Whats the diagnosis Arijit Mitra Consutant Ophthalmogist BMEC

What’s the diagnosis? Arijit Mitra Consutant Ophthalmogist - BMEC

Case 1 27 year female, British Iranian Dentist, medical student Bilateral fixed dilated – 24 hours Difficulty in focussing – BE VA – BE – 6/9 PMH - NAD


Differential diagnosis Pharmacological Posterior synechia Traumatic mydriasis Bilateral Addie’s pupil Bilateral afferent defects – End stage glaucoma, Optic neuropathies Bilateral efferent/structural defects - midbrain strokes/trauma. Beware of bilateral third nerve palsy

Examination Pupils change shape every hour !!! Minimally reactive No difference in light or dark ? Vermiform movement of iris

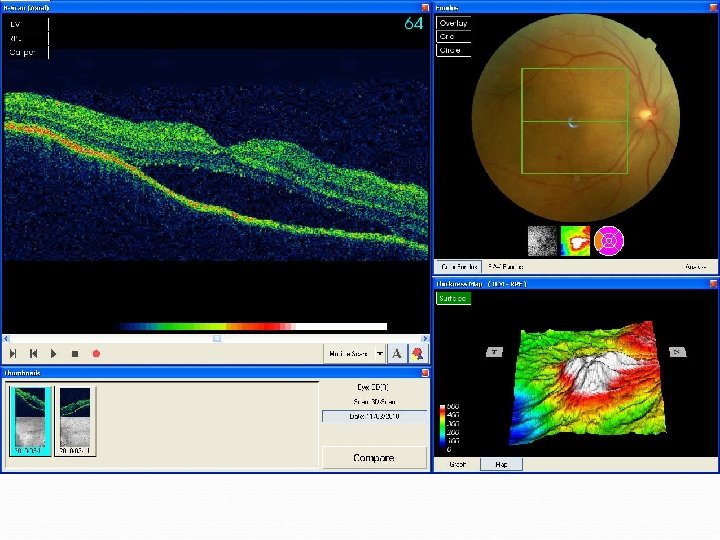
Examination Anterior segments - WNL IOP – WNL Fundus

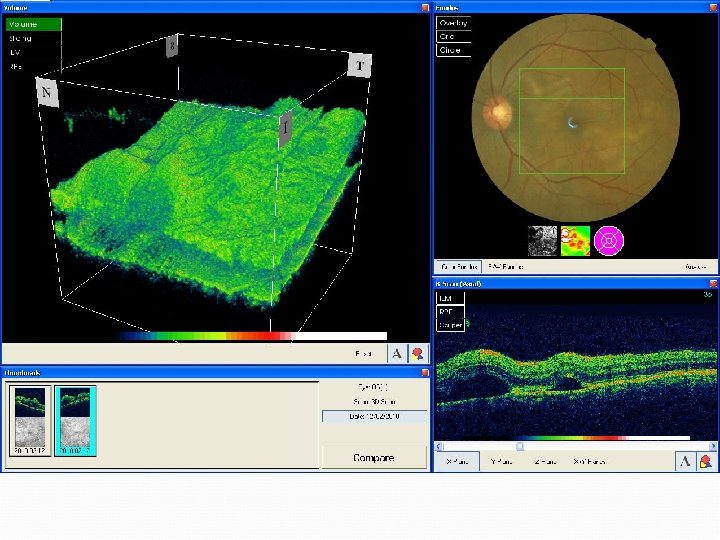
OCT – 21/1/11

Working diagnosis CSCR But why is the pupil dilated? Why is the pupil changing shape every few hours? Referred to neuro-ophthalmology

Tadpole pupil - 1 Segmental spasms of the iris dilator muscle produce intermittent pupillary distortion 26 cases 21 – F, 5 – M Age - 24 to 48 years Thompson HS, Zackon DH, Czarnecki MD. Tadpole-shaped pupils caused by segmental spasm of the iris dilator muscle. Am J Ophthalmol 1983; 96: 467– 477.

