WEEKLY IRON FOLIC ACID SUPPLEMENTATION WIFS NIPI Block

WEEKLY IRON & FOLIC ACID SUPPLEMENTATION WIFS/ NIPI Block level Officers Orientation 08. 01. 2017 Dr PREM SINGH, MPH State Nodal Officer-WIFS

Concerns of �Hon’ble Health Minister, Govt. of Rajasthan �Chief Secretary of Rajasthan (1, Sept 2016) �Principal Health Secretary �SS & Mission Director, NHM �Secretary to Government-Education �Director, ICDS �UNICEF And more than that definitely ‘All of us’

Anemia �Anemia is manifestation of under nutrition and poor dietary intake of Iron affecting not only a section but entire population �It is a condition in which the body does not have enough healthy red blood cells to bring oxygen to body tissues.

Rationale: Evidence � Anemia is multi-factoral in etiology � Iron and folate deficiency are common � Iron deficiency is related to nutritional deficiency, intestinal helminthic deficiency and folate deficiency due to poor intake and chronic hemolytic stage � Besides these, Malaria and other chronic diseases like Tuberculosis, HIV and cancers remain as major contributors to anemia.

Reduced physical development Decreased work output Reduced cognitive development Adolescent Anaemia Decreased work capacity Irregular menstruation Impaired sexual and reproductive development Low prepregnancy iron stores Diminished concentration Poor Disturbance learning ability in perception LBW babies and preterm delivery

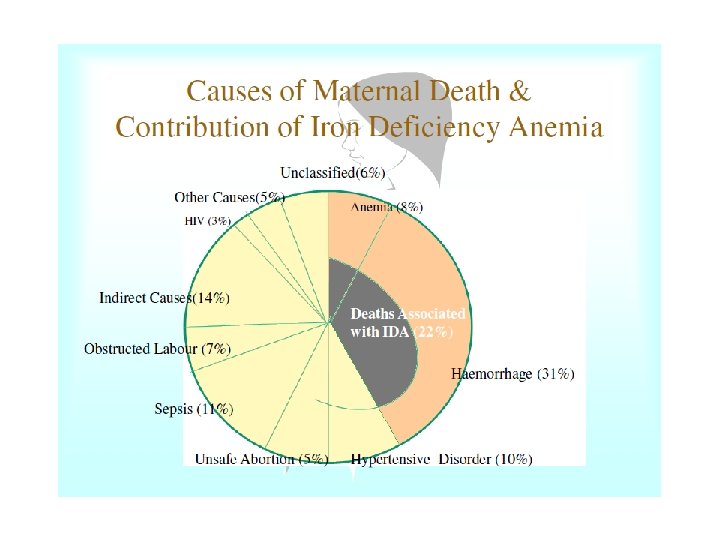
Rationale: Evidence • Anaemia in pregnant women reduces womens ability to survive bleeding during and after child birth • Risk of maternal mortality decreases by about 20%for each one g/dl increase in Hb • Reduction in severe anemia is evidenced in pregnant women who receive regular malaria prophylaxis in malaria endemic areas • 20% maternal deaths are attributable due to

Iron Deficiency Anemia � By the time a person is diagnosed with anemia, the body stores are nil and the RBC Iron is to the minimal level

Health Economics of Micronutrient deficiencies in children �Anemia and other key micronutrient deficiencies can directly attribute to Depressed Cognition Inferior school performance Reduced future earnings & productivity Depressed immunity Repeated infections

Health Economics of Anemia…. cont Impact on Productivity: � In an anemic individual, the aerobic capacity, endurance and energy efficiency are compromised 10 -50% ▪ IDA “reduces the work capacity of individuals and entire populations, bringing serious economic consequences and obstacles to national development’’ (WHO). � Anemia hits hard on productivity with an estimate of 5% deficit among all “blue collar” jobs to additional 17% loss for Heavy manual labor such as agriculture and construction (The Journal of Nutrition, 2002) � India loses 0. 9% of its gross domestic product (GDP) due to IDA (Food Policy, 2003). � This could mean a loss of up to $20. 25 billion (Rs. 1. 35 lakh crore), according to the World Bank’s estimate of India’s GDP in 2016.

