Welcome NEW EMPLOYEE TRAINING Monterey County Behavioral Health

Welcome! NEW EMPLOYEE TRAINING Monterey County Behavioral Health 1

Agenda Check-In Welcome Follow-Up New Employee Training Overview Updated Hiring Process Supervisor Expectations v. New Business v. Suicide Assessment Protocol v. Adverse Childhood Experiences 2
 Elsa Jimenez, Director HR Paperwork")
Getting Oriented MC Health Department- 3 hours (First Day) Elsa Jimenez, Director HR Paperwork MC Behavioral Health Bureau 8 hours (w/in 30 Days) Amie Miller, Director Public Behavioral Health; Quality & Risk Management Monterey County (MC)- One Day (Second Thursday) BOS/Lew Bauman, County Administrative Office (CAO) 3 Customer Service; Benefits

Shared Vision of Person Care: Values in Action Guiding Principles Vision • Strength Based Seamless • Trauma Informed Person Looking at MCBH • Fair & Equitable • Person Driven Person. Centered • Culturally Responsive • Community Integrated • Evidence Supported • Solution Focused Strategic 4 MCBH Looking at Person and Natural Supports Person & MCBH: Focus on What Works, Feedback Loop

Personal Vision of Care What Values Guide How You Approach Person Care? Of MCBH’s eight (8) guiding principles, which principle guides you most in your work? Ø Discuss with your table mate and be prepared to share with the group 5

What is Public Behavioral Health? Behavioral Health Mental Health Substance Use Disorder Treatment Wellness/Recovery/Resiliency Focused Public Medi. Cal, Safety Net Population Addresses Health Inequities Specialty Mental Health Services (SMHS) Medical Necessity: Moderate to Severe 6

Medical Necessity Definitions General Definition: “Medical necessity refers to a decision by your health plan that your treatment, test, or procedure is necessary for your health or to treat a diagnosed medical problem. ” California Code of Regulations (Medi-Cal) definition: 1830. 205. Medical Necessity Criteria for Mental Health Plan (MHP) Reimbursement of Specialty Mental Health Services. 1) Diagnosis (Dx) 7 2) Functional (Fx) Impairment
 B. Impairment Criteria: (one")
Medical Necessity Criteria A. Diagnostic Criteria: 1. Included Diagnosis (Dx) B. Impairment Criteria: (one of the following) 1. Impairment 2. Probable Deterioration 3. For Children, Lack of Progress C. Intervention Criteria (all of the following) 1. Addresses Sx/Impairment 2. Expected to (One of the Following) • Diminish Impairment • Prevent Deterioration 8 • Enable Progress
 Califo Depar")
Public Behavioral Health U. S. Health and Human Services Agency (US HHSA) Califo Depar rnia of Hea tment l Servic th Care es ( DHCS CA ) Count y Menta Health l Plan 9

Monterey County Behavioral Health 10
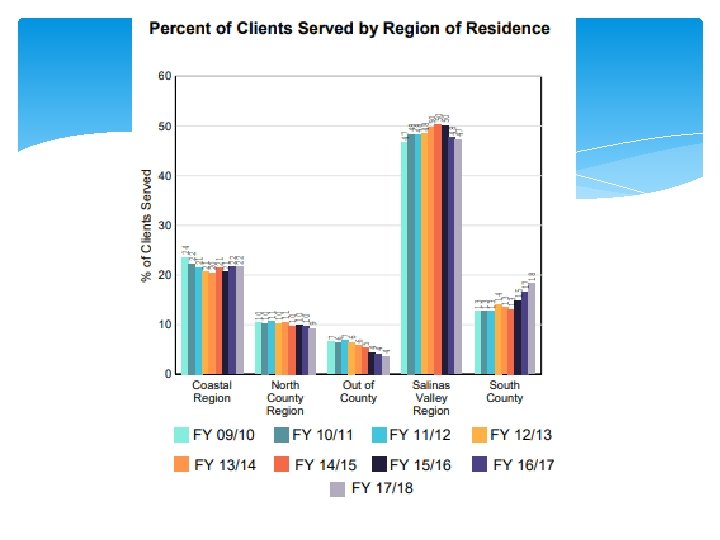
 FY 13/14 Clients Served Total")
Monterey County Behavioral Health Data Driven Decisions (D 3) FY 13/14 Clients Served Total Service Value Avg Spent/Client Avg Age New Clients Discharge Gender (% Male) Language (% English) FY 15/16 FY 16/17 FY 17/18 7778 8529 10482 $56. 2 M $63 M* $83 M $7. 2 K $7. 4 K $8. 0 K 28 28 28 3164 4112 4780 3958 5063 5946 53% 52% 51% 11960 $82 M $6. 9 K 28 4701 6386 50% 12688 $89 M $7. 0 K 29 4664 6664 50% 80% 78% FY 14/15 80% *FY 14/15 Disallowance Rate = 59. 4%

