What Every Chiropractor Needs to Know about Scoliosis

What Every Chiropractor Needs to Know about Scoliosis

About the CLEAR Scoliosis Non Profit • C. L. E. A. R. stands for Chiropractic Leadership, Educational Advancement, and Research • Founded in 2000 • First scoliosis seminar in St. Cloud in 2002 • Began teaching CE seminars at Parker in 2003 • First research article published in 2004 • Founded the first and only Scoliosis Research Clinic on a chiropractic college campus in 2007 • Achieved Non Profit status in 2008 • CLEAR is the ONLY non profit organization associated with chiropractic scoliosis treatment and research

About the CLEAR Scoliosis Non Profit • The mission of CLEAR is to advance the chiropractic treatment of scoliosis through research and spinal rehabilitation • Step One: create a treatment protocol that is consistently effective in getting results • Step Two: educate chiropractors about scoliosis and get more DC’s involved in scoliosis • Step Three: publish high quality scientific research articles to document the effect of scoliosis specific chiropractic treatment protocols

CLEAR Certification • The CLEAR Institute provides education and certification to DC’s interested in working with scoliosis patients • Chiropractors with a heart for scoliosis can undergo training and testing to become CLEAR Certified • Currently there are over 45 CLEAR Certified Doctors around the world, including locations in Singapore, Tokyo, Indonesia, and Panama • CLEAR receives thousands of calls & e mails every year from people searching for a scoliosis DC

Why get involved with scoliosis? • Most common spinal deformity, found in 5% of adolescents, 10 20% of adults, and 66% of geriatrics • 3 million visits to DC’s by scoliosis patients each year • Suspected cause: sensory integration disorder between the brain and the postural muscles • No recognized treatment options for mild cases • Bracing is not always successful; seeks to stabilize rather than reverse; and can be accompanied by psychosocial sequlae leading to poor compliance • Spinal fusion surgery is expensive and introduces long term complications that are still poorly understood • No options besides “live with it” if bracing/surgery are refused or unsuccessful

What is scoliosis? • • NOT a “sideways curvature of the spine” Rotation is the primary component; think helix, not curve The majority of cases are idiopathic Scoliosis can be caused (or exacerbated) by trauma (MVC, slips/falls, etc), although there is no research on this Older patients may develop de novo (degenerative) scoliosis Other causes include congenital defects such as hemivertebrae or pathology (CP, CT disorders, etc. ) – so called “neuromuscular” scoliosis Infantile and juvenile scoliosis are distinct and separate disease entities that likely have different pathogeneses, but similar manifestations & effects Within the category of idiopathic, there may also be different and distinct diseases with different causes and risk factors for progression

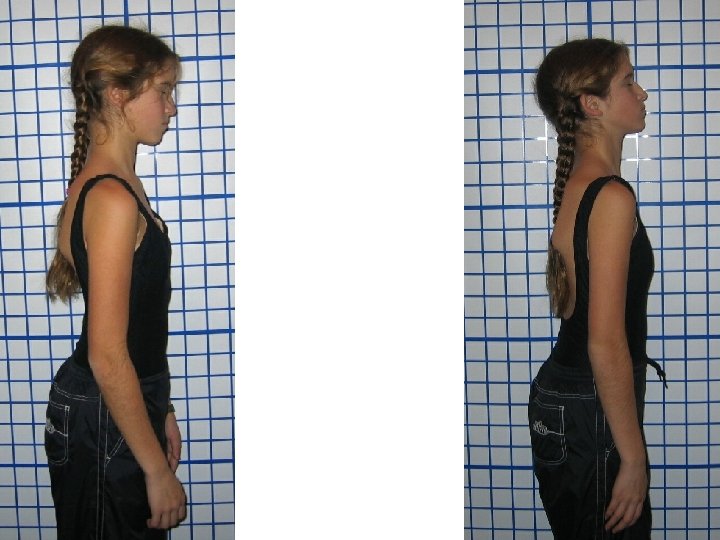
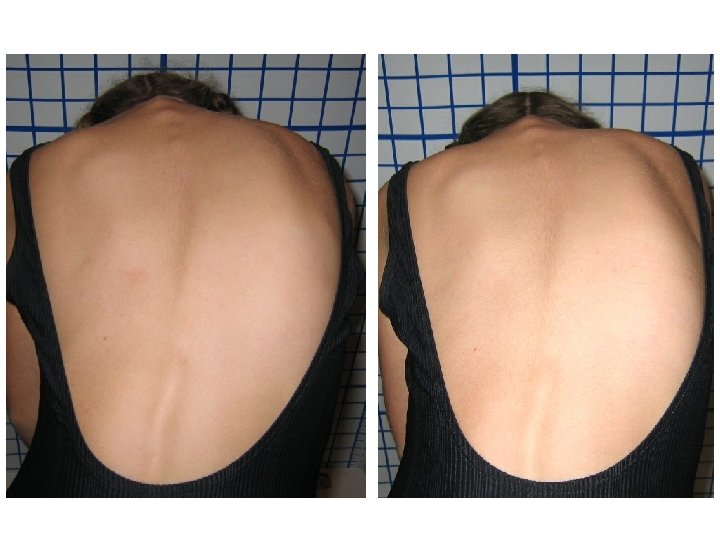
How is it diagnosed? • Postural abnormalities are typically the first sign (imbalances in the shoulders, hips, or ribs) • Scoliosis can ONLY be diagnosed on x ray (but can be reliably measured on MRI’s as well) • Levoscoliosis = left (10%), dextroscoliosis = right (90%) • On x ray, Cobb angle (lateral tilt of 2 vertebrae) of greater than 10◦ and vertebral rotation (Lovett positive) • On exam, noticeable rib arch (NOT “hump”) on Adam’s Forward Bending Test • Proprioceptive imbalances can be detected before the physical or radiographic signs