Health Economics of Anemia…. cont Impact on Children � iron-deficiency anaemia severely affects cognitive performance. � It also impacts language skills, motor skills and coordination among infants and young children, and a deficit of 5 to 10 points in intelligence quotient (IQ). (Iron deficiency in infancy cannot be correct by subsequent iron therapy, according to WHO. ) � Anemic children score 0. 5 to 1. 5 SD lower on Intelligence tests where as iron interventions have similar magnitude of positive impact on cognitive scores. � Global evidences conclude that a 0. 25 SD increase in IQ level would lead to 5 -10% increase in wages

Health Economics of Anemia …. cont Micronutrient deficiencies during pregnancy results in spontaneous abortions, Pre term labour, IUGR, LBW babies and maternal deaths. • The cost implications include: • – Increased length of hospital stay – Expenses related to referral, transport of cases to hospitals with pediatric care facilities – Cost of incubators and Intensive care – Cost of post maternity care These all result in burden on State Health Budget

Global picture

Adolescent Anemia : problem scale by States

Rajasthan : Prevalence of Anaemia among Adolescents and Adults 60 55. 2 53. 9 52. 5 50. 2 50 40 33 30 22. 1 25. 2 17. 8 20 10 0 15 -19 years 20 -29 years Women 30 -39 years Men 40 -49 years

Intergenerational cycle of Anemia Adolescent enters reproductive age group with low iron stores Adolescent with low iron and hemoglobin levels + Menstrual blood loss Uncorrected anemia in infancy and childhood Pregnant women with Anemia Baby with low iron and hemoglobin levels

Anemia & Malnutrition MILD ANAEMIA MODERATE ANEMIA SEVERE ANEMIA ANY ANAEMIA 10. 0 -10. 9 g/dl 7. 0 -9. 9 g/dl <7. 0 g/dl <11. 0 g/dl Three standard indices of physical growth that describe the nutritional status of children Height-forage (stunting) Weight-forheight (wasting) Weight-forage (underweight) 18

Dietary Diversification Provide Improved Health Services Strategies for prevention of IDA IFA Supplementation with Biannual deworming Food Fortification
 Improvements in the prevalence of anaemia among women of reproductive")
Success is possible (Evidence) Improvements in the prevalence of anaemia among women of reproductive age have been seen in countries around the world*: e. g. , Burundi (64. 4% to 28% in 20 years); China (50. 0% to 19. 9% in 19 years); Nicaragua (36. 3% to 16. 0% in 10 years); Sri Lanka (59. 8% to 31. 9% in 13 years); and Viet Nam (40. 0% to 24. 3% in 14 years). *Resolution WHA 65. 6. Comprehensive implementation plan on maternal, infant and young child nutrition. In: Sixty-fifth World Health Assembly Geneva, 21– 26 May 2012. Resolutions and decisions, annexes. Geneva: World Health Organization; 2012: 12– 13 (http: //www. who. int/nutrition/topics/WHA 65. 6_resolution_en. pdf? ua=1, accessed 6 October 2014).
")
Weekly Iron Folic Acid Supplements ( Launched on July 25 th, 2013 )

National Iron Plus Initiative Launched on 2 nd Oct, 2015 by Hon’ble HM Age Group Interventi on/Dose Regime Service delivery Coverage / Status 6– 60 months IFA syrup Biweekly throughout the period 6– 60 months of age Through ASHA/(AWC 5– 10 years WIFS Junior (Pink) Weekly throughout the period 5 – 10 years of age In government school In all 33 (Class 1 - 5) through districts Teachers, Same as WIFS In all 33 districts

