What is ADHD Updates in ADHD for School












 – First line: Evidence-based")
 – Evidence stronger")
 – ADHD medication •")




 • Starting at a")
 •")






 • • Selective norepinephrine reuptake inhibitor Not a controlled substance Oral capsule")

 – Initial dose 0. 1 mg at bedtime,")






- Slides: 37
What is ADHD? Updates in ADHD for School Nurses: Diagnostic and Medical Considerations Lindsay Wargelin, APN Pediatric Nurse Practitioner Developmental Pediatrics James Weedon, MD Developmental and Behavioral Pediatrician Division Director for Developmental Pediatrics School Nurses’ Conference April 9, 2019
Objectives • Review the clinical features and presentation of Attention Deficit Hyperactivity Disorder and evaluation process • Understand diagnosis and treatment recommendations based on age group • Discuss the use and management of medication in treating ADHD
What is ADHD? • DSM-V criteria – Symptoms of inattention or hyperactivity/impulsivity have persisted for at least six months and there is functional impairment in two or more settings. – NEED input from teachers, other adults besides parents. • ADHD Subtypes – Hyperactive, Inattentive, Mixed
Prevalence of Subtypes
DSM-5 Criteria Inattentive Symptoms • Inattention: Six or more symptoms of inattention for children up to age 16, or five or more for adolescents 17 and older and adults; symptoms of inattention have been present for at least 6 months, and they are inappropriate for developmental level: – Often fails to give close attention to details or makes careless mistakes in schoolwork, at work, or with other activities. – Often has trouble holding attention on tasks or play activities. – Often does not seem to listen when spoken to directly. – Often does not follow through on instructions and fails to finish schoolwork, chores, or duties in the workplace (e. g. , loses focus, side-tracked). – Often has trouble organizing tasks and activities. – Often avoids, dislikes, or is reluctant to do tasks that require mental effort over a long period of time (such as schoolwork or homework). – Often loses things necessary for tasks and activities (e. g. school materials, pencils, books, tools, wallets, keys, paperwork, eyeglasses, mobile telephones). – Is often easily distracted – Is often forgetful in daily activities.
DSM-5 Criteria Hyperactive Symptoms • Hyperactivity and Impulsivity: Six or more symptoms of hyperactivityimpulsivity for children up to age 16, or five or more for adolescents 17 and older and adults; symptoms of hyperactivity-impulsivity have been present for at least 6 months to an extent that is disruptive and inappropriate for the person’s developmental level: – Often fidgets with or taps hands or feet, or squirms in seat. – Often leaves seat in situations when remaining seated is expected. – Often runs about or climbs in situations where it is not appropriate (adolescents or adults may be limited to feeling restless). – Often unable to play or take part in leisure activities quietly. – Is often "on the go" acting as if "driven by a motor". – Often talks excessively. – Often blurts out an answer before a question has been completed. – Often has trouble waiting his/her turn. – Often interrupts or intrudes on others (e. g. , butts into conversations or games)
Why is ADHD a Problem? • Prevalence of 8 -10% of all school-age children – 5. 2 Million Children, 2 ½ : 1 -- Male : Female • High incidence of co-morbid disorders – Learning Disability, ODD, CD, Anxiety, Depression • Left untreated – – School failure Difficulty with peer relationships Risk taking behaviors Difficult to achieve success
AAP Clinical Guidelines • Published November 2011 in Pediatrics • Result of a 2 year task force including members of: • • American Academy of Pediatrics American Academy of Child and Adolescent Psychiatry Child Neurology Society for Pediatric Psychology National Association of School Psychologists Society for Developmental and Behavioral Pediatrics American Academy of Family Physicians Children and Adults With Attention-Deficit/Hyperactivity Disorder (CHADD) • Epidemiologist from the Centers for Disease Control and Prevention (CDC).
Key Action Statements • Primary care clinician should initiate an evaluation for ADHD for any child 4 through 18 years of age who presents with academic or behavioral problems and symptoms of inattention, hyperactivity, or impulsivity. • Previously 6 through 12 years of age. • ADHD is difficult to diagnose accurately in the earlier years of life.
Key Action Statements • Include assessment for other co-morbidities • Emotional or behavioral • Anxiety, depressive, oppositional defiant, and conduct disorders • Developmental • Learning and language disorders or other Neurodevelopmental disorders • Other • tics, sleep apnea