Equity v Equality 14

15

Organizational Chart Systems of Care/Programs ACCESS Adult Children’s Medical Administration Finance Management Analysts Quality Improvement Training 16
 Social Worker III Psychiatric Social Worker")
Job Classifications Direct Service Behavioral Health Aid (BHA) Social Worker III Psychiatric Social Worker I, II, Senior Psychologist Psychiatrist, Medical Assistant, Nurse Clinical Support Patient Services Representative Unit Supervisor Administration Administrative Line Staff Program Manager; Finance Manager; Management 17 Analyst
) Social")
Examples of Collaborative Partners Monterey County Departments Health (Policy, Evaluation & Planning (PEP)) Social Services, Probation, Sheriff Contract Providers CSOC: Kinship Center, Rancho Cielo ASOC: Interim; Drake House; SUD: Sun Street All: Community Human Services (CHS) Community Partners Schools Homeless Coalition 18

Quality Management: Overview of Quality Assurance & Clinical Oversight
/Compliance Outcomes/Performance Management Clinical Oversight/Training Electronic Health Records Services")
Quality Improvement Programs/Functions Quality Assurance (“QA”)/Compliance Outcomes/Performance Management Clinical Oversight/Training Electronic Health Records Services
 755 – 4545 Technical")
QI Resources QI Website: Help. Line: www. mtyhd. org/QI (831) 755 – 4545 Technical Assistance and Question: 415 QA@co. monterey. ca. us Clinical Questions: 415 QI@co. monterey. ca. us QI Newsletter Training Academy: My. Learning. Pointe Quality Improvement Committee (QIC) Quarterly

MCBH Compliance Plan Who: Staff, Volunteers, Trainees, and Contractors Where: County-Owned, Operated, or Contracted Sites. What: Support Integrity of All Health Data Submissions: Accuracy, Reliability, Validity, Timeliness Comply Statutory, Regulatory, Contractual Reqs Why: Ensure Excellence in Client Care Prevent Fraud and Abuse At All Levels When: Always How: QI Functions, Policies & Procedures: Quality Assurance, Utilization Review,

Scope of Practice Defined by State Statutes, Regulations, and Laws MCBH Does Not Authorize Providers to Work Outside their Own Scope of Practice Some classifications require a co-signature from a clinical supervisor as a supervision tool. This does not allow practice beyond a particular provider’s scope of practice The California Department of Health Care Services – Mental Health Division (“DHCS – Mental Health”) has specified that a co-signature does not enable someone to provide services beyond his/her scope of practice.

Sustainability Set Standard for All MC BH Clinical Staff: No Less Than Seventy Five Percent (75%). Minimum of 75% of work hours must be spent on tasks and services that are considered “billable” Other indirect service codes are also factored in to the Sustainability report (i. e. vacation time, QI time, etc. ). Revenue generating activities are an important source of income for our agency. This and other source of income allows our agency to offer a broad range of services to our clients.

Case Coordination MCBH uses a Case Coordination Model Each Client Assigned “Case Coordinator” Responsible for: Coordinating services Ensuring that services are medically necessary Completing the required beneficiary assessment and reassessment Approving components of and completing beneficiary Treatment Plan A Case Coordinator Must Be Either: Licensed/license-eligible/waivered staff, MCBH staff psychiatrist MCBH approved community provider staff

Informed Consent = Informed Decision Making Accommodate differences in client preferences Encourage shared decision making Discuss range of services provided, especially risks, benefits & alternatives (r, b, &a). Onset of Services, which includes Informed Consent, is only completed one time in life of client as long as client not closed longer than 365 days. Consent for Treatment no longer needed every year.