Objective �The Ministry of Health and Family Welfare, Government of India has launched the Weekly Iron and Folic Acid Supplementation (WIFS) Programme to reduce the prevalence and severity of nutritional anaemia in adolescent population (10 -19 years) and NIPI for age group 6 month to 10 years.
 programme will be planned")
Target groups � Weekly Iron and Folic Acid supplementation (WIFS) programme will be planned and implemented for the following two target groups in both rural and urban areas: Adolescent girls and boys enrolled in government/government aided/municipal schools from 6 th to 12 th classes. Adolescent Girls who are not in school through AWCs. � National Iron Plus Initiatives Girls and boys enrolled in government/government aided/municipal schools from 1 st to 5 th classes. 6 month to 60 month children through AWCs
")
Targets Group WIFS No. of in-school adolescents 36, 25, 691 (As per DISE 2015) No. of out-of-school girls 7, 22, 029* 43, 47, 720 All 33 districts National Iron Plus Initiatives Government Schools class- 41. 02 lakh 1 st to 5 th 6 Month to 60 month (out 63. 16 lakh of school) 104. 18 lakh

Strategy for Prevention of Anaemia in Adolescents �Fixed day, �Institution Based, �Supervised consumption, �Educating correct dietary practices & increasing iron intake, �Screening for moderate/severe anemia & referring, �Annual / biannual deworming.

Education System Approaches �Weekly Supplementation of IFA tablets on fixed day approach to school going girls and boys in the age group of 10 -19 years. �Supervised consumption of IFA �School based Deworming program �Nutrition education to increase consumption of iron rich food

ICDS Approaches �At AWCs these tablets are distributed free of cost to adolescent girls who is out of school. �For Adolescent girls-Married /Unmarried Weekly IFA for 52 weeks in a year �Information, counseling and support to adolescent girls on: • How to improve their diets, especially iron intake, • How to prevent anemia and • How to minimize the potential undesirable effects of WIFS �Referral services for adolescent girls suffering from moderate and severe anemia

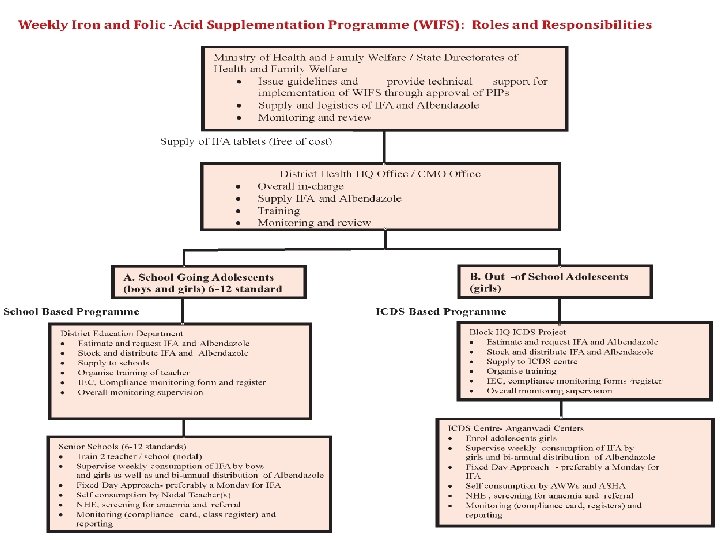
District Education and ICDS Dept As per WIFS operational framework �Ensure monitoring of programme with monthly data collection from block level �Ensure uninterrupted supply of IFA tablets at block level (school and AWC) �Ensure completion of training/orientation sessions of block officers, teachers, ICDS supervisors, ANM, AWW, ASHA and MO-PHC �Ensure IEC material displayed at school and AWC

Block Education Officer and CDPO/ICDS Officer As per WIFS operational framework �Consolidated requirements from schools and ICDS projects for block supply and share with district level �Set up distribution system for schools and AWC �Ensure uninterrupted supply of IFA �Consolidated monitoring data and share with dist. �Conduct quarterly meeting to review the programme �Ensure display of IEC

Estimation of IFA �Education IFA tablets for the year = (52 x Total number of children in 6 to 12 th standards) + (52 tablets /per teacher /year). An additional 20 % stock as buffer will be added. �ICDS Estimating IFA tablet Supply = (Number of adolescent girls registered with ICDS x 52 tablets) + (52 tablets/ year for each AWW + 52 tablets/ year for ASHA). An additional 20% is to be added for ensuring adequate stock supply.