How is it mis-diagnosed? • Lateral curvature of the spine with no vertebral rotation at the apex is probably postural shift; antalgic posture, repetitive strain/microtrauma, or possible pathology • Physical exam not followed up by radiography • Improper patient positioning during radiography • Inaccurate measurements made on x ray • Functional (or postural) scoliosis mistaken for a structural scoliosis • Functional curvatures disappear on lateral bending; structural curves do not

I suspect this patient has scoliosis. What do I do? • • First, confirm physical exam with scoliometer and record the measurements Second, radiographic exam is MANDATORY Be sure to measure Cobb angle correctly, and ALSO apical vertebral rotation (AVR) If the x ray indicates scoliosis, and this is the patient’s first radiographic exam, also take lateral bending films and measure Cobb angle and AVR on them, also Once scoliosis is confirmed, rule out all other possible causes (congenital defects and pathology) before assigning a diagnosis of idiopathic or proceeding with treatment – 50% of cases of left thoracic scoliosis have underlying pathology; get an MRI! Last, perform a risk assessment to estimate the chance of future progression and disease severity Romberg’s, m-CTSIB, or timed unipedal stance test with eyes closed can be helpful in detecting proprioceptive problems

Scoliosis in adults • If you suspect scoliosis in an adult patient, first review their medical history to determine if they were previously diagnosed with scoliosis in adolescence (Adult Idiopathic Scoliosis) • If listhesis (lateral slippage) of the apical vertebra is present, and there is no prior diagnosis of scoliosis in adolescence, it is most likely degenerative (de novo) scoliosis • These patients are over 40 and tend to have loss of the lumbar lordosis and degenerative disc disease • Scoliosis often worsens during menopause

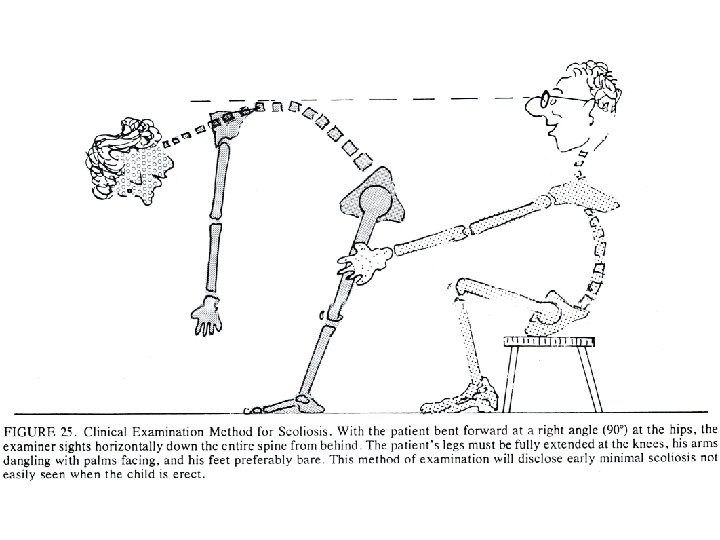
Adam’s Forward Bending Test • Patient barefoot with back fully exposed • Physician seated behind patient • Patient bends forward at the waist 90 degrees, letting the head fall forward and arms dangle, palms together, as the doctor stabilizes the legs • Doctor observes twice in the plane of the spine, looking for arch on one side at partial flexion and on the other side at full flexion
 Diagram of young female with scoliosis")
http: //www. hopkinsmedicine. org/orthopedicsurgery/peds/scoliosis. html ADAMS TEST A) Diagram of young female with scoliosis (note lateral curve of spine) B) Rib arch can be seen on right side when bending over slightly. C) Rib arch present on left side of patient when bending over to greater extent. D) Kyphosis noted when patient bending over and seen from side.