Confidentiality Individual’s have a right to confidentiality and we have a legal and ethical obligation to uphold confidentiality. Confidentiality of health records is protected by State and Federal statutes and regulations. Protected health information (“PHI”) requires consent from the client in order to use, disclose, or exchange except for specific situations indicated by law. Only staff directly involved in treatment may access the health record (it is illegal to access an individual’s health record without their prior authorization). It is never okay for staff to access records to satisfy their own curiosity. Avatar stores information on who accessed the

Confidentiality of Substance Abuse Records Substance Abuse records are held to a higher confidentiality standard than pure mental health record The law defines substance abuse providers as any one who provides substantive substance abuse treatment This includes mental health providers who provide dual diagnosis treatment Who exactly is a substance abuse provider? Due to the confusing status of our providers we ask clients to complete the Authorization to Use, Exchange, and/or Disclose PHI WITHIN

Authorization to Use, Exchange, and/or Disclose Protected Health Information Use the “Authorization to Use, Exchange, and/or Disclosure of Confidential Behavioral Health Information” form The Authorization, once signed, may be valid for a specified amount of time or up to a certain event The form must state who the information may be released to; the purpose the information may be used; what specific information may be released An authorization can be revoked at any time. The revocation can be verbal and does not have to be in writing MH: You can designate role (my Parole Officer).

Breach of Confidentiality On RARE occasions, we disclose information without authorization in situations that are not permissible by law. Even if it is a mistake, the law says it has to be investigated internally and reported to both the State and the Feds If you believe you breached a client’s PHI, contact your supervisor and QI immediately Complete Unusual Incident Report QI is required to report to the State about any possible breach within 72 hours If you accessed a client’s record in error (i. e. transposed numbers). In AVATAR use the “Accidental/Incorrect Client

Client-Care & Medical Necessity

72 -Business Hours Documentation Timeline The absolute standard is to document services no later than 72 business hours after the service. When a service is recorded, practitioners can claim both the time it takes to provide the service and the time it takes to write the note. It is understandable that there will be times when the documentation of the service provided cannot be entered within the expected time frames. When this happens, a “late entry due to” should be included at the top of the progress note body. This entry is a very brief reason for the late entry. State guidelines recommend the 72 -hour timeline for accuracy of information based on our ability to recall information. Chart closed immediately after client dies.

Self Care It Is Absolutely Imperative To Take The Time To Care For Yourself As A Monterey County Behavioral Health Staff Member, You Are A Very Important Part Of The Individual/ Family’s Recovery Process You Are Helping To Change Client Perspectives Of Themselves

Professional Development 34

New Employee Training Schedule mylearningpoint. org NET Welcome to Public Behavioral Health Today NET Quality & Risk Management Today Core Cultural Competence TBD Core Non Violent Crisis Intervention June 19; 8/20/19 Core Clinical Progress Note Writing June 25 Core Clinical Assessment July 17 Core Clinical Treatment Plan Writing May 7; Aug 8 Core Clinical my. AVATAR -Electronic Med Records 35 May 17; June 21

Professionalism Time Arrive on Time to Meetings; Text if Late Request Time Off In Advance Technology (e. g. , Phones, Tablets, Laptops) Meetings: Out Of Sight Unless Note taking Togs (Clothing/Dress Code) Always Neat, Clean, Appropriate Coverage Program Appropriate Civility 36

Clinical Training Components Shared Vision Core Competencies Program Specific Interventions Leadership Academy 37
 Individual Development Plan Core")
Training Policies and Procedures Tools m. LP (my. Learning. Pointe) Individual Development Plan Core Competencies Assessment Tool Continuing Education Disciplines: BBS; Psychologist Philosophy Content > Important than CEUs Attend In Full To Receive Units Sustainability Back Out for Many Trainings 38

Shared Vision of Person Care: Values in Action Guiding Principles Vision • Strength Based Seamless • Trauma Informed Person Looking at MCBH • Fair & Equitable • Person Driven Person. Centered • Culturally Responsive • Community Integrated • Evidence Supported • Outcome Focused Strategic 39 MCBH Looking at Person and Natural Supports Person & MCBH: Focus on What Works, Feedback Loop

Core Competencies • Five Key Areas • Bureau Wide/General • Professionalism • Diversity & Inclusion • Clinical/Technical • Client Care • Clinical Conceptualization • Documentation • Core Competencies Assessment Tool 40