Tadpole pupil - 2 Episodes are brief, lasting less than 5 min – 23 patients, less than 2 min – 18 patients, and less than 1 min – 8 patients Can occur several times a day 11 patients had Horner's syndrome, 4 had Adie's tonic pupil, and 11 had definite or probable migraine The episodes eventually stopped, leaving no serious sequelae Aetiology is unclear, although it is postulated that the cause is of benign neural origin

Over the next few days. . . VA – 6/60 – BE Refd to Moorfields Eye Hospital – confirmed Tadpole pupil Fundus – more extensive central serous / exudative RD Admitted

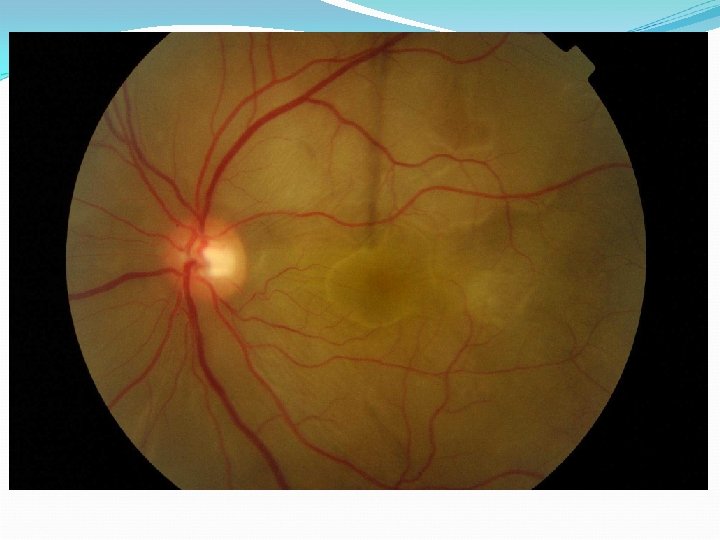
Case 2 30 year male, British Pakistani Loss of vision – LE x 1/52 VE – RE – 6/6, LE – 6/24 PMH – NAD Anterior segment and IOP - WNL

Case 2

Case 3 32 year female, British Pakistani Loss of vision – BE x 1/52 VE – RE – 6/12, LE – 6/12 PMH – NAD Anterior segment and IOP - WNL

Case 3 Pharmacist Grandma on Prednisolone Self medicated with oral Prednisolone 40 mg x 2/7 Felt her vision was improving

Case 3

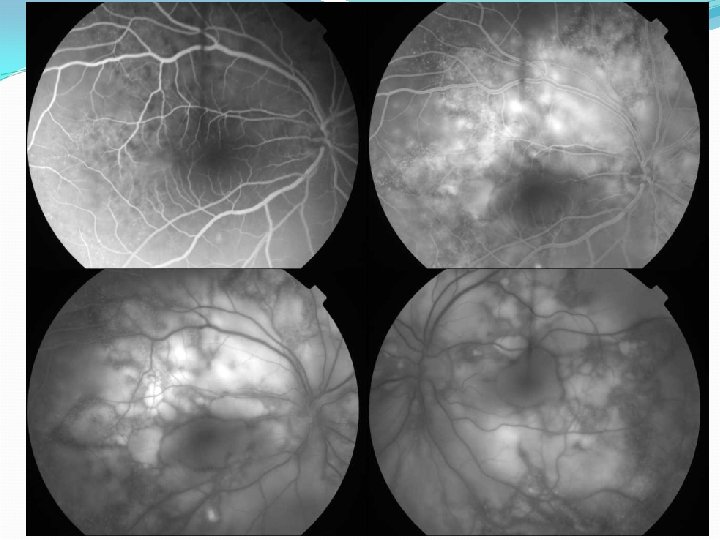
Case 4 – Day 1 29 year male, Bangladeshi Bilateral loss of vision – 3/52 VA – RE – 6/24, LE – 6/18 PMH - NAD

Examination AC – 1+ cells IOPS – WNL Vitreous – 1+ cells

Case 4

Case 4 Bloods – FBC, ESR, CRP, U&E, LFT, Glucose, Hb. A 1 c, Autoantibodies (ACE, ANCA, Anti ds-DNA), RF, Syphilis and Toxoplasma antibodies Chest Xray Mantoux test OCT, FFA +/- ICG