Normal Abnormal

Palms Together Normal Abnormal

Normal Abnormal

Adam’s Forward Bending Test • Adam’s Test results in a high rate of false negatives and inappropriate referrals • Adam’s Test measures rib arching, which usually manifests after the vertebral rotation reaches severe levels (which may not happen until the Cobb angle has progressed to 25 degrees or higher) • “Adam’s Forward Bending Test cannot be considered a safe diagnostic criterion for the early detection of scoliosis (especially when it is used as the only screening tool) because it results in an unacceptable number of false-negative findings. ” (Spine 1999)

Scoliometer Using a Scoliometer drastically increases the effectiveness of scoliosis screening. 7 degrees on the Scoliometer ≈ 20 degree Cobb angle Inexpensive, accurate, reliable, and valid

Using a Scoliometer • Back should be exposed • Starting at the vertebral prominens, run the Scoliometer slowly down the spine, exerting no pressure on the patient • Record the highest value that corresponds to the bead, and also the laterality • Scoliosis can reasonably be suspected at 4 degrees or more

Using a Scoliometer • If using the scoliometer as a monitoring or outcome assessment tool (not for screening), record distinct vertebral levels corresponding to the apices and transitional areas of the curve(s) • Always be sure to use the same vertebral levels for subsequent measurements • Record the measurements both in Adam’s position and prone; this helps to differentiate structural vs. functional cases • Scoliometers have very good intra and inter examiner reliability (Bonagamba et al 2010)

Radiographic Examination • Print out a copy of the ACR-SPR Practice Guideline for the Performance of Radiography for Scoliosis in Children • Make sure the technician taking the x ray follows these guidelines! • Take x rays P A rather than A P to minimize exposure to thyroid and breast tissue • Ensure full visualization from the angles of the mandible to the greater trochanters • If this is the patient’s first radiographic exam, lateral bending films should also be taken; these DO NOT need to be repeated

Radiographic Examination • Don’t attempt to measure bad x rays; re take! • If this is the first time that the scoliosis is being measured, establish the most tilted superior and inferior terminal vertebrae, and then the apical vertebra of each curve (terminal vertebrae may overlap in double or triple curves) • Every subsequent x ray should use these same vertebral levels for future measurements • Don’t miss any curves! You should always be measuring at least two curves. Even a “single” C shaped curve has compensatory curves above and below it

One 45 degree curve? One primary curve and 2 compensatory curves!

Establishing the terminal vertebrae • Place a straight edge along the superior endplate of the vertebra at the top of the curve • Move down to the superior endplate of the next segment • Once you reach a level where the straight edge begins to tilt in the opposite direction, you can establish the previous vertebra as the superior terminal vertebrae • Repeat with the inferior endplate of vertebrae, starting at the bottom of the curve and moving superiorly, to establish the inferior terminus • Be careful with endplates when curves overlap

Terminal Vertebrae T 5 T 12 T 11 L 4

Establishing the apical vertebrae • The apical vertebra is classically defined as the vertebra which is most laterally deviated from midline, and is fairly easy to determine • There may be instances where two vertebrae appear to be roughly the same distance from midline, however; in these instances, establish one vertebra as the “best fit” and use this vertebra in all future measurements to maintain consistency • It tends to be the vertebra with the most “wedged” appearance

Apical Vertebrae T 5 T 12, Apex T 8 T 11 L 4, Apex L 2
 • Although not always measured in orthopedic practice, rotation")
Measuring apical vertebral rotation (AVR) • Although not always measured in orthopedic practice, rotation of the vertebrae classifies the primary component of scoliosis • To measure AVR, draw a line through the pedicle shadow on the convexity • Measure the distance from the convex edge of the vertebra to this line • Measure the total width of the vertebra • Divide the distance by the total width and multiply the result by 100, expressing the result as a percentage

( ( Distance from convex pedicle shadow to convex edge Vertebral body width 9 millimeters 36 millimeters ) ) x 100 = AVR x 100 = 25%
 • There are other methods of measuring AVR; however,")
Measuring apical vertebral rotation (AVR) • There are other methods of measuring AVR; however, this method (Nash Moe) is simple, straightforward, and of sufficient reliability/validity for everyday clinical use • Measuring AVR in addition to Cobb angle emphasizes the three dimensional nature of scoliosis, and provides an additional metric to measure progression and/or the effectiveness of treatment • If Cobb angle is unchanged or improved, but AVR is worse, the scoliosis is not getting better 3 dimensionally (common with old style braces)

Measuring Cobb angle • Once lines have been drawn on the superior endplate of the superior terminal vertebra and on the inferior endplate of the inferior terminal vertebra, perpendicular lines are drawn from these • The angle between the intersection of these perpendicular lines is measured with a protractor, and the result expressed in degrees • It’s best to draw these lines away from the spine to avoid obscuring any vertebral landmarks

Cobb Angle 57 45

Common pitfalls in Cobb angle measurement • Once the terminal vertebrae have been established, always use these same vertebral levels to measure Cobb angle on all subsequent radiographs • Make sure the correct endplates are used (superior endplate for the superior vertebra, and inferior for the inferior vertebra) • If the rotation is severe enough to create an oval shaped appearance to the vertebral endplate, mark the edges and bisect the endplate:

Inherent problems with Cobb angle • Cobb angle is a two dimensional measurement of a three dimensional condition • At its heart, it is only measuring the lateral tilt of two vertebrae • It has a poor correlation with quality of life, pain levels, lung function, cosmetic appearance, and other parameters • It has an inherent measurement error of 4 to 8 degrees, which increases in larger curves • It is not linear; due to the effect of the rotation, a 60 degree Cobb angle is more than twice as severe as a 30 degree Cobb angle
 Lateral view of a coat hanger, showing a Cobb angle of 60 degrees")
(A) Lateral view of a coat hanger, showing a Cobb angle of 60 degrees (B) The coat hanger has been rotated 45 degrees and now the Cobb angle registers only 30 degrees because the coat hanger is not being seen en face as it is in (A) (C) When the coat hanger is turned a further 45 degrees there is no angle at all “Bigger curves are progressively rotated further away from the plane of the patient and thus, for example, a curve of 60 degrees is much more than twice as big as a curve of 30 degrees because the 60 degree curve is seen less en face. ” Idiopathic Scoliosis: The Harms Study Group Treatment Guide, page 20

Determining the risk of progression • Cobb angle must be taken in context with the patient presentation in order to provide meaningful information to the patient and physician • A large Cobb angle in a younger patient is a greater cause for concern than the same Cobb angle in an older individual • Large Cobb angles involving less vertebrae (Harrington Factor) are more likely to worsen • Severe AVR, postural translation, or proprioceptive problems are also indicative of a poorer prognosis and higher risk of progression

Risser sign • Risser sign is the most commonly used method of evaluating skeletal maturity in scoliosis management • The Tanner Whitehouse method, however, is more accurate and involves significantly less radiation exposure • Growth continues up to 2 years after skeletal maturity; adolescents can grow as much as 2 cm – curves can worsen after skeletal maturity • Curves over 30 degrees at the cessation of spinal growth are still likely to progress at a slow rate through adulthood
 • Scoliosis tends to worsen during growth • PGV")
Growth spurts (Peak Growth Velocity) • Scoliosis tends to worsen during growth • PGV refers to the time in an adolescent’s life when they experience the most rapid growth and thus the greatest risk of progression • The problem with measuring PGV is that it is retrospective; measuring growth only tells you after it happened • The average of PGV in girls is 11. 7 years • If you and the parents both believe the patient has yet to enter their growth spurt, the patient should be considered high risk

Determining the risk of progression • Patients less than 10 years of age with a Cobb angle of 20 degrees or more are very high risk; these cases should be referred out to an orthopedist or chiropractic scoliosis specialist (this includes infantile scoliosis). DO NOT ATTEMPT TO TREAT THEM YOURSELF! • Adolescent patients with a Cobb angle of 30 degrees or more (or braced patients) may also be high risk; err on the side of caution! • High risk cases should always be co managed alongside an orthopedic scoliosis specialist.

Determining the risk of progression • • • Chiropractors should feel comfortable accepting mild cases of idiopathic scoliosis (less than 25 degrees) in patients over 13 years of age, provided certain standards of care followed The first of these is proper documentation Second, scheduled re exams at regular intervals, including PA scoliosis radiographs Re exams should occur at least every 12 visits, and re x ray at least every six months If the patient improves or remains stable, continued treatment is justified with informed patient consent If the Cobb angle worsens by >5 degrees, referral to an orthopedist or chiropractic scoliosis specialist is the right thing to do!

Preparing a treatment plan for scoliosis • Be reasonable and cautious with your treatment plan; base it on 12 visits followed by a re exam • Determine what outcome assessments you will use to gauge the success or failure of care, and prepare a plan for what you will do if the patient does not respond as expected • Be realistic about what expect to achieve; the goal of wearing a brace 16 23/hr daily for 2 years is to prevent progression – what can you achieve in twelve 10 minute visits totaling 2 hours?

How to co manage scoliosis patients effectively

Co-management of scoliosis patients • It’s important to realize that every scoliosis patient will most likely consult with an orthopedic surgeon at least once • Overall, there is very limited evidence from which to draw conclusions about chiropractic scoliosis care • Avoid making unfounded statements or antagonistic remarks • Remember, it’s about the patient

Co-management of scoliosis patients • The patient has self selected this method as an alternative to watching and waiting • Research is lacking, but suggests basic chiropractic care and e stim are ineffective; so, don’t use these techniques • Emphasize what outcome measures will be used to gauge success, the timeframe of the re evaluations, and what will be done if the expected results are not achieved • Keep the focus on the patient and respecting their preferences. It’s not DC vs MD, it’s Patient & Doctors vs Scoliosis!

Principles of Evidence-Based Practice • The purpose of EBP is to “combine the best available scientific evidence with the doctor’s clinical expertise, in line with the preferences of the patient, to improve treatment outcomes. ” (Sackett 1996) • Patient preference is the first priority; all of the research in the world in favor of surgery/bracing is irrelevant if the patient has elected to avoid these procedures • SOSORT clinical guidelines suggest exercise based approaches are a reasonable treatment option for mild cases of scoliosis

Common scenarios • Justification for chiropractic care: emphasize patient choice, high satisfaction rates, low risk of progression in the patient, and low risk of side effects • Cobb angle disputes: request a copy of the report, pay attention to the selection of terminal vertebrae, and if necessary fall back on measurement error (4 8 degrees) – this is another reason why using AVR and functional metrics (such as spirometry) is very helpful

