Welcome to Applied Outbreak Investigation Please help yourself

Welcome to Applied Outbreak Investigation • Please help yourself to breakfast • Please sign-in on the attendance sheet • Please find your seat (names listed on table tents)
![Applied Outbreak Investigation Presented by [Names and agencies] [Date and location]](http://slidetodoc.com/presentation_image_h/e7b97fa9d883bc190f6fdc03a9e08223/image-2.jpg "Applied Outbreak Investigation Presented by [Names and agencies] [Date and location]")
Applied Outbreak Investigation Presented by [Names and agencies] [Date and location]

Welcome Housekeeping: Facilities Food Breaks

Introductions • Name, Agency, Position • Have you ever investigated an enteric disease outbreak?

Objectives After completing this training, participants will: • Be able to define what constitutes an outbreak. • Be able to identify when an outbreak investigation is necessary. • Understand practice the basic steps of an outbreak investigation. • Understand the roles and responsibilities of epidemiology, environmental health, and laboratory in an outbreak investigation.
 After completing this training, participants will: • Be aware of and know")
Objectives (continued) After completing this training, participants will: • Be aware of and know how and when to use outbreak resources and tools available to assist local public health agencies during outbreaks. • Know how to document and report on outbreak findings. • Be aware of communication strategies to employ during an outbreak.

Structure of this training • Interactive training modules – Clicker voting • STEPS in an outbreak investigation – Not numbered because each outbreak is unique – May not need to do each step in every outbreak – Outbreaks require flexibility – Follow along on paper copy, laminated copy for reference • Outbreak scenario • * = Resources and tools

Overview of State/Local Outbreak Data
![[Insert 5 slides covering] • All outbreaks by mode of transmission • 5 yr](http://slidetodoc.com/presentation_image_h/e7b97fa9d883bc190f6fdc03a9e08223/image-9.jpg "[Insert 5 slides covering] • All outbreaks by mode of transmission • 5 yr")
[Insert 5 slides covering] • All outbreaks by mode of transmission • 5 yr foodborne outbreak count • Breakdown of pathogens responsible for foodborne outbreaks • Breakdown of how foodborne outbreaks are detected: complaint vs. routine surveillance • Breakdown of foodborne outbreaks by setting

State Information

State Information

State Information

State Information

Establish Existence of an Outbreak *STEP

What is an Outbreak? • Occurrence of more cases of a disease than is expected in a given area, or among a specific group of people, over a particular period of time. • Foodborne Outbreak (CDC definition): similar illness in 2 or more people after consuming the same food item in the US.

Primary Goals of Outbreak Investigations • Stop current outbreak as soon as possible by implementing effective control measures • Prevent similar outbreaks in future • Contribute to food safety and public health policy
 Pathogen-specific surveillance")
Two Main Ways to Detect Outbreaks Notification/ complaint system (on the phone) Pathogen-specific surveillance (on the computer) All (any symptoms) Only selected diseases (reportable conditions) Consumer complaint (“We puked after eating burgers”) Positive lab results (stool culture positive) Common exposures Same pathogen Excluding unrelated cases Difficult (no lab tests, many exposures) Easier (PFGE match!) Detection speed Faster (time it takes to make a phone call) Slower (time it takes to seek care, be tested, be reported…) Localized; short incubation (norovirus at an office party) Widespread; long incubation (Hepatitis A in a commercial product) Types of foodborne illnesses detected Initiating event Linking cases Types of outbreaks best detected

Jim calls to report an outbreak at Mc. Donald’s. He dined alone, ate 3 Big Macs®, and developed abdominal cramps and explosive diarrhea within 15 minutes of completing his meal. Your health department has not received other complaints about this facility. Is this an outbreak? A. Yes B. No C. I don’t know

A school nurse calls on Thursday morning to report that a bunch of kids are out sick today. A few parents mentioned that their kids have “the flu. ” Is this an outbreak? A. Yes B. No C. I don’t know

A conference organizer calls you from Idaho to report that she hosted an underwater basket-weaving conference in your jurisdiction two weeks ago. She received complaints from 20% of attendees, from multiple states, that they developed gastrointestinal symptoms within 24 hours of returning home. One person saw a doctor and was diagnosed with Salmonella. Is this an outbreak? A. Yes B. No C. I don’t know

Prioritization • Limited resources in public health • High priority investigations: – Life threatening illness – Population at high risk for complications – Large number of affected persons – Exposure could be on-going – New cases being reported – Political pressure – Anything that could have been caused intentionally

Who leads the investigation? • Generally, local PH agency leads outbreaks when the exposure and/or the majority of ill people reside within their jurisdiction – With assistance from state health departments as needed • State health departments typically lead: – Multistate clusters/outbreaks – Multicounty clusters/outbreaks