WIFS Supply System INSTITUT E BLOCK DISTRICT • Demand from School and AWWs • Compilation at Block level (Edu & ICDS) • A Copy to BCMOs with name and demand of institutions RMSC • RMSC Supply WIFS tab/ to DDW at Districts District • RCHO receive supply from DDWs; will ensure Supply upto Block level BLOCK • BCMO will receive Supply from Dist; and Demand from BEOs/ CDPOs • Compilation at DEOs /DD ICDS offices • DEOs /DD ICDS officer to RCHO office of health Dept. BLOCK • All RCHO to State office • BCMO will ensure supply upto institutions with coordination of BEOs/Nodal/ CDPOs STATE • State Office to RMSCL for Procurement INSTITUTE • Receive supply; ensure proper storage, consumption, recording and reporting
 � STORAGE – WIFS-IFA Drugs should be kept in a cool")
WIFS-IFA DRUGS (Storage) � STORAGE – WIFS-IFA Drugs should be kept in a cool & dry place. (AVOID EXPOSURE OF DIRECT SUNLIGHT & WATER) Selection of proper place ▪ Locke and key room ▪ Limited access to the store Keep store in good condition ▪ Control the temperature in the store ▪ Control the light in the store ▪ Prevent water damage and control humidity ▪ Keep the store free of pests Keep your store clean and organized ▪ Clean the store and keep it tidy ▪ Store supplies on shelves WIFS Blue TAB Exp: …. . WIFS Pink TAB Exp: …. .
 etcl �ADMINISTRATION – IFA Drugs should be administered WEEKLY ; Schools")
WIFS-IFA DRUGS (Administration) etcl �ADMINISTRATION – IFA Drugs should be administered WEEKLY ; Schools – Monday; AWCs - Thursday) to adolescents (10 -19 years) School going adolescents & Out-ofschool adolescent girls after Mid Day Meal / Poshahaar ( NOT EMPTY STOMACH) �FEFO (First Expiry First Out) �Check Expiry in routin