Common scenarios • Conflicts over bracing: focus on the purpose of bracing to stabilize the curve, the low risk of progression, and that chiropractic may stabilize mild curves without psychological side effects; ensure patient understands that bracing has been recommended by the orthopedist, provide your own recommendation, and then respect their choice to wear a brace or not to • Conflicts over the need for surgery: according to The Scoliosis Sourcebook, scoliosis surgery is NOT a medical emergency such as a ruptured appendix; set a timeline for care and be willing to refer out if the scoliosis increases in this timeframe, but emphasize patient choice

Chiropractic care of scoliosis • Find ways to establish a partnership • Regular status reports to the orthopedist as a common courtesy • Maintain the focus on the patient; avoid philosophical debates, “medical bashing, ” and irrelevant details which have no bearing on the patient’s specific situation

What NOT to do • • P A thoracic spine adjusting Ligament laxity and joint hypermobility Long term electrical muscle stimulation Diversified, full spine adjusting with postural counseling and shoe lifts • Adjusting the “high side of the rainbow”

Scoliosis spinal biomechanics • Normal thoracic kyphosis is defined as a Cobb angle of 20 to 40 degrees measured from T 2 to T 12 [in the sagittal plane] • Idiopathic scoliosis can only develop in patients with hypokyphosis of the thoracic spine • P A adjusting of the thoracic spine is contraindicated in scoliosis patients

Scoliosis spinal biomechanics • In scoliosis, the spinal cord and spinal column rotate in opposite directions • The laws of “coupled motion” are broken: spinous processes rotate into the direction of the lateral bend • The body adapts this unnatural rotation to prevent adverse mechanical tension (AMT) on the spinal cord

Scoliosis spinal biomechanics • DO NOT adjust on the high side of the rainbow for this reason • Attempting to push out the rotation without first reducing the AMT will increase the stress on the spinal cord; the body will not accept the correction • In order to reduce rotation, focus on correcting the sagittal curves FIRST; this takes tension off the spinal cord and gives you room to maneuver

Alar ligaments and proprioception • Idiopathic scoliosis patients tend to have a higher than normal amount of ligament laxity and joint hypermobility • Ligaments are not purely mechanical structures, but also play a role in proprioception and joint position sense • However, the ligaments in scoliosis patients have less mechanoreceptors than normal patients

Alar ligaments and proprioception • DMX studies reveal a high prevalence of upper cervical hypermobility in scoliosis patients • This is most likely due to increased laxity of the alar, ALL/PLL, and transverse ligaments; again, this laxity correlates with proprioceptive problems, which may be a causative and permissive factor in scoliosis • Manual cervical rotary/lateral flexion adjustments may be contraindicated in scoliosis patients for this reason

Alar ligaments and proprioception • APOM lateral flexion x rays can reveal alar ligament laxity • Lateral cervical flexion/extension x rays can reveal ALL, PLL, and transverse ligament instability • If upper cervical ligament laxity is present, utilize a mechanical adjusting instrument to adjust the cervical spine

Long term electrical stimulation • In the 1980’s, experiments were made into using e stim to halt the progression of scoliosis • In the 1990’s, long term research concluded that this approach was ineffective • However, many chiropractors are still using e stim to treat scoliosis

Long term electrical stimulation • Long term use of e stim has a negative effect upon the synapse, resulting in a loss of muscle tone • Functional disturbances of organs, endocrine glands, and muscle metabolism have also been reported • In animal studies, atrophy of fibers and degenerative lesions, necrosis, and hyperemia were found

“Damage to the neuromuscular system is an effect of long-term lateral electrical surface stimulation. Thus, standard LESS therapy may deepen [worsen] idiopathic scoliosis. ” Svarek et al. 2003

“Muscles of “overstimulated” rabbits exhibited clear signs of microscopical lesions, including depletion and disintegration of myofilaments, proliferation, dilatation and sometimes swelling of the sarcoplasmic reticulum and/or mitochondria, as well as signs of destruction of the Z line. ” Kowlaski et al. 2005

JMPT, Lantz et al 2001 • In 1997, the FCER funded a three year, $143, 000 study at Life College of Chiropractic West Public Clinic • The project studied the effect of chiropractic full spine procedures, heel lifts, and postural counseling in mild idiopathic scoliosis (less than 20 degrees) • Full spine adjustments were given one to three times a week over the course of one year

JMPT, Lantz et al 2001 • Of the 150 children who qualified for the study, 40 completed the year of care • The results showed an average reduction of 1. 4 degrees after one year of care • “CONCLUSION: Full-spine chiropractic adjustments with heel lifts and lifestyle counseling are not effective in reducing the severity of scoliotic curves. ”

JMPT, Lantz et al 2001 • • Don’t use heel lifts on a structural scoliosis Use scoliosis specific adjusting protocols Prescribe scoliosis specific exercises Document how what you’re doing is different • If you don’t know any scoliosis specific exercises, don’t treat scoliosis

It’s a question of value… and ethics • If this were your child, would you want you to treat it? Or would you prefer someone with more experience? • A scoliosis patient can easily spend $5, 000 on chiropractic care; the value of their investment is dependent upon the degree of your training in scoliosis. • You’re the expert; act like it. They have ONE CHANCE to change their spine (and their lives). Don’t ruin it for them.

