Welcome EMR EHR PHR CCR WHAT n Electronic














































- Slides: 48
Welcome
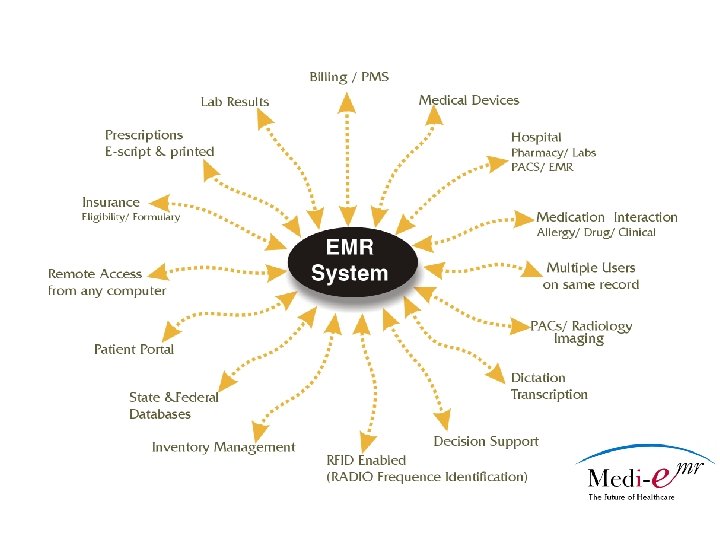
EMR , EHR, PHR, CCR… WHAT? ? n Electronic Medical Record n n Electronic health record n n Refers to the entire Medical System and Interface. Personal Health Record n n Electronic record with full interoperability within an enterprise (hospital, clinic, practice) A medical record held or accessed by the patient. Continuity of Care Record n The standard is a comprehensive clinical content standard including patient demographics, encounters, diagnoses, medications, allergies and immunizations
Why implement an EMR n n n Produce readable records Eliminate Chart Hunting Equivalent of one FTE for most practices Allow access at multiple office locations Eliminate transcription fees Provide coding compliance Open another patient exam room Possibly reduce malpractice premiums Provide offsite accessibility for on call staff/Drs Qualify for ARRA Funds Qualify for CMS Bonus payments
Advantages of EMR n n n Everything comes to the point of care. The chart becomes a dynamic tool beyond just a record of patient encounters. The data becomes n Legible n Easy to retrieve n Searchable n Reportable and measurable
Advantages of EMR n Coding and billing can be combined with clinical documentation to more efficiently capture the information with faster turn around time for reimbursement. n Additional software can manage all communication with the patient, including phone calls and patient portal. n Insurance formularies combined with eligibility checking equals more revenue.
Advantages of EMR n No more chart misplacement. n Data can be accessed from anywhere with internet access. n Prescription information becomes more manageable. n Multiple staff may access a record but not everyone can make changes to it. n Access to information can be determined by job function.
Is it time for your practice? n n n Do you have more than one office? Are you starting a new practice or opening a new office? Have you run out of space for charts? Do you spend too much time spent searching for charts? Have you been concerned about the need for readable charts - for legal or practical reasons? Do you carry your charts in a suitcase with wheels?
When you are ready to consider EMR n n n Form an EMR committee - include Dr, medical assistants/PA’s, billing staff, front desk staff Document all current office practices and rational Evaluate each process for inclusion in the EMR Make a wish list of needs for your practice by department Involve staff – prepare them for change Determine whether a full overhaul or a phased in transition is best for your office
Practice Assessment n Document your practice profile n Single Specialty/Multi Specialty n Number of office locations n Number of Physicians, Nurses, Technicians n Number of front office, back office, and administrative staff and job functions? n Estimated number of medical records? n Number of active patients? n Number and names of the lab(s) the practice uses n Number and names of hospitals the practice uses n Any medical devices
Practice Assessment n Document your practice profile n Single Specialty/Multi Specialty n Number of office locations n Number of Physicians, Nurses, Technicians n Number of front office, back office, and administrative staff and job functions? n Estimated number of medical records? n Number of active patients? n Number and names of the lab(s) the practice uses n Number and names of hospitals the practice uses
EMR Essential Characteristics n Data entry must be easy n Clinical data entry should be similar to current formats n The well designed EMR should enhance patient flow n Whenever possible processes should be automated through electronic interfaces
EMR Essential Characteristics n Ability to modify previously entered data with audit trails to identify the revisions n Search access should be fast, efficient and accurate n Ideal EMR interfaces with ANY practice management system
EMR Essential Characteristics n Patient education tools can be integrated and services reportable for more measurable results n Documentation can be enhanced for accurate billing of all services provided n Reporting capabilities can be improved for better utilization review and clinical profiles
The Search n Ask if the Practice Management System can interface with an EMR n Pro’s – don’t have to implement a new cash flow system and workflow system. n Con’s – ‘interfacing’ can put your practice in a position of interacting with two vendors with two different agendas, fees, etc
Ask n n n Does Your EMR have a 2 -way HL 7 interface? What is the infrastructure Microsoft, Oracle or IBM db 2? Does it interface with our existing PMS? What is the disaster recovery plan? How many modules are there? Are the formats customizable?