• You work at Mountain County Public Health. • It is Friday, December 19, at 3: 00 pm. • You receive a Shiga Toxin-Producing E. coli (STEC) case in your surveillance system which has been confirmed at the state lab as E. coli O 157: H 7. • You promptly contact the case, a 25 year old male; he reports that he ate the majority of his meals out in the week prior to his illness. • He says his roommate has also had some diarrhea in the last week.
: pathogenic; different")
E. coli O 157: H 7 • Shiga toxin-producing E. coli (STEC): pathogenic; different than E. coli found in our guts Symptoms Diarrhea (often bloody), abdominal pain, sometimes vomiting and fever Incubation Period 1 – 10 days (avg 3 -4) Duration Up to 12 days (can shed for longer) Transmission Contaminated food/water (especially ground beef, produce); fecal-oral (animal-to-human, human-tohuman) Reservoir Gut of cattle, deer, elk, goats, other animals Special Considerations Low infectious dose; important cause of hemolytic uremic syndrome (HUS) in children; can persist in environment

TIMELINE: DECEMBER 2014 SUN MON TUE WED THU FRI SAT 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 Initial STEC case report

Is this an Outbreak? A. Yes B. No C. I don’t know

• On Monday morning, December 22, you receive a phone call from Rita, a resident of Valley County (a county adjacent to you). • Rita and members of her Frisbee Golf team have experienced “stomach flu” over the past week. • Over a week ago, during the weekend of December 6 -7, they participated in a Frisbee Golf tournament in Mountain County.

TIMELINE: DECEMBER 2014 SUN MON TUE WED THU FRI SAT 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 Complaint call Frisbee Golf Team ill Initial STEC case report

What questions would you ask?

From your interview with Rita, you learn: • There are 18 adult players on the team. • Team members live in Mountain, Valley, and Plateau Counties. • Rita knows that at least 4 have been sick with some sort of GI symptoms since the tournament, but does not know their exact symptoms. Rita has been ill as well. • One ill person is currently hospitalized in Plateau County. • While in Mountain County, the team dined at Burger Central and Deli Queen on December 7.

After talking to Rita, you logged the complaint into Mountain County’s *foodborne illness complaint system. Here’s a copy of the abbreviated complaint log. What are you concerned about?

TIMELINE: DECEMBER 2014 SUN MON TUE WED THU FRI SAT 1 2 3 4 5 6 Initial STEC case at Deli Queen 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 Frisbee Golf Team ate at Deli Queen Complaint call Frisbee Golf Team ill Initial STEC case report

Is this an Outbreak? A. Yes B. No C. I don’t know

• You report the outbreak to the state health department and begin your investigation.

Form a team STEP

Three Legged Stool Administrative Staff Communication EPR IT ry Environment Ep to ide ra mi bo ol o La gy Leadership

Investigation Team • Identify local, regional, and state resources • Size of team depends on etiology, setting, number of affected people, etc. • Some jurisdictions set up “Outbreak Response Teams” ahead of time • Designate a Leader (could be Epi, EH, director, EPR staff, etc. )
 • ICS: a standardized approach to coordinate, manage,")
Consider using Incident Command System (ICS) • ICS: a standardized approach to coordinate, manage, and organize incidents and resources • ICS can be used in outbreak investigations, especially larger/protracted investigations • Training resource: North Carolina Center for Public Health Preparedness – “ICS in Action: Using the Incident Command System in Public Health Outbreak Investigations” http: //cphp. sph. unc. edu/trainingpackages/ics_in_ action/ • *Sample ICS structure on resource website

Sample ICS Structure Incident Commander Public Information Officer Planning Section Chief Surveillance & Investigations Branch Interviewing Unit Specimen Collection Unit Deputy Incident Commander Consumer Protection Branch Restaurant Inspection Unit Epidemiology Branch Data Analysis Unit

You form your investigation team. *Back at your office, you can use the “Outbreak Team Members” resource on the resource website to create your office’s outbreak team.

Attempt to identify etiology STEP

Etiology is…. Known Unknown Detection method Pathogen-based surveillance Complaint-based surveillance Symptoms Interview patient to learn if Collect specific symptoms are consistent information and duration of with etiology. illness Onset date Helps determine exposure If exposure date is known date using incubation period (ex wedding party), use to calculate incubation period Lab tests Review results from clinical lab, make sure specimen being forwarded to public health lab Collect stool for testing Resources Pathogen-based disease reporting system, communicable disease manual, CDC website, *enteric pathogen table CIFOR symptom table: http: //www. cifor. us/docum ents/CIFORGuidelines. Appen dices. pdf

Specimen Testing at State Public Health Lab

Laboratory Supplies • It is helpful to keep supplies on hand at your agency. – Bulk stool containers and biohazard bags do not expire – Accessories: “hats, ” spoons, gloves, labels have a long shelf life – Bacterial transport media swabs (Cary Blair, Amies) have short shelf life, so check the expiration date before using • When working with specimens, follow your agency’s biohazard plan

Specimen Testing at CDPHE Lab In most outbreak situations, CDPHE can support testing specimens at CDPHE lab Exceptions: person-to-person outbreaks in LTCFs or child care centers that are consistent with norovirus/viral gastroenteritis
![[State specific lab info] Info on how to get supplies What testing can be](http://slidetodoc.com/presentation_image_h/e7b97fa9d883bc190f6fdc03a9e08223/image-46.jpg "[State specific lab info] Info on how to get supplies What testing can be")
[State specific lab info] Info on how to get supplies What testing can be performed Lab form and how to complete it Labeling/identification requirements for specimens • Transport/courier • •

Completing Lab Paperwork • https: //www. youtube. com/watch? v=ay. BXmt. W b. Or 0