Program Specific Interventions Evidence Supported Practice Evidence Based Practice Based Evidence/Promising Practices Community Define Interventions Motivational Interviewing (Core Competency) Cognitive Behavioral Interventions Seeking Safety 41

Leadership Academy • Goal • Support Professional Development, • Client Services • For All Clinical • Program Managers • Supervisors • On-Going, Once per Month for 2 hours 42

Risk & Safety Management Emma Orellana, LCSW Behavioral Health Unit Supervisor AB 109 & Mobile Crisis Unit orellana. EN@co. Monterey. ca. us 831 -796 -1240

Overview o Clinical Programs o Forensic teams o Crisis teams o Specialty Teams & Training Programs o Mindset of Safety o Crisis Developmental Model (CPI) o Decision-Making Matrix o Working with a team o Understanding Risk & Your Responsibilities o 5150, APS, CPS, Tarasoff o Incident Reports o Documentation o Resources
 Drug Treatment Court (DTC) DUI")
Forensic Teams Therapeutic Justice Courts MH Treatment Court (CNC) Drug Treatment Court (DTC) DUI Treatment Court VTC & Military Diversion Misdemeanor Competency Restoration AB 109 Post Release Community Supervision High Risk Felony Probationers

Crisis Teams Emergency Department Access Team Crisis team based out of NMC ED 24/7 Mobile Crisis Team Wednesday-Saturday 12: 30 pm-10: 00 pm Alternating Tuesdays 1: 30 pm-10: 00 pm

Mobile Crisis Team • Active in Monterey County since November 2015 • 3 Mobile Crisis Intervention Specialists (MCIS) • 1 for each region • Based out of Monterey PD, Greenfield PD and Salinas • MCIS respond to calls for service that come thru dispatch with LE • MCIS also to do non-emergency follow-up in the field • Available to support / not replace the efforts of
 242 -0508 Peninsula")
Mobile Crisis Team Salinas / North County Region Michele O'Brien (831) 242 -0508 Peninsula Region Ryan Speed (831) 242 -0509 South County Region Maria Guerrero (831) 242 -0507 Important: These numbers are for staff use only, only do not give to the public. Clients & families should be given: 1 -888 -2586029
 Crisis Intervention")
Specialty Teams & Training Crisis Negotiation Team Critical Incident Stress Management (CISM) Crisis Intervention Team & Training (CIT) Mental Health First Aid for Public Safety

Mindset of Safety What’s that mean to you? How can you incorporate that into your work?
 Established in 1980 in Brookfield, WI Training for Human Services")
Crisis Prevention Institute (CPI) Established in 1980 in Brookfield, WI Training for Human Services Professionals & Educators More the 6 million people trained worldwide Goal = to provide for the Care, Welfare, Safety & Security for everyone involved in a crisis situation CPI Non-Violent Crisis Intervention Training Program
 Developed the Non-Violent Crisis Intervention Training program Purpose = Recognize")
Crisis Prevention Institute (CPI) Developed the Non-Violent Crisis Intervention Training program Purpose = Recognize Warnings Signs Intervene Effectively Maintain Safety What to do before, during and after a crisis Balances the practical applications & humanistic concerns CPI Non-Violent Crisis Intervention Training Program

Crisis Development Model The key to deescalating a crisis situation is recognizing warning signs and intervening as early as possible Behavioral Levels Anxiety Defensive Risk Behavior Tension Reduction Staff Attitude/Response Supportive Directive Disengagement skills Therapeutic Rapport Integrated Experience - looks at the interdependence of these things… CPI Non-Violent Crisis Intervention Training Program

CPI Non-Violent Crisis Intervention Training Program

More About Risk & OUR RESPONSIBILITIES!

Do you have a responsibility if… A client is a danger to themselves or others? A client is decompensating and unable to care for themselves in a safe manner?

Yes… Welfare and Institutions Code Section 5150

W&I 5150 A 5150 is a legal hold imposed on a person that is believed to be in need of involuntary psychiatric treatment in the State of California. The person is believed to be a combination of 1 or more of the following: A Danger to Self A Danger to Others Gravely Disabled Due to a mental health disorder

W&I 5150 – who can initiate a hold? Mental health professionals approved by the county behavioral health director after completing training and passing a test Selected members of attending staff at evaluation facilities/hospitals that are designated for involuntary detainment by the county Peace Officers, including Sheriffs, State Park Rangers, State University Peace Officers.