Preliminary Results of the Scoliosis Reduction and Rehabilitation Protocol: A Pilot Study Mark W Morningstar, DC, Dennis Woggon, DC, Gary Lawrence, DC Abstract Purpose: To test the effectiveness of a new scoliosis specific chiropractic rehabilitation protocol Method: A total of 22 subjects were randomly selected to participate in the protocol. Anteroposterior radiographs were taken of each subject prior to treatment intervention and 4 6 weeks during the intervention. A Cobb angle was drawn and analyzed on each radiograph, so pre and post comparisons could be made. Results: After 4 -6 weeks of treatment, the entire sample size averaged a 62% reduction in their Cobb angle measurements. None of the patients’ Cobb angles increased. A total of 3 subjects were dismissed from the study for noncompliance relating to the home care instructions, leaving 19 subjects to be evaluated post intervention. Conclusion: The Scoliosis Reduction and Rehabilitation Protocol appeared to markedly reduce the severity of the Cobb angle in all 19 subjects. These results warrant further testing of this protocol.
 Subject # Initial Post % 1")
Cobb Angle Measurements After 4 -6 Weeks (Degrees) Subject # Initial Post % 1 32 24 25 2 23 8 3 29 4 Initial Post % 11 40 22 45 65 12 31 9 71 11 62 13 27 14 48 52 19 63 14 33 7 79 5 19 4 79 15 32 18 44 6 28 11 61 16 16 4 75 7 16 2 88 17 15 4 73 8 25 11 56 18 21 6 71 9 35 20 43 19 38 11 71 10 28 13 54 Average Reduction Among All Subjects: 62% in 4 -6 Weeks Subject # 8/19 No Scoliosis Average Reduction: 28 to 11 degrees

Research #1 Most Highly Accessed Article of All-Time BMC Musculoskeletal Disorders 2004 “Scoliosis treatment using a combination of manipulative and rehabilitative therapy” 55, 926 hits as of 3 -25 -2013 (number two on chronic, non-specific LBP = 41, 401 hits)

CLEAR Scoliosis Treatment • X rays are taken to create a 3 dimensional picture of the spine • Adjustments, therapies, and exercises are applied based upon the individual x ray measurements • Post x rays taken with identical positioning can validate the changes in spinal and pelvic alignment

Concerns about x ray exposure • The total amount of radiation from one full CLEAR x ray examination is 1. 5 m. Sv. • The average radiation exposure from environmental sources annually is 2. 4 m. Sv. • “Below 100 m. Sv, risks of health effects are either too small to be observed or are nonexistent. ” Radiation Risk in Perspective: Position Statement of the Health Physics Society, Revised August 2004. • Request a copy of the CLEAR X-Ray Safety Guidelines for more information.

CLEAR Scoliosis Specific Radiographic Protocol II. Radiographic Analysis: 77 total measurements A. Cervical series 1. 2. 3. 4. 5. Lateral cervical neutral: 11 measurements Lateral cervical flexion: 13 measurements Lateral cervical extension: 13 measurements A P Open Mouth cervicodorsal: 6 measurements Base Posterior (Vertex): 3 measurements B. Lumbar series 1. 2. A P lumbar: 8 measurements Lateral lumbar: 8 measurements C. Scoliosis series 1. 2. P A scoliosis: 11 measurements P A left and right lateral bending: 4 measurements

Measurements are made on the radiographs to quantify the degree of sagittal, coronal, and axial spinal misalignment. This information is then used to determine the specific manual and instrument assisted manipulative therapies, the spinal weighting protocols, and physical therapies that will be applied in each case.

Treatment Procedure Treatment sessions are approximately two hours long, and consist of three phases, informally termed, “Mix, Fix, and Set. ” The first phase is designed to address the soft tissues, the second phase influences spinal biomechanics, and the third phase is designed to affect proprioception and neuromuscular function. The first phase has six parts: active spinal mobility exercises, passive vibration therapy, active cervical traction exercises, massage therapy, passive flexion distraction therapy, and mobilization therapy. The second phase consisted of CMT. Supine thoracic, prone lumbar, side posture pelvic manual manipulations, and, seated cervical instrument assisted manipulations were performed. The third phase consisted of three parts: reactive body weighting therapy, isometric spinal exercises, and vibration therapy.

Active spinal mobility exercises are performed with the patient seated upon a chair with a seat that pivots in a 360 -degree range of motion. Initially, the patient performs general stretching exercises, followed by spinal range of motion exercises. Lastly, repetitive lateral bending exercises are performed in the direction of the convexity of each curve with the patient’s hand positioned at the apex.

Passive vibration therapy consists of the patient lying supine with a cylinder below the cervical and/or lumbar lordosis that oscillates at a frequency of 4 Hertz, which may have a lengthening effect upon the spine, as well as additional supports and/or wedges designed to create a “mirror-image” position of the patient’s typical posture.