Collecting and Submitting Specimens • https: //www. youtube. com/watch? v=BLm 4 f. Cyj 1 CY&feature=youtu. be

Getting Specimens to the Lab • Hand-delivered – Specimen receiving door (SE corner of building) • Courier [Insert State information] • Fed. Ex or other shipping service – Biohazard sticker and “Diagnostic Specimen UN 3373” Lab hours: [State Lab Hours]

Interpretation of Stool Specimen Testing • Positive for certain agent – Patient’s illness caused by agent – Patient colonized with agent but illness not caused by agent – Contamination of specimen • Negative for certain agent – Patient’s illness not caused by agent (caused by another agent requiring different testing) – Collected too late in course of illness – Specimen handled improperly

• When talking to Rita on Monday, December 22, she agreed to provide a stool specimen to public health for testing. • Using her bulk stool sample, prepare a bacterial culture swab and package for transport.

• Please complete the specimen and testing sections of the lab form. Consider the symptom profile when deciding which tests to select. • How would you get the specimen to the state public health lab from YOUR public health agency?

Define and identify cases STEP

Establish a Case Definition • What is a “case”? • Typically contains the following elements: – Clinical information and/or laboratory results. – Characteristics about the people affected (person). – Information about the place of exposure (place). – Time during which the outbreak occurred (time).

Example Case Definition • A case is defined as an individual experiencing diarrhea (defined as at least three loose stools in a 24 -hour period) and dined at “Restaurant X” between January 15 and January 25.

Case Definitions are Important • Accurately capturing who is and isn’t part of an outbreak • Allows you to describe your outbreak in order to implement appropriate public health action • Reduces bias in your results • They allow you to test hypotheses – Do NOT include suspected vehicle of outbreak (i. e. , hypothesis you are trying to test)

A case is defined as a person who attends or works at “Child Care Center X” who became ill with vomiting and/or diarrhea (defined as at least 3 loose stools in a 24 hour period) whose symptoms lasted less than 72 hours. What is missing from this child care center outbreak case definition? A. B. C. D. Person Place Time Clinical Information

A confirmed case is defined as an individual with laboratory confirmed Salmonella Typhimurium between January 15 and January 25. What is missing from this outbreak case definition? A. B. C. D. Person Place Time Clinical Information

What is wrong with this case definition? A case is defined as an ogre living in the swamp near Lord Farquaad’s Kingdom experiencing diarrhea (defined as 3 or more loose stools in 24 hours), with onset after eating cake at Shrek and Fiona’s wedding. A. Ogres are not people B. The place is missing C. Suspected vehicle is included in case definition D. Nothing, this is a good case definition

More on Case Definitions • You may have separate definitions for confirmed, probable, and suspect cases. • Case definitions are often changed and refined as more information about the outbreak is gathered. – Usually, your initial case definition does not include any suspected sources of the outbreak Analyze your data using your case definitions!

Example Case Definitions • Confirmed: Laboratory –confirmed case of Shigella in a child or staff member at childcare center A with onset since January 29, 2014. • Probable: A child or staff member at childcare center A with diarrhea (defined as 3 or more loose stools in a 24 -hour period) for 72 hours or more, with onset since January 29, 2014. • Suspect: A child or staff member at childcare center A with gastrointestinal symptoms.

Case Finding • Cast a wide net to identify population at risk • Identified cases may be “tip of the iceberg” • Surveillance methods: – Passive Surveillance: Health care providers and laboratories report cases of disease to health department – Active Surveillance: Health department contacts health care providers (or others) requesting information about conditions or diseases to identify possible cases

Pyramid of Reporting Reported to Health Dept Laboratory confirmed case Lab tests for organism Specimen obtained Person seeks care Person becomes ill Exposure in the general population Public health surveillance

Case Finding Methods • • • Which of these methods are passive surveillance? Ask organizer for a list of attendees Routine notifiable disease surveillance Email other local public health agencies National outbreak email list serves/web boards Reservation lists / credit card sales Web orders Contact ERs, local medical offices, labs – health alerts Other cases—is anyone else ill? Review complaints received at the health dept Press release *Sample health alerts, press releases, letters to schools/childcares

• On Tuesday, December 23, the local hospital calls to say that they have another case of STEC in a 7 year old girl. • Upon interviewing her mother, she dined at Deli Queen on Monday, December 8. • On Friday, December 26 you receive results from Rita’s stool specimen that was tested at the State Public Health Laboratory – it is positive for STEC O 157.

TIMELINE: DECEMBER 2014 SUN MON TUE WED THU FRI SAT 1 2 3 4 5 6 Initial STEC case at Deli Queen 7 Frisbee Golf Team ate at Deli Queen 8 2 nd STEC case 9 10 11 12 13 ate at Deli Queen 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 Complaint call Frisbee Golf Team ill 2 nd STEC case report Initial STEC case report Rita – stool tests positive for STEC

Create a case definition Remember to include: • Person • Place • Time • Clinical information

How do we identify additional cases?
 STEP")
Describe and orient the data (DESCRIPTIVE EPIDEMIOLOGY) STEP

Line List • Contains basic information about each person suspected to be part of a cluster or outbreak – Allows information about time, person, and place to be organized and reviewed – Best to develop in an electronic format (Excel, Access, Epi Info) • In large outbreaks, designate one person to be in-charge of the line list (full time job)