Do you have a responsibility if… You have knowledge a child is possibly being abused or neglected? You become aware a dependent or older adult is being abused or neglected?

Yes… You are a mandated reporter Form SS 8572 Consult with your supervisor File report with Child Protective Services (CPS) Be sure to document appropriately

Yes… You are a mandated reporter Form SOC 341 Consult with your supervisor File report with Adult Protective Services (APS) Be sure to document appropriately

Do you have a responsibility if… You become aware a client is making threats to harm another person, a group, or target a location?

Yes… Based on Tarasoff v Regents of the University of California, CA Supreme Court decision, 1976 Policy & Procedure 306 “[w]hen a therapist determines, or pursuant to the standards of his profession should determine, that his patient presents a serious danger of violence to another, he incurs an obligation to use reasonable care to protect the intended victim against such danger. ”
 in the")
Continued… If a threat is made to harm a reasonably identifiable victim(s) in the designated individual’s presence, they must notify the person(s) threatened and call law enforcement to report the threat. (Tarasoff) Communications from family members made to advance the patient’s therapy are considered patient communications (Ewing) Credible threats from family/reliable 3 rd parties trigger duty to protect (Ewing) Ewing v Goldstein (2004) Ewing I & Ewing v Northridge Hospital (2004) Ewing II

Documentation It’s important always, but even more so in high risk situations Why? Incidents Reports Policy & Procedure 123

Some things you can do Ø QI website is a great resource Ø Clinical documentation guide Ø Policies & Procedures Ø Develop a Mindset of Safety Ø Intervene in teams in crisis situations Ø Consult, consult & use your team as the invaluable resource it is Ø Ongoing Training Ø Attend Non-Violent Crisis Intervention training annually Ø Attend 5150 certification training (if your position calls for that & get your authorization card) first, then attend Practical Aspects of 5150 Situations training

Monterey County Resources

Monterey County Behavioral Health Salinas Adult Services: 1441 Constitution Blvd. , bldg. 400 suite 202, Salinas (831) 796 -1700 or Access (all ages) for assessment (888) 258 -6029 Marina Clinic: 299 12 th Street, Marina, (831) 647 -7652 Soledad Clinic: 359 Gabilan Drive, Soledad, (831) 678 -5125 King City Clinic: 200 Broadway Street, suite 70, King City, (831) 386 -6868 Children’s BH Main Clinic: 951 B Blanco Circle, Salinas (831) 784 -2150 Children’s BH Clinic: 1000 South Main #210 B, Salinas (831) 796 -1500 Website: www. mtyhd. org
 663 -5433")
Mental Health Crisis Intervention 24/7 Suicide Prevention of the Central Coast (877) 663 -5433 Toll Free National Suicide Prevention Lifeline (800) 784 -2433 or (800) 273 -8255 Veterans Crisis Line (Nation-wide) (800) 273 -TALK (press 1) Natividad Medical Center ED Access (831) 755 -4111 (ask for crisis team)

Other Mental Health Resources CHOMP Outpatient Behavioral Health: 576 Hartnell Street, Monterey 831 -625 -4600 Website: www. chomp. org Interim, Inc. MCHOME (homeless outreach) 831 -883 -3030 National Alliance on Mental Illness (NAMI) Website: www. namimonterey. org 831 -375 -6264 (Monterey); 831 -402 -4940 (Salinas) PREP: 909 A Blanco Circle, Salinas Website: www. prepwellness. org 831 -4245033

SAM’S GUIDE to Monterey County Resources http: //mcdss. co. monterey. ca. us/docs/SAMs_01_2017. pdf

Monterey County Guide to Homeless Services http: //mcdss. co. monterey. ca. us/cap/download/2017%20 MC%20 HSRG. pdf

What questions do you have?

Next Steps Review Individualized Development Plan w/ Supv Documentation Universal Psychosocial Assessment Person Centered Treatment Planning my. Avatar Risk & Safety Management Non-Violent Crisis Intervention (CPI) Involuntary Hold Training (5150/5585) Cultural Competence 75
- Slides: 75