Diagnostic Considerations • Anxiety or depression can present as hyperactivity or inattention in children • Children with developmental delay should be assessed according to their developmental expectations • Children with ADHD-combined or primarily hyperactive are identified earlier than with inattentive subtype and boys tend to be more hyperactive than girls. • Most common presenting symptom in preschool is hyperactivity and impulsive control
Treatment of ADHD • Three-pronged approach 1. Behavioral modification 2. Educational support 3. Use of medication to supplement
Evidence for Treatment by Age • Age 4 -5 (Preschool-aged) – First line: Evidence-based parent and/or teacheradministered behavior therapy • Quality of evidence A / Strong recommendation – If behavioral interventions do not provide significant improvement and symptoms are moderate-severe, trial of stimulant medication with weighing harm of early medication with delay of diagnosis and treatment • Quality of evidence B / Strong recommendation
Evidence for Treatment by Age • Age 6 -11 (Elementary school-aged) – Evidence stronger for ADHD medication • Quality of evidence A / Strong recommendation – And/or Parent/teacher behavior therapy • Quality of evidence B / Strong recommendation – Preferably both with educational supports
Evidence for Treatment by Age • Ages 12 -18 (Adolescents) – ADHD medication • Quality of evidence A / Strong recommendation – Behavior therapy • Quality of evidence C / Recommendation – Preferably both with educational supports
Educational Accommodations and Supports
Educational Supports • Classroom environment – Special education vs. mainstream classroom – Accommodations – Educational strategies • Individualized Education Program – IEP • 504 plan
Examples of School Accommodations • Physical – Seating – Organization of materials – Removal of distractions including during testing • Instructional accommodations – Repeat and simplify directions – Check in for understanding – Provide examples and written instructions • Behavioral accommodations – Positive reinforcement – Special jobs or leadership duties – Open communication with parents
ADHD Medication
Medication Considerations • Finding the right medication (stimulants vs non-stimulants) • Starting at a low dose and increase slowly • Monitor for side effects versus benefit • Use Vanderbilt questionnaire as a baseline to monitor response to treatment
ADHD Medications • Stimulants 1. Methylphenidates 2. Amphetamines • Nonstimulants – Atomoxetine (Strattera) • Alpha-2 -adrenergic agonists • Antidepressants – Tricyclics and dopamine reuptake inhibitors
Stimulant Pharmacokinetics • Weight dependent dosing in children is not well established. In general, start at a low dose and increase slowly. • Onset of action 45 min to 1 hour • Duration – Immediate release 3 -5 hours – Extended release 8 -12 hours • Be wary of peaks and valleys
Stimulant Medications
Methylphenidates
Amphetamines
Side Effects of Stimulants • Appetite suppression • Sleep disturbance • Weight loss • Transient symptoms: – Headache, stomachache • Stop taking immediately if: – Acute marked changes in behavior or mood – Symptoms of hallucination, psychosis, or mania
Other Concerns • Stimulants as gateway to drug abuse? – NO! Untreated ADHD has increased risk of substance abuse. Treated ADHD risk of substance abuse is near population levels.
Atomoxetine (Strattera) • • Selective norepinephrine reuptake inhibitor Not a controlled substance Oral capsule – do not open and sprinkle Starting dose of 0. 5 mg/kg/day, titrate to 1. 2 mg/kg/day. Max of 1. 4 mg/kg/day • Daily dosing or BID • Must be given every day
Side Effects of Strattera • • • Less common Abdominal pain, nausea, vomiting Decreased appetite Headache Somnolence
Alpha-2 -Adrenergic Agonists • Clonidine (Catapres) – Initial dose 0. 1 mg at bedtime, titrate by 0. 1 mg weekly, maximum 0. 4 mg/day, up to QID – Extended-release: Kapvay • Guanfacine (Tenex) – Initial dose 0. 5 -1 mg/day at bedtime, titrate by 0. 51 mg weekly, maximum 4 mg/day, up to QID dosing – Extended-release: Intuniv
Alpha-2 -Adrenergic Agonists • Can be used as monotherapy or adjunct to stimulant medication • Requires 1 -2 weeks for initial response • Must taper off slowly to prevent rebound hypertension
Side Effects • • Sedation Bradycardia Headache Hypotension • May be useful in children who are overaroused, highly active, and aggressive • Improvement in tics
MTA Study – 14 month f/u
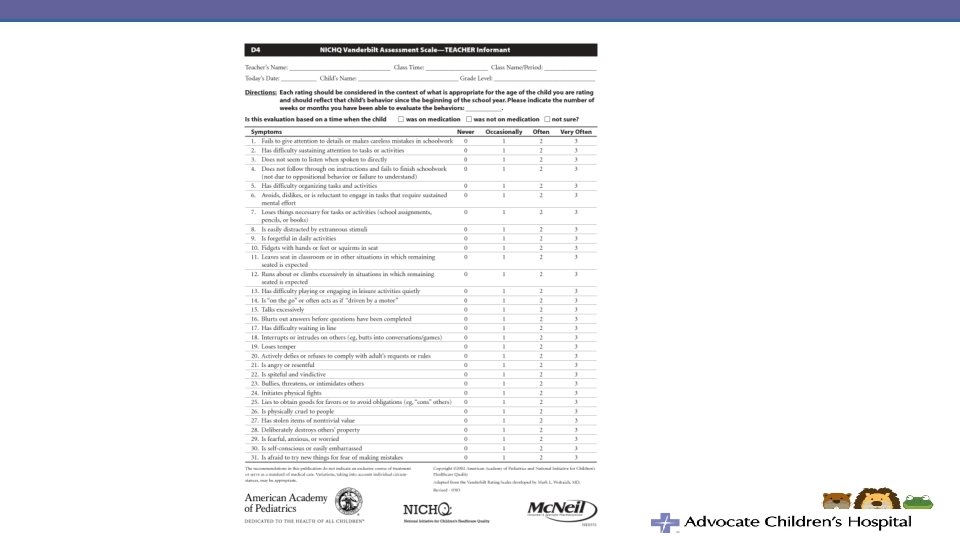
How to Track Efficacy – Vanderbilt Rating Scales • Parent and teacher – School reports – Academic progress – Behavior reports
Additional treatment strategies • • Social skills groups Occupational therapy ADHD coach Parent support groups
Resources • Taking Charge of ADHD by Russell Barkley, Ph. D • SOS Help for Parents by Lynn Clark, Ph. D • Smart But Scattered by Dawson and Guare • Siblings Without Rivalry by Faber and Mazlish • CHADD – chadd. org • Family Resource Center on Disability • www. parentsmedguide. org