Line List Example *Line list template § Each row represents one person § Each column represents a variable of interest § Can add/take out variables as needed

Descriptive Epidemiology Clues • Person-to-person transmission – Clustering in social units – Localized to one part of community – Occurrence of cases in waves • Transmission by public drinking water – Widespread illness – Affecting both sexes and all age groups – Distribution consistent with public water system • Transmission by food – Increased risk among certain groups – Distribution similar to distribution of foods

What can your data tell you? Who is ill? E. coli O 157 – 2009 – 80 cases – 31 states Unique vehicle for this pathogen – consuming prepackaged raw cookie dough

What can your data tell you? What might be the etiology? Symptoms Diarrhea Bloody diarrhea Abdominal pain Fever Myalgia Vomiting Hospitalized n 51/51 12/44 40/49 36/48 24/47 18/48 3/51 % 100 27 81 75 64 37 6

What can your data tell you?

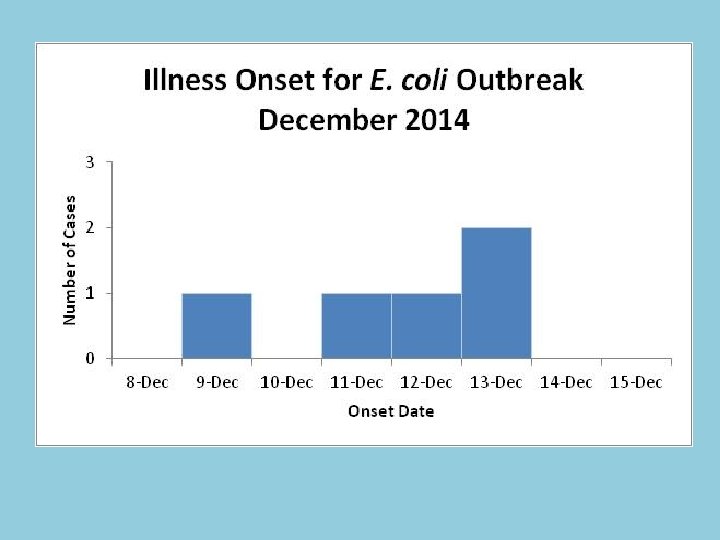
Construct an Epidemic Curve 1. Title your epi curve 2. Create your horizontal axis: TIME – Preferably use onset date – Units ¼ to ½ of incubation period work best – Consider adding an incubation period to the x-axis on both sides of the cases 3. 4. 5. 6. Create your vertical axis: NUMBER OF CASES Build a histogram using your line list Note important events (optional) Interpret your epi curve

Uses of Epi Curves • • Grasp magnitude of outbreak Clarify outbreak’s timeline Identify cases that are outliers Draw inferences about pattern of spread – Point source outbreak – Continuous common source outbreak – Propagated outbreak

Point Source Outbreak • Exposure to same source over brief time • Cases rise rapidly to a peak and fall off gradually • Majority of cases within one incubation period Cryptosporidiosis cases, June one incubation period = 7 days

Continuous Common Source Outbreak • Exposure to same source over prolonged time • Epidemic curve rises gradually • May plateau Infections with Salmonella Enteritidis by date of onset of illness, January and February. one incubation period = 2 -3 days January February

Propagated Outbreak • Spread from person to person • Series of progressively taller peaks • Peaks one incubation period apart Measles cases by date of onset of illness, Aberdeen, South Dakota, October 15 – January 16 one incubation period = 10 days October November December January
 B. Point-Source")
What type of outbreak does this Epi Curve demonstrate? A. Person-to-Person (propagated) B. Point-Source C. Continuous Common Source
 B.")
What type of outbreak does this Epi Curve demonstrate? A. Person-to. Person (propagated) B. Point-Source C. Continuous Common Source
 B.")
What type of outbreak does this Epi Curve demonstrate? A. Person-to. Person (propagated) B. Point-Source C. Continuous Common Source

Let’s Review the Outbreak! • You are investigating an enteric disease outbreak • There are 5 ill people who meet confirmed and probable case definitions – 2 identified through public health surveillance – 3 are members of the frisbee golf team; illness was discovered through a complaint call – All cases report eating at Deli Queen between December 5 th and 8 th

• You have some information on 6 ill people that you put into a line list: – Rita – 3 other team members, one hospitalized – Initial reported case - 25 year old STEC case – Second reported case - 7 year old hospitalized STEC case

Tabulate and Describe Study Data • Apply your case definition • Calculate basic descriptive data – % male/female – Median age (range) – Symptom description – % hospitalized – Any deaths – Etc.

