When Good Kidneys Go Bad Chronic Kidney Disease

When Good Kidneys Go Bad Chronic Kidney Disease Kay Mc. Laughlin Renal Service Capital & Coast District Health Board

Causes of chronic kidney disease other than diabetes Screening for renal disease Supporting people with kidney disease

Other Causes of End Stage Kidney Disease Glomerulonephritis 22% Hypertensive vascular disease 9% Polycystic kidney disease 5% Ureteric reflux Tubulointerstitial disease e. g. Drug induced e. g. antibiotics, NSAIDs Obstructive uropathy e. g. prostatism Plasma cell disorders e. g. myeloma, amyloid nephopathy

Kidney Disease in New Zealand as at 31 st Dec 2014 4306 Renal Replacement Therapy 2678 on Dialysis 1628 functioning Kidney Transplants (131 transplants in 2014) 547 new dialysis patients in 2014 53% new pts - Maori or Pacific People ANZDATA Registry 2015


CCDHB Regional Renal Service Lower North Island & Upper South Island Total renal replacement therapy = 481 pts Haemodialysis = 160 20% home haemodialysis 80% supported haemodialysis Peritoneal Dialysis = 83 Functioning kidney transplant = 238 Predialysis (e. GFR <15 ml/min) = 100 – 120 Outpatient clinics (Wellington, Hutt, Kenepuru, Kapiti)

Survival of people on dialysis Percentage survival for people on dialysis, according to age at the start of dialysis Age (years) After one year After two years After five years 0 -24 95 93 75 25 -44 99 94 74 45 -64 90 80 52 65 -74 84 71 34 75 -84 76 54 20 Over 85 61 42 19 Source: Australia and New Zealand Dialysis and Transplant Register: www. anzdata. org. au

End stage kidney failure comprises the visible component of care Endstage Stage 5 CKD Stage 1 CKD
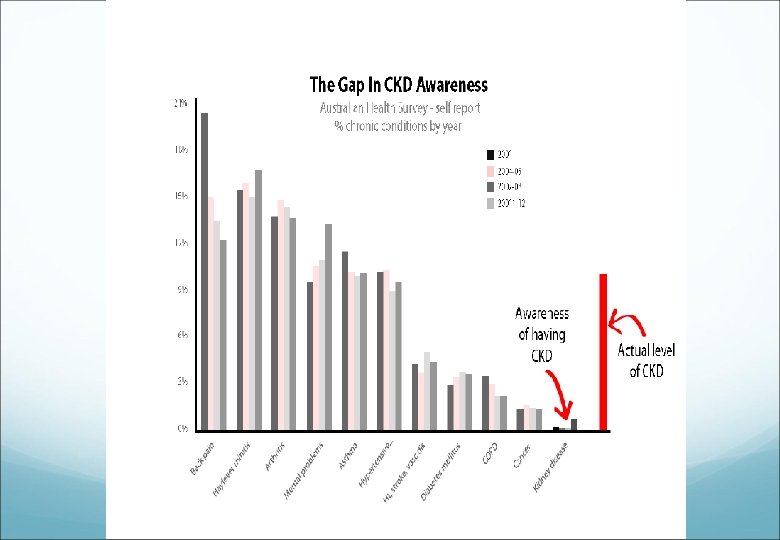

Why Identify CKD Early? Prevalence of ESRD increasing in NZ at 4 - 6% pa Doubling of dialysis numbers every 13 yrs Once symptomatic (GFR ~ 20 m. L/min) then kidney failure inevitable and complications already apparent (CVD, PTH, anaemia) Late referral associated with increased costs, morbidity and reduced survival

Screening – High Risk Groups Annual renal function tests Diabetics / metabolic syndrome Cardiovascular disease Hypertension Family history of renal disease Maori, Pacific Island people Elderly Multisystem disease – SLE, vasculitis, myeloma

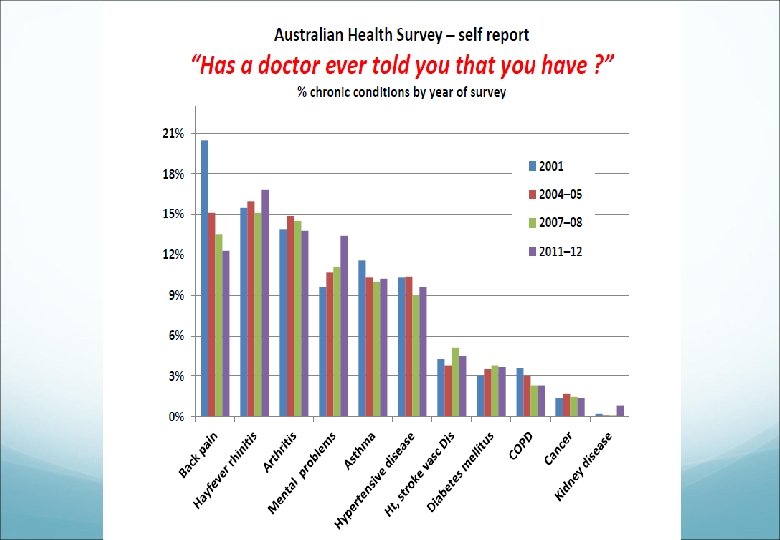
Detection of kidney disease: BP measure for hypertension Blood test – level of kidney function (e. GFR) Urine test for protein (ACR)