Active spinal traction exercises are performed by the patient in a standing position. While positioned in this device, the patient bends the knees to gently traction the spine, then straightens the legs and repeats this maneuver 60 to 100 times. These axial traction exercises are performed in a manner to emphasize the cervical lordosis and ideal sagittal spinal alignment. Repetitive loading and unloading of the spine may have a beneficial effect upon the intervertebral discs.

The patient lies supine on a specialized table. Lateral traction straps and raised wedges are used to create a “mirror-image” of the patient’s postural configuration. While in this position, a motor flexes the lower section of the table repeatedly by approximately 30 degrees, then returns, providing continuous passive motion that intermittently axially tractions and then relaxes the spine. This intermittent axial traction combined with the “mirror-image” positioning may have a beneficial effect upon the soft tissues surrounding the spine and the intervertebral discs.

The patient was positioned supine with a motorized wedge placed underneath the shoulders, torso, and/or pelvis. This wedge has an electric motor that raises and lowers approximately ½-inch six times per second. The goal is to duplicate the effect of CMT; for instance, by placing it underneath the right side of the torso, the rotation of the thoracic spine and rib cage may be addressed. Additional foam wedges were positioned beneath the patient for stability and to enhance a “mirror-image” effect.

Adjustments are delivered based upon the results of the x-rays. For instance, if the x-rays demonstrate a loss of the thoracic curve, no prone P-A adjusting of the thoracic spine is performed, only A-P supine adjustments. Side posture adjustments take into account the measured pelvic rotation, and utilize tractive forces rather than compressive forces.

CMT is applied to the cervical spine with the aid of a mechanical adjusting instrument. The goal is to reduce forward head posture and reduce any misalignments noted on the cervical x-rays. A mechanical instrument is used in lieu of manual CMT to avoid aggravating any hypermobility that may be present in the cervical spine.

After CMT, the patient performs isometric lateral flexion and/or rotation exercises. In this picture, the patient is seated and laterally flexes to the left, then holds this position. Additional exercises may be performed either seated or standing, and either laterally flexed or rotated to either the left or right. The goal of these exercises are to engage and strengthen specific paraspinal muscles. Whole-body vibration therapy is applied while the patient performs these exercises in an attempt to enhance rehabilitation of the neuromuscular system.

The patient is positioned in an adjustable chair that combines axial traction with lateral traction, de rotation, and whole body vibration. Active isometric exercises are performed by the patient while they are in this chair. The goal is to restore normal sagittal spinal alignment, create a “mirror image” of the patient’s coronal and axial posture and spinal configuration, engage specific paraspinal muscle groups, and utilize vibratory stimulation to enhance neuromuscular rehabilitation.

Weights and/or cantilevers are strategically placed on the head, shoulders, torso, and/or hips, according to the patient’s clinical and radiographic presentation. The patient stands on an unstable surface (such as an air-filled balance training disc), placed on top of a whole-body vibration platform. The purpose is to cause the paraspinal muscles of the body to react in a manner which will effect a de-rotation and detranslation of the spine, and to stimulate the neuromuscular pathways responsible for automatic postural control.

Scoliosis Case Studies CLEAR Scoliosis Patients

Sadi 12 th Visit



 12 th Visit")
Pre Lat Cervical Head Wt & Glasses (3 rd Visit) 12 th Visit

5 th Visit

5 th Visit

12 th Visit

Sadi 12 th Visit

Jamie 6 Total Adjustments and Exercises Only

Sarah 2002 1/2003 03/31/03

03/14/05 01/04/08 3/17/08

Sarah - 12 Visits

Amanda

Amanda’s Story "People who say that it can't be done should not interrupt those of us who are doing it!" The unknown author of this quote precisely explained my thoughts and feelings after completing five days at the CLEAR Institute with Dr. Dennis Woggon. Although I knew I wanted to become a Chiropractor from a young age, it wasn’t until I started at Palmer that I become intrigued learning about and correcting Scoliosis, especially my own. Perhaps from my eagerness to answer the ‘why’s’ in life, I cannot and will not accept that my scoliosis is idiopathic. I am determined to discover how this condition was conceived in myself, and how, in others, it is born. Fueling the flame further, I found no answers at school, the place where chiropractors become experts on the spine, nervous, and muscular systems. Too many times, I hear, “Besides pain management, there is nothing chiropractic can do for patients with Scoliosis. ”