Using the data in the line list, calculate: • % male/female • Median age (range) • Symptom description (frequency and %) … this data will populate “Table 1. ”
 Number Percent Male 2")
Table 1. Description of Cases Median Range 49 (7 -55) Number Percent Male 2 40% Female 3 60% Diarrhea 5 100% Bloody Diarrhea 5 100% Abdominal Cramps 5 100% Vomiting 2 40% Fever 4 80% Headache 4 80% Body Aches 3 60% Hospitalizations 2 40% Deaths 0 0 Age Sex Symptoms

• From this line list, apply your case definition and construct an epi curve

TIMELINE: DECEMBER 2014 SUN MON TUE WED THU FRI SAT 1 2 3 4 5 6 Initial STEC case at Deli Queen 7 Frisbee Golf Team ate at Deli Queen 8 2 nd STEC case 9 10 11 12 13 ate at Deli Queen 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 Complaint call Frisbee Golf Team ill 2 nd STEC case report Initial STEC case report Rita – stool tests positive for STEC

Develop hypothesis STEP

Developing a Hypothesis • Using available information to make an educated guess about the cause and source of an outbreak • Purpose – To direct immediate control measures – To narrow focus of subsequent studies – To determine the need to involve others in investigation • Undertaken by entire team

Elements of a Hypothesis • Includes likely causative agent, people at risk, mode of transmission, vehicle, and period of interest • Example: “The outbreak is due to a bacterium that was spread during the first week of November by a food commonly consumed by children. ”

Key Sources of Information • Basic information about causative agent • Information on implicated facility or food • Descriptive epidemiology (i. e. , describe cases by time, place, and person) • Case interviews (“hypothesis-generating interviews”)

What is your leading hypothesis? • Using the data you have, what is your leading hypothesis? – Includes likely causative agent, people at risk, mode of transmission, vehicle, and period of interest • What are some other possible hypotheses?

Evaluate hypothesis - Epi STEP

Purpose of an Epi Study • Test a hypothesis • Compare ill cases to people who did not become ill to see if commonalities are: – Reflective of population at large? – A chance happening? – Related to an unknown factor? • Two common analytical studies are cohort study and case-control study • *Study Design Handout

Cohort Study • Population is well defined • Start with who is exposed, then determine who is ill • Examples: church potluck, wedding, school class, jail Ate food Did not eat food Illness No illness

Case-Control Study • Population is NOT well defined • Start with who is ill, then determine who ate food • Identify potential controls – Random or sequential digit dialing – Neighborhood controls • Example: Matching PFGE pattern in different states Ate food Did not eat food Cases Controls

How to choose? • Are members of the group easily identifiable? • What is known about the exposure-disease relationship? • What resources do you have?

A local health department receives reports of gastrointestinal illness from attendees of a polka festival in the local county. Which study design would you use? A. Cohort study B. Case-control study

An estimated 1, 200 people attended a conference. Food trucks served food during the event, none of which were licensed, and many people became ill. The conference is now over, and most attendees have returned home. Which study design would you use? A. Cohort B. Case-control

A total of 11 people are infected with a matching strain of Salmonella in three states. Which study design would you use? A. Cohort B. Case-control

Several members of a cow share ill with Campylobacter. Which study design would you use? A. Cohort B. Case-control

There is an E. coli O 157 outbreak with 9 ill cases in the Denver Metro Area. Which study design would you use? A. Cohort B. Case-control

What type of study would you conduct for this outbreak?

• You decided to do a cohort study with the Frisbee Golf Team. You would then develop a questionnaire based on the Deli Queen menu.

Develop Questionnaire • First, talk to your colleagues at state and local health departments. There is probably another questionnaire or template you can modify. Don’t reinvent the wheel!

• Here is the questionnaire used for this outbreak.

Questionnaire Components • • • Introduction Demographics on respondent Illness information Exposure information Secondary transmission Conclusion/follow-up

Questionnaire Database • Microsoft Access, Excel, Epi Info 7 • Database should mirror questionnaire to allow for easy data entry

Example: Epi Info Form Free software developed by CDC for the public health community Performs data: - collection - management - analysis - visualization Download at: http: //wwwn. cdc. gov/epiinfo /html/downloads. htm

Questionnaire and Database Tips • • Write questions in an unbiased manner Do not use “leading” or “loaded” questions Keep each question brief, simple and specific For every field you create, ask yourself: – What is the intent of this question? – Will people answering the survey understand the question? (avoid jargon, abbreviations, etc. ) – What type of answers/data am I looking for? • i. e. , numeric, text, date, time, etc. – How will I analyze this data?

Update your epi curve with this additional information

It’s stats time! 1. 2. 3. 4. Choose the correct measure of association Complete 2 x 2 tables Use Epi Info to calculate Interpret the results *Study Design & Analysis Tool

1. Choose Measure of Association • Cohort study: calculate relative risks (also called a risk ratio) • Case-Control study: calculate odds ratios • How? Epi Info 7 is a free tool that can do all of this

• Which measure of association should we calculate?

2. Complete 2 x 2 Tables Cases or Ill Controls or Well Ate food item or exposed a b Did not eat food item or not exposed c d a = cases who were exposed b = controls who were exposed c = cases who were not exposed d = controls who were not exposed

• *Here’s the new line list that includes some exposure data • Who do we include in cohort analysis? • Create 2 x 2 tables for each food item on the line list.

3. Use Epi Info*

• Together, using Epi Info STAT CALC, let’s calculate relative risks for each food item.