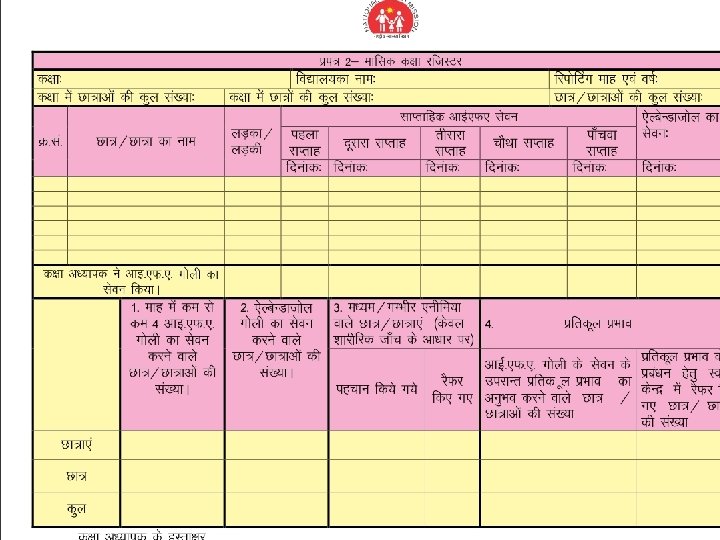
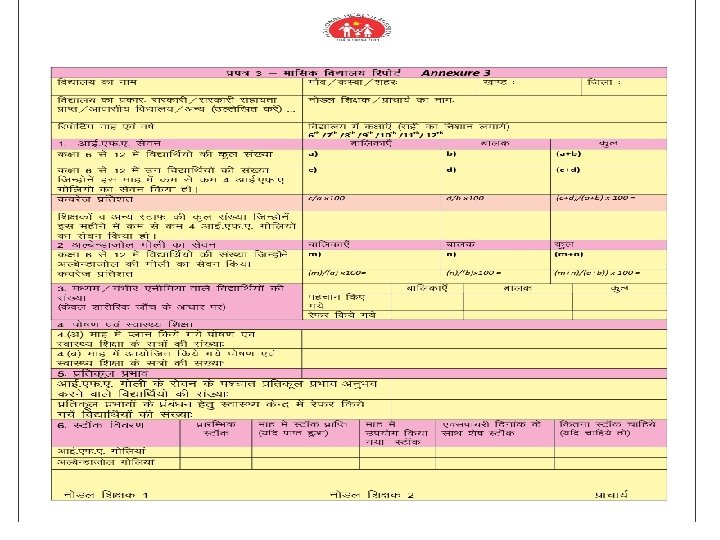
Monitoring of Programme School Level Monitoring � � Individual through ICC Class ▪ Monitoring register by class teacher School ▪ Nodal teacher, format (Annexure-3) School WIFS committee (headed by the Principal /Head Master , Nodal teachers, student representatives and ANM for regular monitoring and management of the programme) ▪ ▪ ▪ ▪ Compliance in consumption of the tablets Regular IEC and Nutrition and Health Education session Record keeping at class level Transfer of correct information from recording registers to the reporting format Timeliness of the submission of monthly reports Ensuring timely IFA and Albendazole distribution Proper storage of IFA and Albendazole tablets

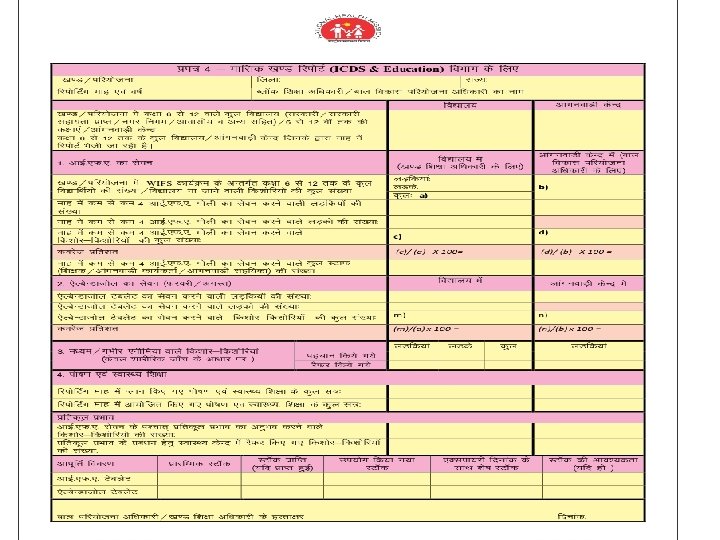
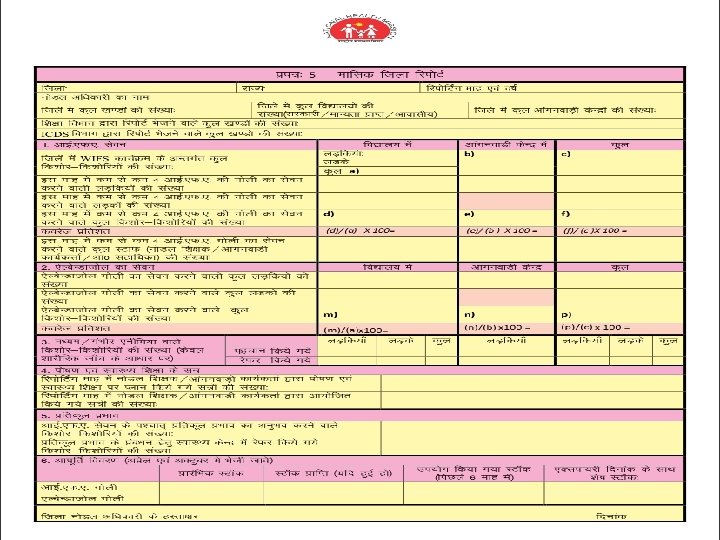
Monitoring of Programme � Block Level Monitoring The Block Education Officer will review the monthly report from each school and consolidate the reports for all schools in the block and submit it to the District Education Officer as per Annexure 4. � District Level Monitoring (District WIFS Advisory Committee) {it is merged in District Health Society at district level} Status of implementation of the programme and timeliness of the submission of monthly reports Facilitate convergence and ensure use of community based platform like VHSCs for community mobilization and awareness Training Timely and adequate supply and distribution of IFA and Albendazole tablets Provision and usage of IEC materials
 (State WIFS Advisory Status of implementation of")
Monitoring of Programme �State Level Monitoring Committee) (State WIFS Advisory Status of implementation of the programme and timeliness of the submission of monthly reports Facilitate convergence Training Timely and adequate supply and distribution of IFA and Albendazole tablets Provision and use of IEC and counseling materials Ensuring quality control

