WELCOME COMPASSIONATE COMMUNITIES Making Death Dying and Bereavement

WELCOME COMPASSIONATE COMMUNITIES Making Death, Dying and Bereavement Everyone’s Business

Alison Bunce Programme Lead alison. bunce@ardhosp. co. uk

Public Health Approach to Palliative Care Making death, dying and bereavement everyone’s business (Kellehear, 2005)

Death and Dying is: • a normal part of life • more than a medical responsibility • a Public Health and Societal Issue • a responsibility of a ‘compassionate community’ (Pugh and Aungiers, 2015)

Inspiration Professor Allan Kellehear Compassionate Communities Conference Interested people / Partnership working

Policy Direction Communities of all kinds are empowered to provide effective support to those dealing with death, dying, bereavement and loss. (2011) Communities are stronger, responsible and more able to identify, articulate and take action on their needs and aspirations to bring about an improvement in the quality of community life. (2013) People know how to help and support each other at times of increased health need and in bereavement, recognising the importance of families and communities working alongside formal services. (2016)

“ A Compassionate community is a community where everybody recognises that We all have a role to play in supporting each other in times of crisis and loss. People are ready, willing and confident to have conversations about living and dying well and to support each other in an emotional and practical ways” (2016)

Role of palliative care

Compassionate Communities

Local Initiative, Part of a Global Social Movement


Compassionate Inverclyde What it is not • Social Movement • A service • Involves ordinary people • About health professionals • Community development • A palliative care service • Needs based evolution, with • Prescriptive no blue print development

Public Engagement

")
Building Community Capacity • Improving well being • Compassionate citizens (No One Dies Alone) • Work with schools / Annual public event (to absentfriends) • Compassionate Organisations

Improving Wellbeing

No One Dies Alone Compassionate Companions

To Absent Friends

Initiatives with schools
 • Formation of a")
Progress so Far • Initial Public engagement (over 200 people) • Formation of a Compassionate Inverclyde Board and external support network • 4 Pilot Groups: Improving Wellbeing Programmes which will be known as HIGH 5 • 1 st pilot Bereavement Café at Branchton Community Centre • 1 st working group meeting for No One Dies Alone Programme at IRH • 1 st community ‘toabsentfriends’ event 7 organisations took part • 1 st meeting with Education about working with young people and parents


Current Partnerships • West College Scotland, Lecturer Emma Maxwell is taking forward the High 5 Programme currently running 2 nd public group at Branchton Community centre. • Branchton Community Centre. Manager Willie Wilson providing accommodation and beverages free of charge for Bereavement Café and High 5 group. • Your Voice, Staff have helped facilitate public engagement and developed the film for the Launch event. • Inverclyde Council dedicated a tree for the absent friends event in the Well Park. • Inverclyde Royal Hospital, pilot of the No One Dies Alone programme. • Initial discussions with colleagues in Seville.

Vision for Inverclyde as a Compassionate Community Every person in Inverclyde will take part in a ‘toabsentfriends event’ Gp’s and Primary care teams know how to make a request for support Art gallery, museum and Beacon Arts center will showcase Art/drama work 100% of churches will have an end of life care group Compassionate Inverclyde Every community centre in Inverclyde will have a bereavement cafe Every community centre will have a resource bank of Compassionate Citizens At least 50% of people in Inverclyde will die in their place of choice 100% of people in IRH will not die alone if that is their wish 100% of organisations in Inverclyde will have a bereavement policy in place Every school in Inverclyde will run the wellbeing programme

Evaluation: What does success look like? 2017 Compassionate Communities Symposium at ICC Sydney https: //www. youtube. com/watch? v=ZGwr. LRy. BIR 0 • Building healthy public policy • Creating supportive environments • Strengthening community action • Developing personal skills • Reorienting health care services toward prevention of illness and promotion of health

Compassionate = Acts of Kindness Helpful = Say YES to help Neighbourly = Ordinary people

Learning from Australia: A Call to Action • As an Individual • As a Community • As an Organisation

Important Facts • We are all in it together • Now in a period of radical change • We need to think about Network Focussed Care • Active Hope • This is the start of a Social Movement • Death Literacy