4. Interpret Odds Ratio Close to 1. 0 Odds of exposure is similar among cases and controls Relative Risk Interpretation Risk of disease is Exposure not similar among exposed associated with illness and not exposed Greater than 1. 0 Odds of exposure Risk of disease is Exposure could be a among cases is higher among exposed risk factor for illness than among controls than not exposed Less than 1. 0 Odds of exposure Risk of disease is lower Exposure could be a among cases is lower among exposed than “protective factor” than among controls not exposed Magnitude Reflects strength of association between exposure and illness

• Let’s interpret our relative risks

Food Results ATE FOOD Veggie Sandwich Turkey Sandwich Ill DID NOT EAT FOOD Total Who Ate Attack Well Food Rate (%) Ill Well Total Who Did Not Eat Attack Relative Confidence Food Rate (%) Risk Interval 3 5 8 38% 2 7 9 22% 1. 7 (0. 4, 7. 7) 2 7 9 22% 3 5 8 38% 0. 6 (0. 1, 2. 3) Tomato 3 6 9 33% 2 6 8 25% 1. 3 (0. 3, 6. 1) Lettuce 3 7 10 30% 2 5 7 29% 1. 1 (0. 2, 4. 7) Sprouts 4 1 5 80% 1 11 12 8% 9. 6 (1. 3, 65. 9)

Evaluate hypothesis – Environmental Health STEP

Environmental Assessment • Essential to investigating outbreaks • Onsite investigations should be done as early in the investigation as possible • Multiple visits may be necessary • *Tool: Environmental Assessment Quick. Train • *Tool : CDC e-Learning on Environmental Assessment • *Tool: Environmental Assessment Quick Reference

Routine Inspection vs. Environmental Assessment Routine Regulatory Inspection Environmental Assessment Focus Common food safety problems Food safety problems related to suspected food during outbreak period Timeframe of Interest Present Past Undertaken Regularly scheduled but often unannounced In response to a specific problem Initiated by Regulatory Agency Outbreak Investigation Team Regulatory Authority State or local environmental health departments State or local public and/or environmental health departments

Preparation for Assessment • Epi will communicate: – Causative or suspect agent – Onset of illness among cases – Likely exposure dates/meals/foods • EH will review: – Existing regulatory records – Menus, recipes, product formulations – Facility disease control policies • Epi and EH together will discuss: – – History of outbreaks at facility Reservoirs and previously identified vehicles Modes of transmission Likely contributing factors
 “When you have a foodborne outbreak, more than one thing")
Investigate Suspected Food Item(s) “When you have a foodborne outbreak, more than one thing went wrong. ”

Contributing Factors • Contamination – Bare-hand contact by ill person – Contaminated raw product • Survival – Time and temperature abuse • Proliferation and Amplification – Time and temperature abuse – Inadequate processing (acidification, fermentation)

Generalizations Causative agent Common contributing factors Spore formers and preformed toxins Cooling, reheating, hot holding, bare- hand contact, room temperature storage, cold holding Viral infections Ill food worker, bare-hand contact, inadequate handwashing, contaminated raw products, contaminated surfaces Bacterial infections Ill food worker, bare-hand contact, inadequate handwashing, contaminated raw product, cross-contamination, inadequate cooking Parasitic infections Contaminated raw products, source, water, cross-contamination, inadequate cooking

Look for Ill Foodhandlers • Interview persons associated with the facility – All levels (dishwasher to owner) – Were they sick too? – *Food handler/manager questionnaire templates: https: //www. colorado. gov/pacific/cdphe/outbreakinvestigation-guidelines • Collect stool from workers (depending on situation)

Collect Documentation • Collect pertinent records – Menus – Invoices and delivery logs – Employee schedules – Employee sick policy – Reservation lists – Complaints received by restaurant – If shellfish is involved, shellfish tags • Take photos, especially of documents you cannot take

Environmental Sampling • We love having positive food tests!!!! • Collect and hold food and environmental samples if available *Environmental Sampling Log However, be aware that: • Food and environmental testing is complicated/expensive • Usually only test when pathogen is known AND there is strong epi evidence implicating a food item

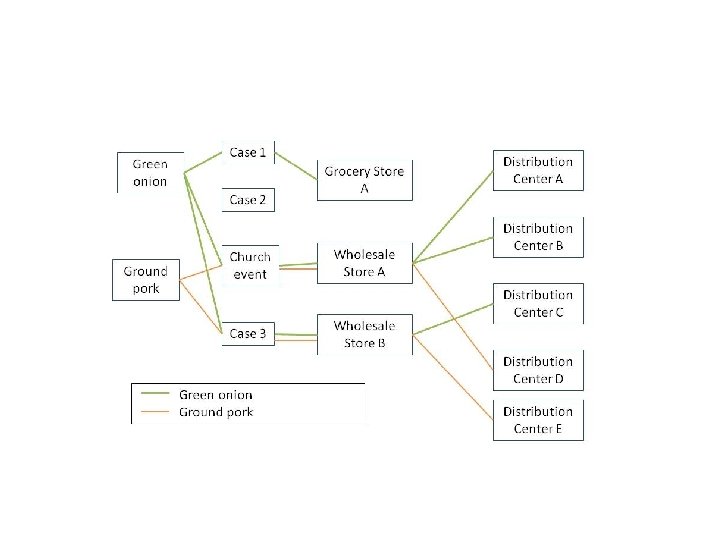
Traceback • Local public health often starts the traceback process • Gathered information may be shared with state health department and FDA/USDA – *Which federal agency had jurisdiction over which foods? http: //www. fda. gov/downloads/ICECI/Inspections/I OM/ucm 127390. pdf

Traceback Diagram created during Listeria outbreak associated with Colorado-grown cantaloupes, 2011

Would you collect food and/or environmental samples for testing in this outbreak? If so, what food item(s)? Would you start traceback activities?