Samblambn Monitoring Report A initaive of education dept कर म क 2 4 6 7 8 11 12 15 16 17 20 21 23 24 29 30 31 32 ज ल ALWAR BARAN BHARATPUR BHILWARA BIKANER CHURU DAUSA GANGANAGAR HANUMANGARH JAIPUR JHALAWAR JHUNUN KARAULI KOTA SAWAI MADHOPUR SIKAR SIROHI TONK ब लक बचच /ब ल क दव र ओ क कल व दय लय श च लय ल ए अलग अवल क म क -अलग त पयजल उपय ग श च लय व ध सव ध क य लय उपलबध ह सव ध ज रह उपलबध ह ह श च ल यम न यम त जल आपरत क वयवस थ ह श ल सवछत बचच हत क स बन उपलवध स ह थ कर ई गय ध न क र श (500ल ए अलग र स परत म ह सव ध )पर पत उपलबध ह ह गय ? प ष ह र (म ड ड म ल )स पहल बचच स बन स ह थ ध त ह ? र षट य ब ल श ल सव सथय क रयकरम क अतरगत बचच क सव सथय पर कषण कर ल य गय ह ? ब लक ब ल क ओ क स पत ह क आयरन ग ल द ज रह ह ? 283 158 195 188 170 246 122 186 130 443 157 187 127 160 230 134 141 183 168 240 90 185 119 390 141 178 86 155 268 151 187 184 158 226 119 182 113 424 149 187 117 155 278 143 186 184 166 234 120 181 119 434 152 184 115 155 222 84 130 152 139 188 69 151 102 350 122 166 67 126 252 139 181 171 150 215 109 171 109 364 149 162 118 132 275 147 175 186 165 234 109 170 118 423 148 182 113 152 276 150 187 183 166 232 117 181 119 428 154 184 114 159 207 100 144 166 116 189 58 185 88 221 119 181 66 126 226 142 168 182 127 228 115 120 110 379 124 183 103 148 161 130 154 118 159 152 155 124 134 295 125 159 261 113 143 274 123 154 286 124 156 227 92 115 276 118 151 285 118 148 290 120 154 214 75 116 263 105 148
 S. N o From Form To Dead Line 1 School Principal Annex")
Reporting schedule(Education) S. N o From Form To Dead Line 1 School Principal Annex 3 BEO Copy to ANM 5 th of every month 2 Block Education Officer / Nodal Annex 4 District Education Officer & Copy to BCMO 7 thof every month 3 District Education Officer Annex 5 Dist RCHO office Copy to State Education Dept 10 th of every month 4 Dist RCHO office State Nodal Officer. WIFS 15 th of every month
 S. N From o Form To Dead Line 1 AWW Annex 7")
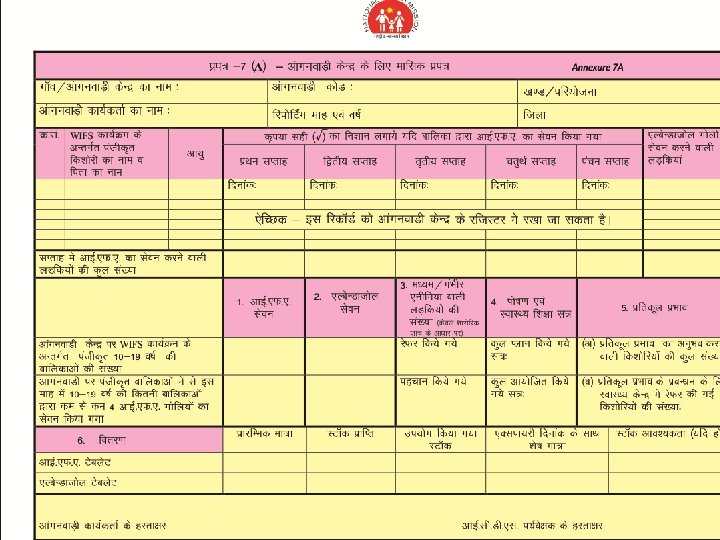
Reporting schedule(ICDS) S. N From o Form To Dead Line 1 AWW Annex 7 A LS 5 th of every month 2 LS Annex 7 B CDPO Copy to ANM 7 thof every month 3 CDPO Annex 4 DD, ICDS & Copy to BCMO 9 th of every month 4 DD, ICDS Annex 5 RCHOs Copy to Dir, ICDS 12 th of every month 4 Dist RCHO office State Nodal Officer-WIFS 15 th of every month