Integration Perspective

Integration health & social care • • • Joint Future LHCP CHP HSCP Integrated Joint Boards The Public Bodies (Joint Working) (Scotland) Act 2014 • Reflect how far we have come from the debate over a medical and social bath and how far we need to travel until we reach optimum level of integration.
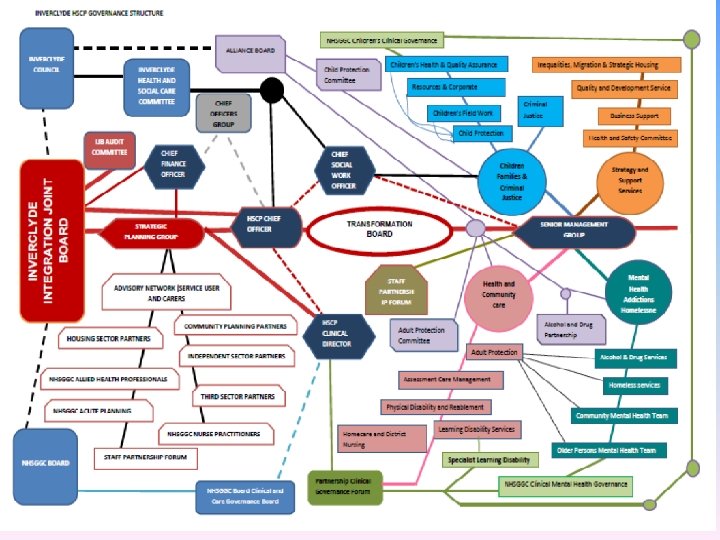

Inverclyde HSCP Governance Structure Blue - Parent Bodies and reporting structures Lilac - Inverclyde Alliance Board and sub-committees Green - NHSGGC Clinical and Care Governance – and three specialist sub-groups Dark Blue - HSCP NHSGGC and Inverclyde Council advising or Chief Officers Blue - Parent Bodies and reporting structures Grey - National HSCP Chief Officer and Chief Financial Officers Groups Lilac - Inverclyde Alliance Board and sub-committees Green - NHSGGC Clinical and Care Governance – and three specialist sub-groups Brown - Staff partnership Forum Dark Blue - HSCP NHSGGC and Inverclyde Council advising or Chief Officers Grey - National HSCP Chief Officer and Chief Financial Officers Groups Pink - Health and Community Care and linked Teams Brown - Staff partnership Forum Pink - Health and Community Care and linked Teams Light Blue - Children, Families and Criminal Justice and linked Teams Teal - Mental Health Addictions and Homelessness and Linked Teams Orange - Strategy and Support Services and Linked Teams Broken Red line ----- Delegated Responsibility and Advisory Functions which feed into the HSCP Orange - Strategy and Support Services and Linked Teams Broken Black line ---- Reporting links to Parent Bodies Broken Blue line --- Reporting lines of Clinical Director to NHSGGC Board Clinical and Care Governance Broken Red line ----- Delegated Responsibility and Advisory Functions which feed into the HSCP Thick Red oval shape –Inverclyde HSCP Transformation Board Red outline and white background shape - Representative membership of the Strategic Planning Group Broken Black line ---- Reporting links to Parent Bodies Full red colour shapes - Integration Joint Board , Audit Sub-committee and Strategic Planning Group Broken Blue line --- Reporting lines of Clinical Director to NHSGGC Board Clinical and Care Governance Thick Red oval shape –Inverclyde HSCP Transformation Board Red outline and white background shape - Representative membership of the Strategic Planning Group Full red colour shapes - Integration Joint Board , Audit Sub-committee and Strategic Planning Group

Integration health and social care • • National Health and Wellbeing Outcomes Integration Planning and Delivery Principles Core Suite of Integration Indicators Clinical and Care Governance Framework Strategic Commissioning Plans Financial Assurance Localities