Which EH action would be most crucial at this point? A. Interview foodhandlers B. Conduct traceback C. Collect menus and receipts

Which other EH action would be most crucial at this point? A. Review preparation for all menu items B. Review preparation for suspected items C. Review complaint history for Deli Queen

• An Environmental assessment was conducted at Deli Queen on Wednesday, December 24. • During the Environmental Assessment, you determine that at least one food handler was ill with diarrhea in the beginning of December.
 along with other")
• EH collected produce items (lettuce, sprouts, tomatoes, onions, cucumbers) along with other items that were statistically associated with illness to submit to the State Laboratory for STEC testing; these items are not likely from the same lots served to the ill persons due to product turnover. – The lab only tested the sprouts – They were negative for STEC

TIMELINE: DECEMBER 2014 SUN MON TUE WED THU FRI SAT 1 2 3 4 5 6 Initial STEC case at Deli Queen 7 Frisbee Golf Team ate at Deli Queen 8 2 nd STEC case 9 10 11 12 13 ate at Deli Queen 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 Complaint call Frisbee Golf Team ill 2 nd STEC case report EH Assessment at Deli Queen Initial STEC case report Rita – stool tests positive for STEC

Implement control and prevention measures STEP

Control Measures • Implement as soon as the outbreak is discovered and throughout the course of the investigation • Balance between preventing further disease and protecting credibility/reputation of facility • Guided by evidence from investigation – Do not need to wait for laboratory results – Control measures may change or expand as more is known • *Guidelines for Control of Enteric Pathogens

Examples • Education and Training • Clean and disinfect facility • Exclude from high risk settings and/or duties (food service, health care, childcare) • Tell the public to avoid a food • Cohort ill persons • Temporarily close restaurant, food producer, or facility (or halt new admissions) • Recall food items

Which Control Measures are most important? Choose your top choice. A. Exclude ill foodhandlers B. Test all foodhandlers at Deli Queen for E. coli C. Close the restaurant

Which Control Measures are most important? Choose your top choice. A. Educate all members of Frisbee golf team about E. coli B. Instruct ill persons to not work in sensitive occupations while ill C. Quarantine all members of Frisbee golf team

Communication during and after outbreak STEP

Communication • Effective communication is vital throughout the outbreak investigation • Methods and extent of communication will depend on – Type of outbreak – Size of outbreak – Needs and expectations of your community – Agency policies

Internal Communication • Consider doing daily internal updates early in the investigation – Can be via meetings or update email • Ongoing documentation – Emails – Notes – Timelines – Situation reports • Involve your PIO early in the investigation

External Communication • Notify relevant public health partners – Neighboring counties – State health department – Other stakeholders • Press release may be necessary – Are others at risk of being exposed? – Disease prevention/control measures? • Media may be alerted by affected persons – Be prepared to respond

External Communication • Health Alert Network is often useful to inform health care partners • Other methods: o Letters home to parents (schools, child cares) o Fact sheet to affected individuals o Posting signs/warnings • *Samples of press releases and HANS are on your resource website

Closing an outbreak STEP

When is it over? • Depends on the type of outbreak, transmission route, etiology, etc. • Sometimes 2 incubation periods after the last case’s onset is used as a measure to determine if outbreak is over

Outbreak Debrief / HOT WASH • • • What were our successes? What were our challenges? What can we do better next time? Develop improvement plan based on findings Include internal and external partners who participated in the outbreak investigation.

Outbreak Report • • • Introduction/Background Methods Results Discussion Recommendations Conclusion Acknowledgements Supporting documents *Sample outbreak reports After Action Reports Confidential Information

NORS Form • • National Outbreak Reporting System Timeline for submitting When to complete NORS form Video guidance: https: //www. youtube. com/watch? v=3 Qm. Nc. Pvr. O 3 c • Fillable NORS form http: //www. cdc. gov/nors/pdf/NORS_CDC_5213 -fillable. pdf • *NORS Guidance document

Legal Considerations • Increasingly, outbreaks result in litigation • Outbreak documentation could be subject to the Open Records laws – Emails – Outbreak report – HANS, letters, press releases – Completed questionnaires – Case records – Lab results
 • Ensure confidential information is redacted – Individual cases can")
Legal Considerations (cont. ) • Ensure confidential information is redacted – Individual cases can obtain records about their illness – *Guidance on releasing case information • Consult your agency’s policy

• A case in the outbreak calls you to let you know that he wants to sue the Deli Queen. How would you handle this?

Wrapping Up • Write an outbreak report • *Complete NORS Form

Common Outbreak Pitfalls • Not investigating because the outbreak “occurred too long ago” or “is over” • Questionnaires not filled out completely • Not creating or applying a case definition • Not interviewing well persons • Not collecting specimens for testing (especially human) • Communication

Any questions?