Individual Compliance Card
")
NIPI Reporting format (IFA Syrup)

WIFS Junior Reporting Format

On Web �http: //rajswasthya. nic. in/ �https: //www. facebook. com/rksk. rajasthan �http: //nrhm. gov. in/nrhm-components/rmnch- a/adolescent-health-rksk/weekly-iron-folicacid-supplementation-wifs/background. html

Issues in Reporting �Data Quality �Non Reporting �Irregular Reporting �Time of reporting �Old formats �Change denominator �Over Reporting

Summry � Public Health Challenge of our Country. � Find the gap in implementation of prog and resolve it immediately � Include in Health Education (Anemia) in school routine system. � Priorities and Increase focus and visibility in community. � Regular availability/supply of supplements in inst. � Regular Reporting (it is reflection of your dist) � Regular agenda of DHS & BHS. � Increase convergence among inter and intra depts. � Use innovation for implement and increase reliance of public. � Adverse event � Media management � Remember 3 mantra to OVERCOME from anemia WIFS Nutrition education (Ion Reach Source) Deworming (National Deworming Day)

Take Care of Adolescent, They will take care of Country
")
Action Plan District wise SN Issues Action Point 1. Cover those schools /AWCs (if) where prog is not implemented 1. 2. Regular Reporting 1. 2. 3. Submission of remaining reports 1. 2. 4. Maintain data quality of reports 5. Ensuring continuous drug supply in institutions 6. Awareness /Sensitization among students & Parents 7. Convergence issue Time line

Contact details: At State- Dr Prem Singh SNO- Adolescent Health-WIFS Mobile no: 9460060445 Email: wifs. raj@gmail. com premsingh 111@gmail. com At Districts- Reproductive & Child Health Officers At Block Chief Medical & Health Officers
- Slides: 56