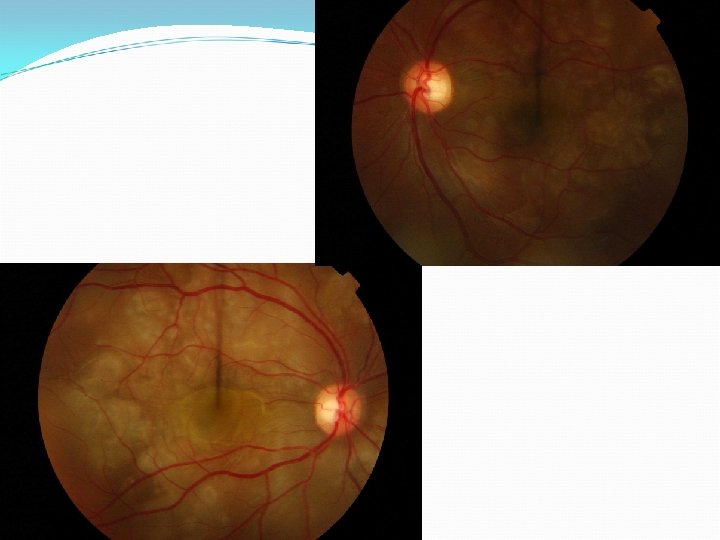
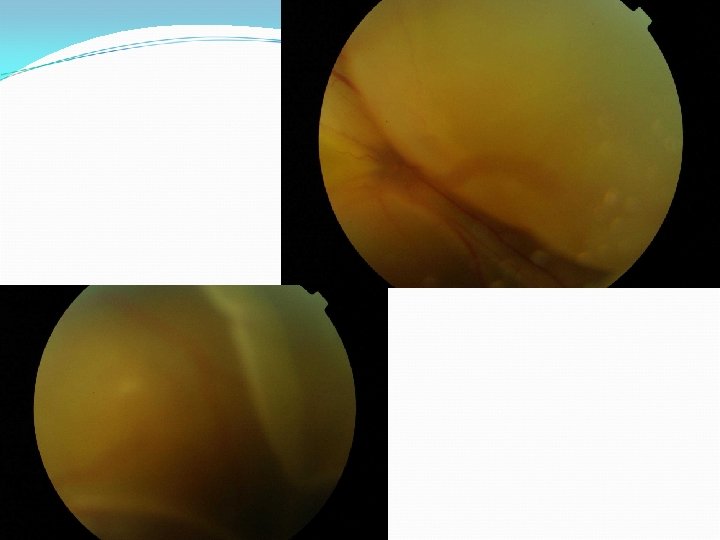
Case 4 – Day 3 Deaf VA – BE – 6/60 Anterior segments and IOP – unchanged Fundus examination

Case 4

Investigations - Case - 1 Full uveitis screen MRI Lumbar puncture CSF – 100 % lymphocytic pleocytosis (with melanin laden cells)