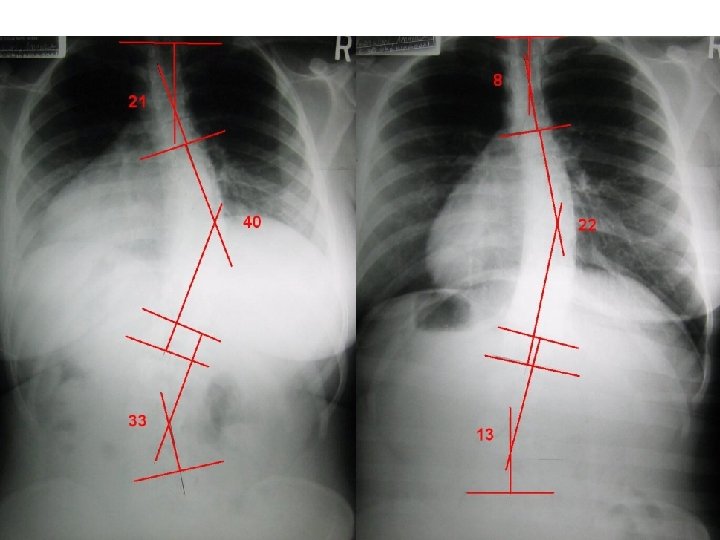
I arrived on a Monday morning at the St. Cloud Chiropractic Clinic not sure what to expect. De. Jeanne Denet, an upper quarter student, accompanied me. With a scoliosis worse than mine, and this being her second visit to the clinic, gave me a sense encouragement. I was surprised to find Dr. Woggon already at the clinic treating patients at 7: 30 that morning. After I filled out a history and evaluation, Dr. Woggon took my X-rays. I was shocked to find out how bad my scoliosis actually was: 142% loss of cervical lordosis, 1. 4 inches of forward head posture, 24 pounds apparent head weight and a triple curve scoliosis with angles measuring 21 degrees upper dorsal, 40 degrees lower dorsal, and 33 degrees lumbar curvatures.

Now that we had a blueprint to my spine, the work began. Each morning and afternoon for the next four days, I wobbled, performed cervical traction, stretched, exercised, warmed my spine up, and got adjusted. In addition to those treatments, I sat in the Scoliosis Traction Chair for 30 minutes. After the chair, I concluded each session with wearing head weights and hip weights while having to walk blindfolded on a tightrope. After 6 hours of treatment a day, I experienced great exhaustion, not only physically but emotionally as well. I often napped after the morning treatments on my lunch break, and I longed for my bed with the conclusion of the afternoon sessions.

It was Monday morning when I received my first adjustment, and had a peculiar emotional response. I choked back the tears, trying not to let my new Chiropractor see my tears. I wanted him to be proud of how strong I was… silly thoughts, now when I look back. Later that week, I watched Dr. Woggon adjust another scoliosis patient, and saw she had the same response I had. The hardest day was after the second day of treatments. Although De. Jeanne was staying with me, I longed for family and friends. Besides having headaches, I also was sore from the treatments, physically exhausted, and emotionally unstable. I dug deep and carried on, giving it all I had to give. Surprisingly, I woke the next morning, feeling better than the first two days. That morning we took another X-ray of my cervical curve to make sure I was responding to treatment. Seeing my neck reversing back to a lordotic curve, filled my soul with encouragement and strength to keep working hard. The days flew by after that. It seemed my body was adapting to the treatments and its new form.

I woke Friday morning excited, wondering how my spine had changed. Did the treatments work on me? I soon found out when Dr. Woggon took my last set of X-rays. He put the X-rays of my cervicals and scoliotic spine on the view box. A rush came over my whole body when I saw my new form. My triple curve scoliosis went from 21 degrees in the upper dorsals to 8 degrees, 40 degrees in the mid dorsals to 22 degrees, and 33 degrees in the lumbars to 13 degrees! My cervical lordosis went from a loss of 142% to a loss of only 90% and a reduction of forward head posture by 11 pounds and 2. 1 inches. My strength and range of motions all improved dramatically, and my lung capacity went from 3100 cc to 3300 cc. By the rehydration of my discs and the straightening of my spine, I was a half-inch taller. Overall, I was amazed by the results.

In the days following my treatment at the CLEAR Institute, I began to realize how much better I felt. (These new feelings are hard to explain, and probably even harder for others to relate to. ) I had a new sense of who I was after my trip to CLEAR. I felt like I had a heavy fog lifted off me. Things like my self-esteem, mental capability, concentration, hearing, vision, and overall well-being were all enhanced. As strange as it may sound, it was as if I was looking at the world and experiencing life in a new, brighter dimension. Although all this was remarkable, I believe it was my satisfaction with the fact chiropractic care for scoliotic patients truly was possible and it was EXISTENT. . . after all, I had experienced it myself. Thus, for all those who are indifferent and not in agreement, I leave you with my opening quote, one in which Dr. Woggon uses frequently, "People who say that it can't be done should not interrupt those of us who are doing it!"

De. Jeanne

De. Jeanne: Thoracic: 62 – 31 – 22 Lumbar: 70 – 46 – 38

Sharon – 55 y/o female

Marvin – 84 Years Young 43 / 42 January 2006 29 / 34 March 2006 23 / 28 October 2006 14 / 17 March 2007

Additional Resources • BEST SCOLIOSIS BOOK EVER: Scoliosis and the Human Spine, by Martha Hawes Ph. D – www. scoliosis. org • CLEAR scoliosis seminars available at Parker and online – www. clear institute. org • Upper Cervical Subluxation Complex: A review of the chiropractic and medical literature, by Kirk Eriksen DC
- Slides: 110