Types of EMRs
ASP = Application Service provider n Internet based n Data located off site n Should be available form anywhere n Access thru login only
ASP PROS n n n n n Available from any internet connection No onsite servers No backup required No hardware maintenance No onsite data center No software to install No software to maintain No software upgrade to install Real time updates
ASP CONS n n Must have internet to access patient chart Data not in your hands May have slower access Usually no software ownership
CLINET SERVER n n Office based Data located on site May or may not be available form anywhere May operate faster
Client Server PROS n n n May have access via web No reliance on internet All data is onsite
CLIENT SERVER CONS n n n n n Available from any internet connection onsite servers required Backup required Hardware maintenance Onsite data center Software to install Software to maintain Software upgrade to install Updates with next Release
Starting The Process
When you are ready to consider EMR n n n Form an EMR committee - include Dr, medical assistants/PA’s, billing staff, front desk staff Document all current office practices and rational if needed Evaluate each process for inclusion in the EMR Make a wish list of needs for your practice by department Involve staff – prepare them for change Determine whether a full overhaul or a phased in transition is best for your office
Selection process n Ideally review 3 to 5 different products with demonstration documentation by each company n Then narrow down to top 2 or 3 for onsite demo’s n Ask for recommendations or trial period.
Practice Assessment n Document your practice profile n Single Specialty/Multi Specialty n Number of office locations n Number of Physicians, Nurses, Technicians n Number of front office, back office, and administrative staff and job functions? n Estimated number of medical records? n Number of active patients? n Number and names of the lab(s) the practice uses n Number and names of hospitals the practice uses
EMR Essential Characteristics n Ask if the Practice Management System can interface with an EMR n Pro’s – don’t have to implement a new cash flow system and workflow system. n Con’s – ‘interfacing’ can put your practice in a position of interacting with two vendors with two different agendas, fees, etc
Ask n n n n Does Your EMR have a 2 -way HL 7 interface? What other interface type are available? What is the database infrastructure Microsoft, Oracle or IBM db 2? What operating system does it run on? Does it interface with our existing PMS? What is the disaster recovery plan? How many modules are there? Are the formats customizable?
EMR Essential Characteristics n Data entry must be easy n Clinical data entry should be similar to current formats n The well designed EMR should enhance patient flow n Whenever possible processes should be automated through electronic interfaces
EMR Essential Characteristics n Patient education tools can be integrated and services reportable for more measurable results n Documentation can be enhanced for accurate billing of all services provided n Reporting capabilities can be improved for better utilization review and clinical profiles n Ability to modify previously entered data with audit trails to identify the revisions
Attributes of EMRs for Physician Practices n Physician and practice workforce must be an integral part of identifying practice workflows, processes, and action triggers, and of specifying business requirements that will underpin the EHR n The EMR must integrate administrative and clinical business requirements
Possible Components n n n n Patient Demographics Insurance eligibility checking. E-prescribe with clinical and interaction check. Electronic Medical Records Scheduling Billing-electronic or drop to paper Sales & Inventory Custom Reporting
Incentives
HITECH Act On February 17 th, President Obama signed the 2009 American Recovery and Reinvestment Act, allocating $19. 2 billion for health information technology. The provision of the legislation known as the HITECH Act will be distributed as follows: $17. 2 billion incentive payments for EHR use. $2 billion is available for grants and loans for health information technology advancement. When coupled with existing measures, these funds represent significant income opportunities for existing EHR users and to assist new users with adoption related costs.
HITECH Act
CMS Incentives n 2 ½ % bonus payment for E-prescribing. n 2 ½ % bonus for PQRI reporting.
Other Incentives n n n Malpractice reduction. 5%-15% Reduction for using robust EMR Technology Grants Lab subsidies Billing Company subsidies Radiology Center Subsidies Hospital Subsidies.
The Installation
Key points of EMR selection n n Be very clear about practice objectives in implementation Assign an individual to work with EMR vendor on customization who: n understands and embraces the technology n has time in their schedule to work w/vendor Set realistic timelines of implementation Keep staff updated on project/timeline Allay staff fear of losing jobs- ask staff to identify other tasks getting least attention currently
Transition Considerations n n Big Bang n On one day, pull the switch and everything goes electronic Modular n Adopt one module at a time (e. g. . e. Prescribing), then transcription, then interfaces with Practice Management System, Lab, Hospital, Pharmacy …
Build Detailed Timeline n n n n Project Team and Plan Communication w/ vendors & staff Map Critical Practice Workflows (where are current bottlenecks) and remap with EMR Plan for Existing Data Training System Testing Contingency Planning Go-Live Planning
Transition Considerations n Big Bang n n n More disruptive on front end, less on back end Full team commitment More difficult to measure ROI Best for new practices Modular n n Less disruptive Slower to experience full benefit Adaptable to resistant physicians Easier to measure ROI
Wrap up n n It is not a matter of “if”, it’s a matter of when n Exception: retiring from practice in next 5 years CMS encouraging practices to move to EMR
Questions and Answers
Thank You Now The Demonstration