Proteinuria assessment

Prognosis of CKD
 People with chronic kidney disease have: • 10 - 20 fold")
Cardiovascular Disease (CVD) People with chronic kidney disease have: • 10 - 20 fold greater risk of cardiac death • Are at least 20 times more likely to die from CVD than survive to the point of needing RRT The kidneys are sometimes described as the ‘canary in the coal mine’ Noble, E. et al (2008), Nephrology Dialysis Transplantation 1 -6

CKD patients who are best managed in primary care Stable stage 3 CKD (e. GFR 30 -60 ml/min) Elderly CKD patients Absent heavy proteinuria (ACR<30 mg/mmol) with no haematuria Focus on BP control and CVD risk Avoidance of nephrotoxins BPJ: The detection and management of patients with chronic kidney disease in primary care, p 37 – 44. Issue 66,

Who do the renal service need to see? Progressive CKD in patients with e. GFR <45 ml/min Evidence of intrinsic kidney disease e. g. glomerulonephritis, polycystic kidney disease or interstitial nephritis (haematuria with heavy proteinuria) Resistant hypertension and/or significant issues with blood glucose control and/or multiple vascular complications BPJ: The detection and management of patients with chronic kidney disease in primary care, Issue 66, p 37 – 44

But. . The majority of patients with CKD 3 -5 are elderly women No evidence of structural issue with kidneys or urinary abnormalities Is this really a disease? Most of these patients will never develop clinically significant renal disease

The Aging Kidney

Ms EM age 74 Decline in renal function Known hypertension but recently well controlled Not diabetic Rx – nifedipine, metoprolol, omeprazole, thyroxine Recent US normal SCr 109 -134 over last 3 yrs (variable) e. GFR 46 → 34 over 3 yrs (CKD Stage 3 b) Urinary ACR 0. 7 mg/mmol (normal <3. 5 mg/mmol)

Ms EM age 74 What’s the likely diagnosis? What is the prognosis? How should this be treated? Is renal review really necessary?

Ms EM age 74 What’s the likely diagnosis? Age and HTN related nephrosclerosis What is the prognosis? Likely very slow deterioration in renal function How should this be treated? BP control & avoidance of nephrotoxins Is renal review really necessary? Probably not

Management – stage 3 CKD Blood Pressure <130/80 mm. Hg <125/75 mm. Hg if proteinuria (>1 g) Use ACEi / ARB first line Blood pressure Likely to need multiple agents 2014 Joint National Committee Guidelines (JNC 8)

‘It is difficult to make the asymptomatic patient feel better’ Stanley O. Hoerr 1962

Management stage 3 CKD Proteinuria: Aim to reduce by >50% ACEi / ARB Lipids – CVD guidelines: Total cholesterol target < 4. 0 LDL < 2. 0 HDL > 1. 0 Triglycerides < 1. 7 Glucose control: Target Hb. A 1 c 50 -55 mmol/mol
 Stop fibrates (Bezafibrate) Reduce drug doses (metformin)")
Management stage 3 Avoid NSAIDs (Naproxen, Ibuprofen) Stop fibrates (Bezafibrate) Reduce drug doses (metformin) Plus ‘specific’ renal CKD treatment

Renal CKD Treatment Anaemia Eligible for EPO if Hb < 100 g/L &: No other cause of anaemia identified e. GFR < 45 m. L/min & diabetic e. GFR < 30 m. L/min & non-diabetic Consider likely benefit of raising Hb Mobility, exercise potential, independence CVS symptoms Hb > 120 g/L of no benefit No evidence of improved long-term survival

EPO Management Eprex injections 1 -2 x weekly Usual starting dose 4000 u 1 x week Fortnightly Hb monitoring for 1 month & then monthly Aim to keep Hb 100 -120 g/L Iron repletion essential Ferritin > 200, TSAT > 20%

General Management of CKD Hyperkalaemia Consider reduction in ACE-I/ARB dose Consider reduction in β-blocker dose Acidosis Sodium bicarbonate – Sodibic tabs Evidence suggests slowing of progressive CKD

Dietary Advice for CKD Potassium restriction only if K+ consistently >5. 5 mmol/L Sodium restriction if hypertensive or volume overload Phosphate restriction if PO 4 > 2. 0 mmol/L Protein restriction only of benefit in late stage CKD
 Diuretics Fibrates &")
Medicines To Be Wary Of NSAIDs (esp. with ACEI & diuretics) Diuretics Fibrates & statins e. g. Bezafibrate & Simvastatin Metformin (reduce in CKD) IV radio contrast containing iodine (angiography)

Summary Identification of patients with e. GFR < 60 m. L/min is now common Useful for identifying patients: At risk of drug toxicity At increased cardiovascular risk At risk of progressive CKD Proteinuria is a major prognostic marker & an important treatment target

Summary Roughly 10% of population, >30% of elderly, will be identified as having CKD Most will remain well and asymptomatic and die of other diseases Appropriate referral guidelines and tailored renal advice essential Most stable elderly patients should be dealt with in primary care

Integrated Care needed to manage CKD

BPAC Guidelines & Decision Support Module

Video resource for patients and families: ‘Treatment Options for End Stage Kidney Disease’ • Kidney Transplant • Peritoneal Dialysis • Haemodialysis • Supportive Care (No dialysis or transplant)
- Slides: 37