Data Integration Lessons Learned

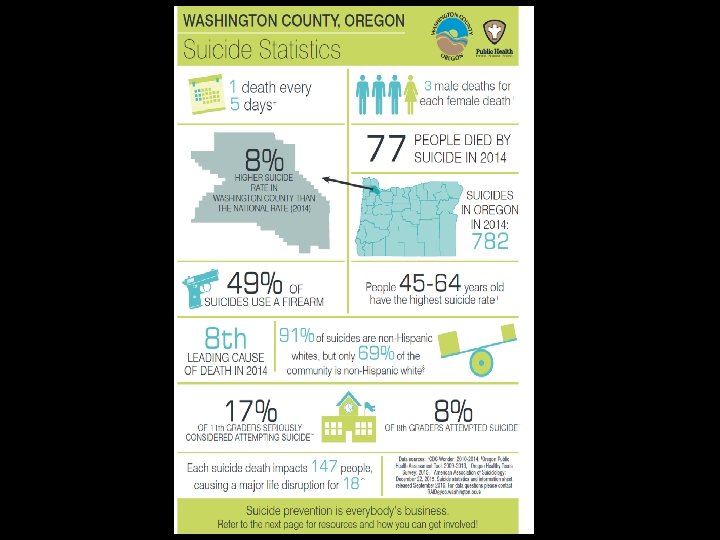
Suicide rates Age-adjusted suicide rate: 2010 -2014 20 18 17. 7 16 14 12 13. 0 13. 3 10 8 6 4 2 0 Washington County Oregon US 2015 -2016 age-adjusted rates per 100 K population per year (CDC) Data: CDC Wonder
 DESIGNATED SUICIDE PREVENTION COORDINATOR (DEC. 2012) SUICIDE")
Suicide prevention 2010 -2012 GLS GRANT (TRAINING) DESIGNATED SUICIDE PREVENTION COORDINATOR (DEC. 2012) SUICIDE PREVENTION COUNCIL (2013) SPC RECOMMENDS CREATION OF SUICIDE FATALITY REVIEW COMMUNITY HEALTH IMPROVEMENT PLAN (DEC. 2014) REGIONAL COMMUNITY HEALTH NEEDS ASSESSMENT RESULTS (MID 2013) GLS GRANT RECEIVED (OCT. 2014 – SEPT. 2019) SFR PLANNING GROUP STARTS MEETING (MID 2013) HIRED DEDICATED SUICIDE PREVENTION COORDINATOR (AUGUST 2015)
 SUICIDE PREVENTION")
Suicide prevention 2010 -2012 GLS GRANT DESIGNATED SUICIDE PREVENTION COORDINATOR (DEC. 2012) SUICIDE PREVENTION COUNCIL (2013) SPC RECOMMENDS CREATION OF SUICIDE FATALITY REVIEW COMMUNITY HEALTH IMPROVEMENT PLAN (DEC. 2014) SFR PLANNING GROUP STARTS MEETING (MID 2013) GLS GRANT RECEIVED (OCT. 2014 – SEPT. 2019) REGIONAL COMMUNITY HEALTH ASSESSMENT RESULTS (MID 2013) HIRED DEDICATED SUICIDE PREVENTION COORDINATOR (AUGUST 2015)
 SUICIDE PREVENTION")
Suicide prevention 2010 -2012 GLS GRANT DESIGNATED SUICIDE PREVENTION COORDINATOR (DEC. 2012) SUICIDE PREVENTION COUNCIL (2013) SPC RECOMMENDS CREATION OF SUICIDE FATALITY REVIEW COMMUNITY HEALTH IMPROVEMENT PLAN (CHIP) (DEC. 2014) SFR PLANNING GROUP STARTS MEETING (MID 2013) GLS GRANT RECEIVED (OCT. 2014 – SEPT. 2019) REGIONAL COMMUNITY HEALTH ASSESSMENT RESULTS (MID 2013) HIRED DEDICATED SUICIDE PREVENTION COORDINATOR (AUGUST 2015)


Risk factors

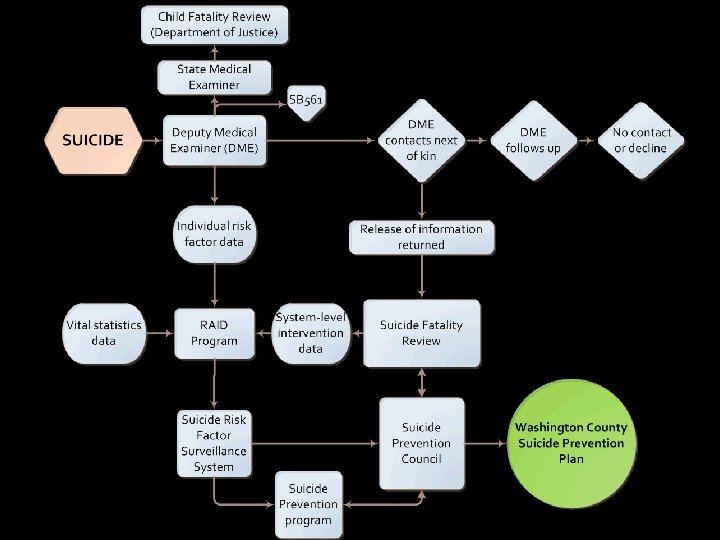
Development of SFR RAID Epi Deputy Medical Examiner Suicide Prevention Coordinator

So what did we have to consider when starting this process? • Could we create a legislative mandate like we have for Child Fatality Review? Not much support • HIPAA violations and family privacy concerns? County council to work on a Release of Information • Confidentiality Statements for board members

What else? • Local Hospitals? Could get patient information but not hospital review of centennial event • How to share and store ME reports with other board members • What kind of review? psychological autopsy? OR child fatality review? OR domestic violence review team? suicide fatality review examples from Michigan, New Hampshire, and Fesno County, CA

What else? - Create a charter: - what is the purpose, goals of the group? - how will we review cases? - roles and responsibilities? - How often are we meeting? - For how long, where?