Norovirus 101 Special Thanks to: Amy Woron, Molecular Biologist, TN SPHL Traci De. Salvo, Epidemiologist, WI DOH Brian Collins, Director of Env Health, City of Plano, TX Leslie Barclay, CDC Julia Wolfe, Orange County, CA Michele Samarya-Timm, Somerset County, NJ

Objectives • Learn the basics of norovirus • Epidemiology of norovirus

Have you ever suffered from norovirus? A. YES B. NO C. I don’t know – I’ve blocked those memories

July 2: Two days before the July 4 th holiday…. .

Time to shop for all the July 4 th essentials!

Nausea suddenly takes a nasty turn…. .

What are the typical norovirus symptoms? A. Sneezing, coughing, headache B. Vomiting, diarrhea, nausea, feeling like you are going to die C. Fever, skin rash, body aches D. Fever, headache, stiff neck, nausea, vomiting

Sick and embarrassed, she leaves the store immediately

How far can vomit travel through the air? A. B. C. D. Up to 2 feet Up to 5 feet Over 10 feet Not as far as I can run
 has been or could be exposed?")
Who (and what) has been or could be exposed?

What is the infectious dose of norovirus? A. B. C. D. <20 viral particles 50 -100 viral particles 100 -1000 viral particles > 1000 viral particles

How is norovirus transmitted? A. Fecal-oral transmission B. Vomit-oral transmission C. Consuming contaminated food or water D. Touching surfaces contaminated with vomit or diarrhea and then touching your mouth E. All of the above
 • Virus highly concentrated")
Transmission: Highly Contagious! • Very low infectious dose (<20 particles) • Virus highly concentrated in stool/vomit of infected people – 1 gram of feces contains ~5 billion viral particles • Communicability: – Most contagious while symptomatic – Transmission documented at least 2 days after ill person recovers – People can shed virus for up to four weeks after recovery (possibly longer)

Transmission • Fecal/vomitus oral – Foodborne – Waterborne – Person-to-person – Fomites / environmental contamination – Norovirus can be recovered on surfaces after 3 – 4 weeks at room temperature! • “Airborne” spread – Aerosolized vomitus can travel over 10 feet in the air and settle on environmental surfaces – If you touch these surfaces and then touch your mouth you can be infected

Store Maintenance is called to Clean the Mess

Which of the following is effective at killing norovirus? A. B. C. D. Any type of cleanser Bleach Ammonia Hot water from the tap

Residual Norovirus with Various Cleaning Methods: • 100% of contaminated surfaces still have norovirus after being cleaned with detergent and water • 14% – 28% of contaminated surfaces still have norovirus after applying a 5000 ppm bleach solution for 1 to 5 minutes • 0% of contaminated surfaces have residual norovirus when cleaned with detergent and water, then treated with 5000 ppm bleach solution for 1 minute Source: Barker et al; “Effects of cleaning and disinfection in reducing the spread of Norovirus contamination via environmental surfaces. ” Journal of Hospital Infection 2004 Sep; 58(1): 42 -29

July 3: The July 4 th party is tomorrow…

July 4: Party time!

What is the incubation period for norovirus? A. B. C. D. 6 -12 hours 12 -48 hours 3 -5 days > 7 days

July 5: Uh oh…several guests aren’t feeling so well….

Norovirus Basics • Causes viral gastroenteritis: rarely fatal – Vomiting – Low-grade fever – Headache – Chills • • • – Diarrhea (watery) – Abdominal cramps – Nausea – Malaise and body aches Incubation period: 12 – 48 hours (avg 30) Duration of symptoms: 12 – 60 hours (avg 24) Reservoir: humans Treatment: fluid replacement Immunity: short-lived (viruses evolve)

Testing – human specimens • Norovirus RT-PCR is widely available at commercial labs and is available at most state public health labs. • In outbreak settings, your state lab may cover testing fees or it may be fee-for-service.

Preventing Norovirus Handwashing, handwashing Wash fruits and vegetables thoroughly If you are sick, do not prepare food for others Promptly clean and disinfect surfaces contaminated by feces or vomit • Promptly launder contaminated clothes, towels, linens, etc. • •

Norovirus Resources • Norovirus One Minute Medical School: http: //www. youtube. com/watch? v=HAhu. Df. D 0 L f. Y • CDPHE website: https: //www. colorado. gov/pacific/cdphe/norov irus-and-viral-gastroenteritis • CDC website: http: //www. cdc. gov/norovirus/index. Html • CDC Vital Signs dedicated to norovirus: http: //www. cdc. gov/vitalsigns/

Evaluation Write on index cards.

Overall, how would you rate this training? A. Excellent B. Very Good C. Good D. Fair E. Poor

After this training, I feel better prepared to investigate a foodborne outbreak A. Strongly Agree B. Agree C. Disagree D. Strongly Disagree

Going through an outbreak scenario was beneficial. A. Strongly Agree B. Agree C. Disagree D. Strongly Disagree

I practiced outbreak investigation skills during the training. A. Strongly Agree B. Agree C. Disagree D. Strongly Disagree
 were helpful. A. Strongly Agree B. Agree C. Disagree")
Training materials (slides, handouts, flashdrive) were helpful. A. Strongly Agree B. Agree C. Disagree D. Strongly Disagree

How were the organizational and presentation skills of the instructors? A. Excellent B. Very Good C. Good D. Fair E. Poor

Thank you!
- Slides: 198