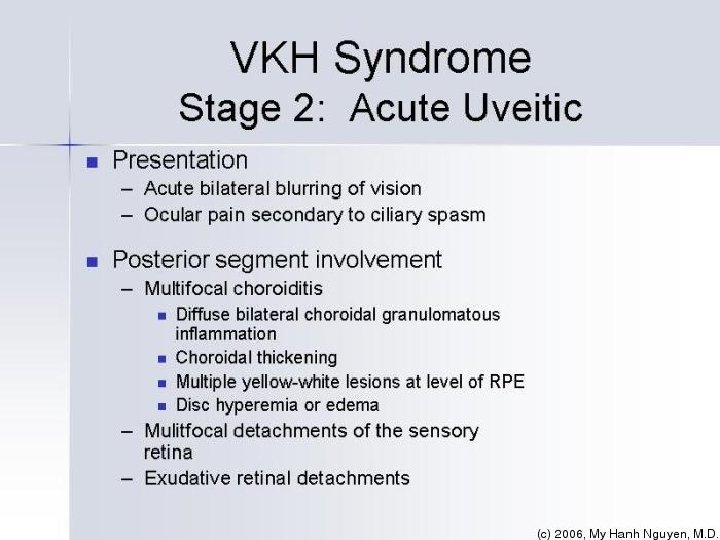
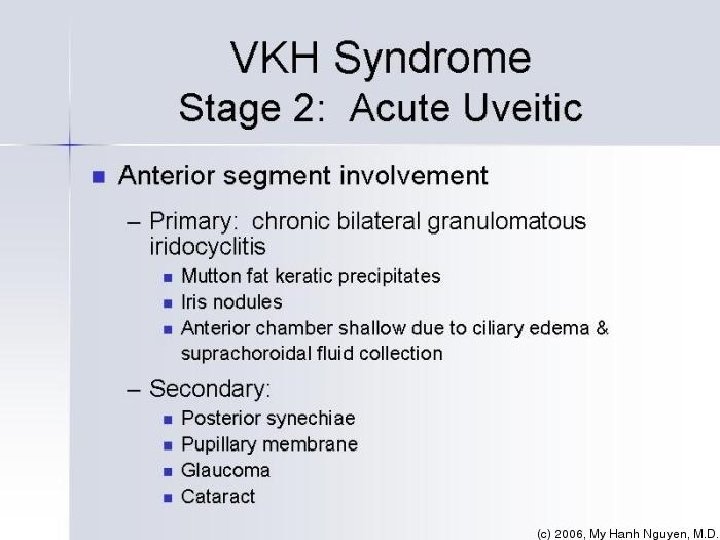
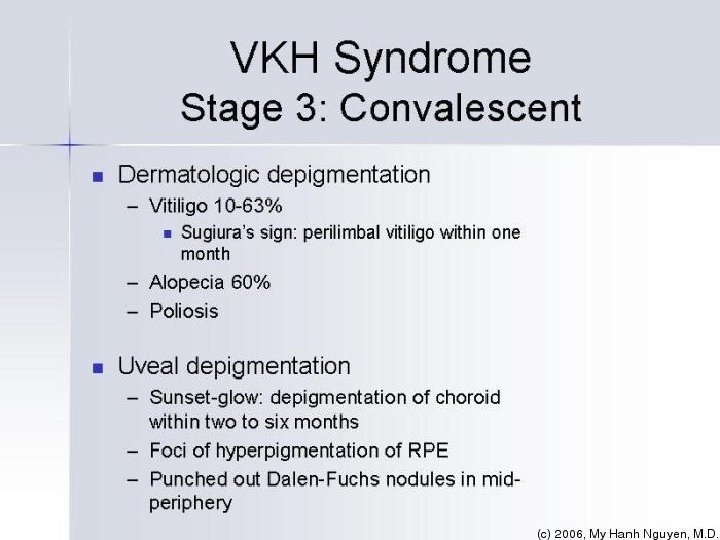
Vogt-Koyanagi-Harada Syndrome

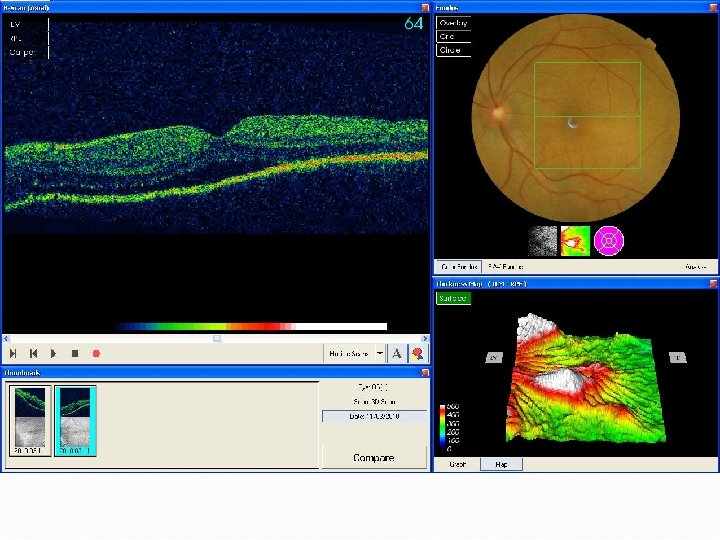
Treatment – Case 1 IV Methylprednisolone – 1 gm /day x 3/7 Oral Prednisolone VA started improving 5 days later – VA – 6/9 - BE