 Lines for Life (local national")
SFR members Washington County Programs: Community Members: RAID (Epidemiology) Lines for Life (local national suicide prevention lifeline provider) Emergency Medical Services Medical Examiners Mental Health Developmental Disabilities Commitment Team Sherriff's Office District Attorney’s Office Disability and Veteran Services Washington County Crisis Team (contracted to local behavioral health non-profit) School District (mental health care coordinator) Local Chaplin Local Hospital Representative (inpatient behavioral health unit nurse manager) Portland Veteran’s Association (suicide prevention coordinator) Local ambulance services rep Federal Bureau of Investigation (operations specialist

SFR meeting Meeting structure Meets four times yearly for two hours Max of 5 cases reviewed per session Prior to each review, team members sent case files and CRAP form Case review procedure DME reviews case file Team members share their own case-specific information Clarifying questions Protective and Risk Factors Modular Approach RAID team member collects data during meeting Suicide Prevention Coordinator records all recommendations Self care

Protective and risk factor modular approach PROTECTIVE FACTORS Effective clinical care for mental, physical, and substance abuse disorders RISK FACTORS: Social isolation • • Alcohol problem Eviction/loss of home crisis • • • Research training for vision practitioners Work with hospital ED on screening/identification Peer support connection resources through hospital? Screening and interventions for alcohol abuse at hospital What VA services are available? Strong connections to family and community support • • • What kind of support can the • hospital provide? Does hospital have resources to provide? Reduce access to highly lethal means of suicide Training for neighbor • offer QPR for neighborhood watch • groups? Veteran support groups in county- how do they connect with vets? Connect with AA and similar programs to provide awareness/education • Training on means reduction at hospital Engage veteran support groups in education/training Patient, community, and provider education on link of alcohol use and suicide attempt List crisis line on eviction notices- who do we need to connect with? Adapted from: http: //www 2. isu. edu/irh/projects/ysp/Community. Suicide. Prevention/4 Prevention. Planning/Prevention. Planning. pdf

SFR by the numbers 2014 2015 2016 2017 Suicide Count Authorizations Received Cases Reviewed Rollover 67 70 77 78 20 19 15 13* 12 8 16 20 8 19 18 18 *17 additional letters have been sent out and await response ** 2018 Suicide Count YTD = 9

Risk factors

Individual risk factors

Protective factors

Recommended system-level interventions

Recommended system-level interventions Strategic Direction 1: Healthy and Empowered Individuals, Families, and Communities Outreach to hotels/motels to provide QPR and crisis line information on phones and books in hotel rooms School based suicide prevention Outreach to gun shops/retail on mental health, refusing sales and awareness of first time gun buyers Strategic Direction 2: Clinical and Community Preventive Services Training on suicide prevention for various groups: friends, family members & general public, caregivers and skilled nursing facility staff, detectives, parole officers, juvenile system, etc. Training on means reduction Strategic Direction 3: Treatment and Support Services Outreach to clinical care for screening for suicidal ideation and mental health (outreach to specialty care: neurology, women’s health, and post stroke care Consider decreased amount of prescription medications prescribed, opioid addictions work, keeping medications secured Notify crisis team upon discharge for mental health with discharge plan

How are recommendations used? Training: County animal shelter and volunteers Adult foster care providers County and city police officers and Crisis Negotiation Unit County 911 service providers Engagement: LGBTQ organizations Local health care and health plan partners Leadership Support: Lethal means reduction work

Other outcomes Connect DME with local health care system contacts Personal affect boxes Family donation to program Support to next of kin Surviving a Suicide brochure

Clackamas County’s suicide fatality review process is in development: Health, Housing and Human Services Department support Clackamas County Behavioral Health Division support Clackamas County Public Health Division support Clackamas County Deputy Medical Examiner support

Clackamas County Next steps: Develop a Suicide Prevention Council where Council and Suicide Prevention Coordinator identify priorities, research how to influence system and make recommendations.

Get Trained to Help Website Clackamas, Multnomah and Washington counties joined together to create a one-stop gateway where community members can go to learn about and register for free mental health first aid trainings. By combining resources, we offer classes across the region, reaching more people desiring to help others in need.

Get Trained to Help Website Goals of Get Trained to Help : • Increasing Awareness • Normalizing Mental Health Issues • Increasing Knowledge, Skills & Confidence • Sharing Resources • Empowering Families, Communities and Individuals Get Trained to Help Offers Evidence-Based Trainings By Certified Instructors • QPR – Question, Persuade & Refer • Mental Health First Aid • Applied Suicide Intervention Skills Training (ASIST) • Counseling on Access to Lethal Means (CALM) • Honest, Open, Proud (HOP)

Get Trained to Help Website http: //gettrainedtohelp. com/

What have we learned?

Contact information Debra Darmata Suicide Prevention Coordinator Washington County debra_darmata@co. washington. or. us 503— 846 -4748 Adam Knapp Deputy Medical Examiner Washington County Public Health Adam_Knapp@co. washington. or. us Kimberly Repp, Ph. D, MPH RAID Program Supervisor Washington County Public Health Kimberly_Repp@co. washington. or. us 503 -846 -4914 Galli Murray Suicide Prevention Coordinator Clackamas Galli. Mur@co. clackamas. or. us 503 -742 -5373
- Slides: 33