Integration delivery principles • Evidence how services are planned and delivered in a person centred way; • Demonstrate how integrated services are developed for the benefit of service users
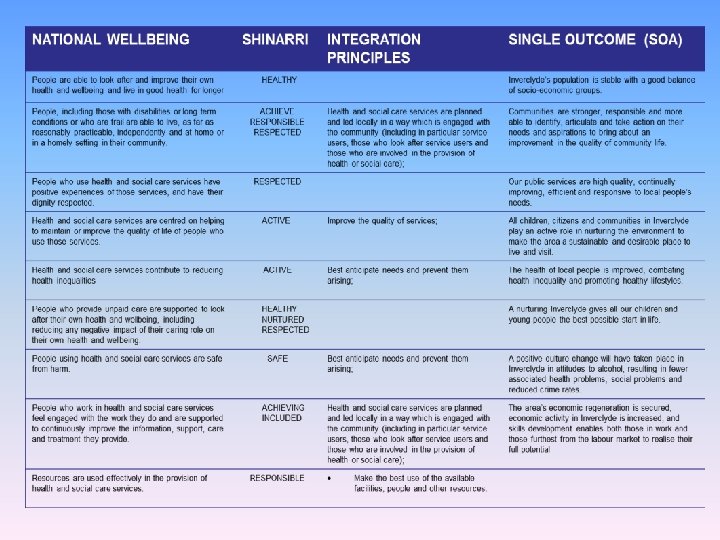

NATIONAL WELLBEING OUTCOMES SHINARRI People are able to look after and improve their own health and wellbeing and live in good health for longer HEALTHY People, including those with disabilities or long term conditions or who are frail are able to live, as far as reasonably practicable, independently and at home or in a homely setting in their community. ACHIEVE RESPONSIBLE RESPECTED People who use health and social care services have positive experiences of those services, and have their dignity respected. INTEGRATION PRINCIPLES SINGLE OUTCOME AGREEMENT (SOA) Inverclyde’s population is stable with a good balance of socio-economic groups. Health and social care services are planned and led locally in a way which is engaged with the community (including in particular service users, those who look after service users and those who are involved in the provision of health or social care); RESPECTED Communities are stronger, responsible and more able to identify, articulate and take action on their needs and aspirations to bring about an improvement in the quality of community life. Our public services are high quality, continually improving, efficient and responsive to local people’s needs. Health and social care services are centred on helping to maintain or improve the quality of life of people who use those services. ACTIVE Improve the quality of services; All children, citizens and communities in Inverclyde play an active role in nurturing the environment to make the area a sustainable and desirable place to live and visit. Health and social care services contribute to reducing health inequalities ACTIVE Best anticipate needs and prevent them arising; The health of local people is improved, combating health inequality and promoting healthy lifestyles. People who provide unpaid care supported to look after their own health and wellbeing, including reducing any negative impact of their caring role on their own health and wellbeing. HEALTHY NURTURED RESPECTED People using health and social care services are safe from harm. SAFE People who work in health and social care services feel engaged with the work they do and are supported to continuously improve the information, support, care and treatment they provide. ACHIEVING INCLUDED Resources are used effectively in the provision of health and social care services. RESPONSIBLE A nurturing Inverclyde gives all our children and young people the best possible start in life. Best anticipate needs and prevent them arising; A positive culture change will have taken place in Inverclyde in attitudes to alcohol, resulting in fewer associated health problems, social problems and reduced crime rates. Health and social care services are planned and led locally in a way which is engaged with the community (including in particular service users, those who look after service users and those who are involved in the provision of health or social care); The area’s economic regeneration is secured, economic activity in Inverclyde is increased, and skills development enables both those in work and those furthest from the labour market to realise their full potential Make the best use of the available facilities, people and other resources.

Integration health and social care • National Wellbeing Outcomes – How the 9 outcomes are ‘improving lives’ through the delivery of service • Commissioning • Partnership Working – How has the service worked in collaboration with partners and stakeholders? • Strategic Planning & IJB – Localities Planning and Cluster Working • Financial Performance • Best Value & Inspection of Services

Strategic Alliance • • • Inverclyde council – Elected members Skills Development Scotland West College Scotland Scottish Fire & Rescue Service Scottish Natural Heritage Scottish Enterprise 3 rd Sector Interface Department of Works and Pensions River Clyde Homes – Registered social Landlords Police Scotland Strathclyde Partnership for Transport Community Council Forum • • • In attendance: Chief Executive Inverclyde council Chief Officer Inverclyde HSCP

Integration health and social care Integration principles Community planning Building capacity Inclusiveness of Inverclyde community • Choice and control • • – Individual is focus of service provision support and care

THANK YOU
- Slides: 39