OCT – 21/1/11

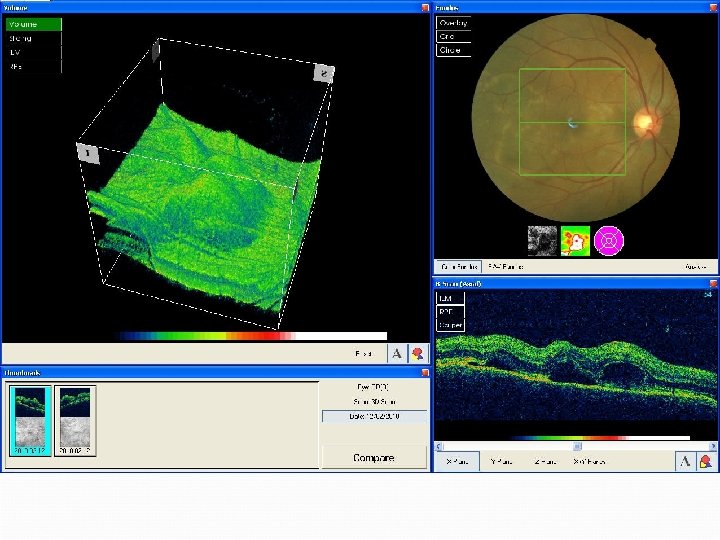
OCT – 26/1/11

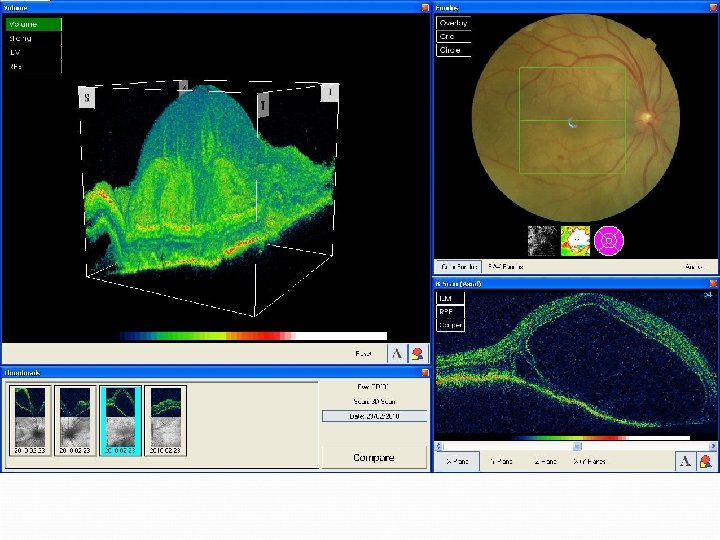
Case 4 – Pre-treatment

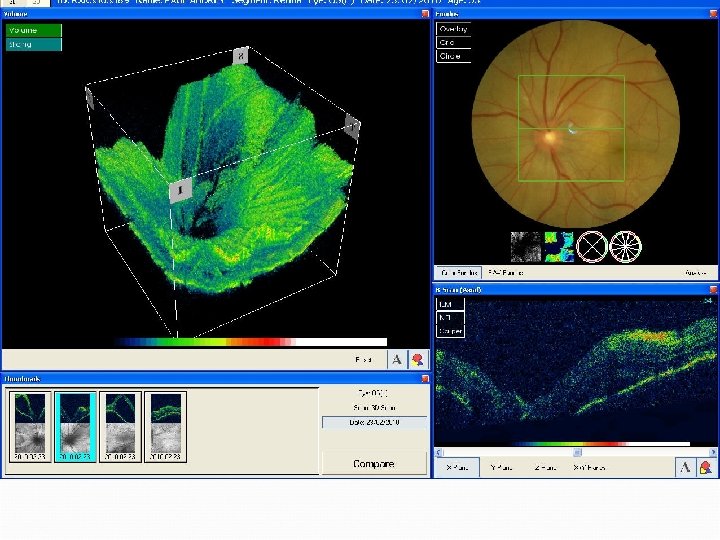
Case 4 – Post-treatment

Leopard - spots

MB - 1

Case 5 53 yo A-C medical secretary Worsening vision and eye pain over 1 -2/7 Associated lethargy/tiredness Preceding headache, neck pain and photophobia RVA 6/12 (6/9) LVA 6/9(6/6)

MB – 2
")
Case 6 26 yo Bangladeshi, 12/40 preg 2/7 blurring vision RVA 6/18 LVA 3/60(6/12) No pain, headache, photophobia No AC or Vit inflammation Brother had TB 10 yrs ago

Treatment TB ‘excluded’ IV Methylprednisolone 500 mg alt days x 3 Oral steroids delayed because of potential risk to foetus 3 weeks post presentation – VA PL OU Total RDs
 and slowly increased")
Cyclosporin added (relative saftey in Pregnancy) and slowly increased

Outcome Healthy baby Continued to need immunosuppression RVA 1/60 LVA 2/60

VKH
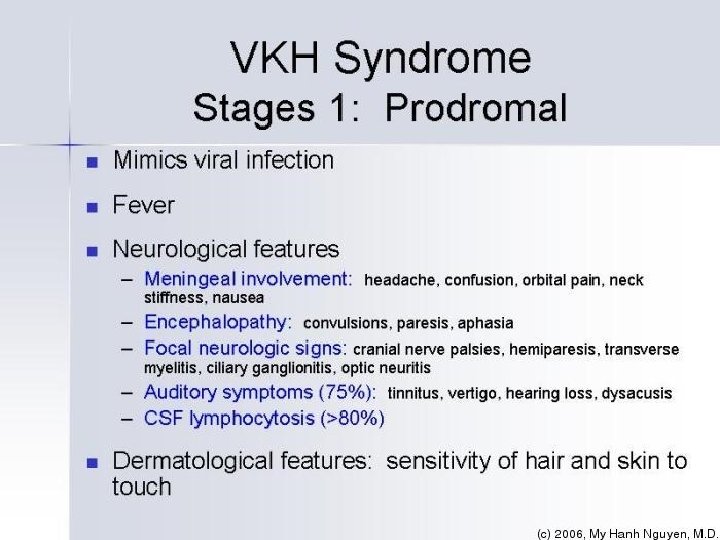
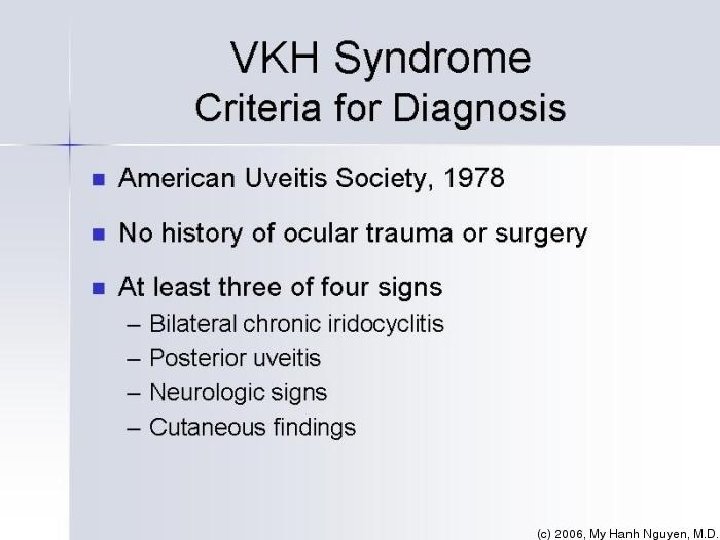

International Committee of Experts during The First International Workshop on VKH Disease in 1999 Complete Posterior uveitis Neurologic and auditory manifestations Integumentary manifestations (but not before others) Incomplete Probable

International Committee of Experts during The First International Workshop on VKH Disease in 1999 I. No history of ocular trauma or surgery. II. No clinical or laboratory evidence of other inflammatory causes. III. Bilateral ocular involvement: a. Early manifestations i. Diffuse choroiditis (with or without anterior uveitis, vitritis, disc hyperemia) ii. With equivocal fundus finding. Both of the following two must be present: fluorescein angiogram findings: delay in choroidal perfusion, multifocal pinpoint leakage, large placoid hyperfluorescence within subretinal fluid, or optic disc staining; and ultrasound findings: diffuse choroidal thickening without posterior scleritis. b. Late manifestations i. Previous history suggestive of early ocular manifestation of VKH, and either both (ii) and (iii) below, or multiple signs from (iii) ii. Ocular depigmentation (sunset fundus or limbal depigmentation known also as sugiura sign) iii. Other ocular signs: nummular retinal depigmentation, retinal pigment epithelial pigment clumping, or recurrent or chronic anterior uveitis. IV. Central nervous system or auditory complaints: meningismus, tinnitus, or CSF pleocytosis. V. Integumentary findings (not preceding the CNS or ocular manifestations): alopecia, poliosis, or vitiligo. A diagnosis of complete VKH requires the presence of all 5 criteria. Incomplete VKH is made when only criteria I-III are present together with either IV or V. When only the first 3 criteria are present, the diagnosis is probable VKH.


Pathophysiology Uncertain Multisystem nature suggests infectious or autoimmune central cause Cell-mediated autoimmune disease directed against melanocytes. Immunogenetic predisposition? HLA-DR 4, HLA-DR 53, HLA-DQ 4, HLA-DQ 7, HLA-DR 1

Treatment Early aggressive treatment Corticosteroids Oral prednisolone Iv methylprednisolone Immunosuppresive agents Cyclosporin. A Cytotoxic agents Azathioprine Immunoglobulin therapy
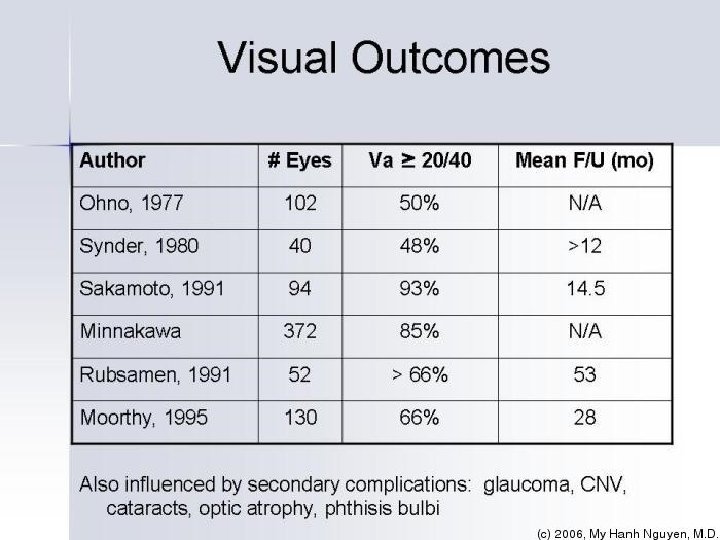

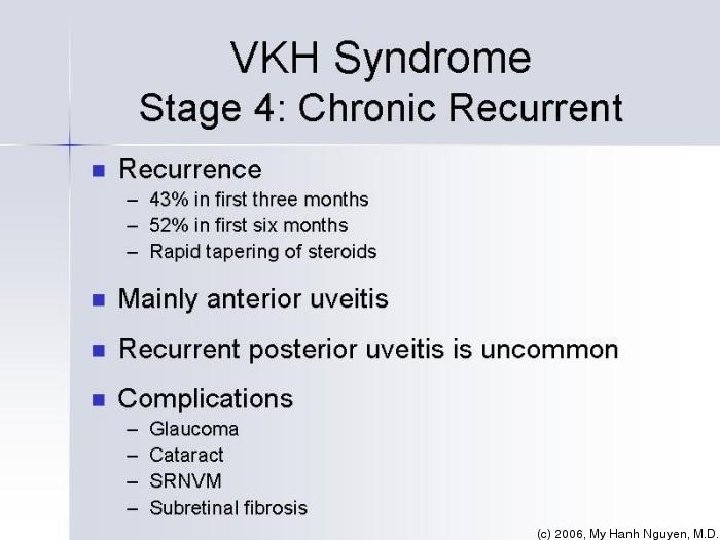
VKH Summary Multisystem disorder Bilateral Uveitis Exudative detachments, effusions Anterior Neurological/auditory manifestations Integumentary findings (not preceding the onset of CNS or ocular disease) - Alopecia, or Poliosis, or Vitiligo Treat early and aggressively Rule out other causes first Chronic disease requiring long term treatment Visual outcomes can be good

Take home message Multifocal bilateral CSR like appearance in an Asian patient with or without skin changes / neurological features – Think of VKH Contact the Uveitis team / VR fellow Admit these patients for full work up

Thank you
- Slides: 65