Wee FIM Alyssa Sherd Rachel Elery History Created

 for adults Criterion")






 2=Maximal")
 & total raw score")








- Slides: 23
Wee. FIM Alyssa Sherd & Rachel Elery
History Created in 1987 Adaptation of the Functional Independence Measure (FIM) for adults Criterion and norm-referenced
Wee. FIM Purpose & Philosophy Intended to provide an overview of child’s functional status Should be used in conjunction with other assessments of daily living skills Measures burden of care and disability Assists in setting treatment goals Tracks child’s outcomes and monitors changes
Who can administer? Not domain-specific, so used by multiple health professionals Administrators must be trained and pass exam Re-certification every 2 years
Cost & Availability $4, 100 for inpatient & outpatient training programs Includes: Wee. FIM instrument & Data set Wee. FIMware software National Database & Benchmark Reports Education, training, credentialing, & consulting Research & Development
Who does it measure? No disability: children 6 months to 7 years Initial Disability: normative sampling of 400 children 6 months to 18 or 21 years Congenital, developmental, or acquired disabilities Functioning at or below 7 years
Assessment Direct 15 -30 observation, interview, or both minute administration time Inpatient, settings outpatient, & community-based
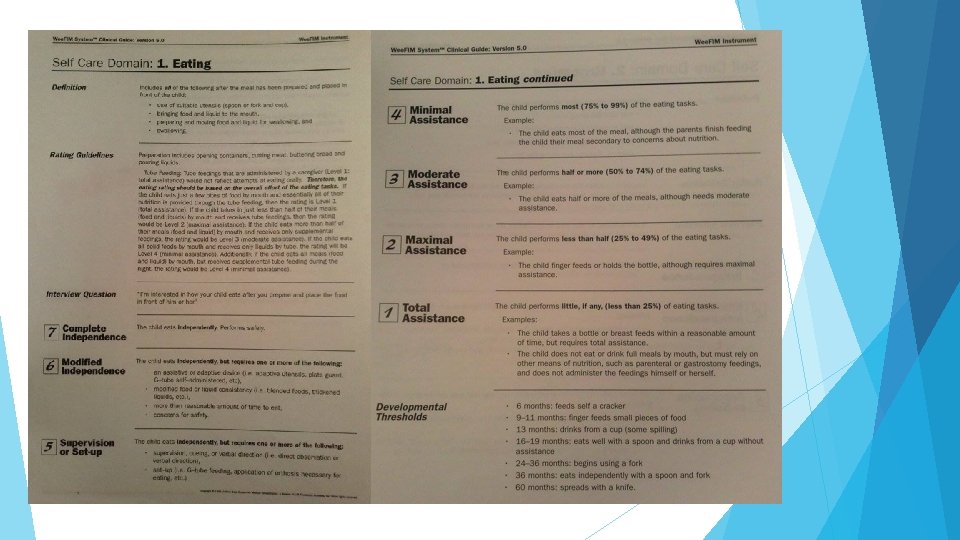
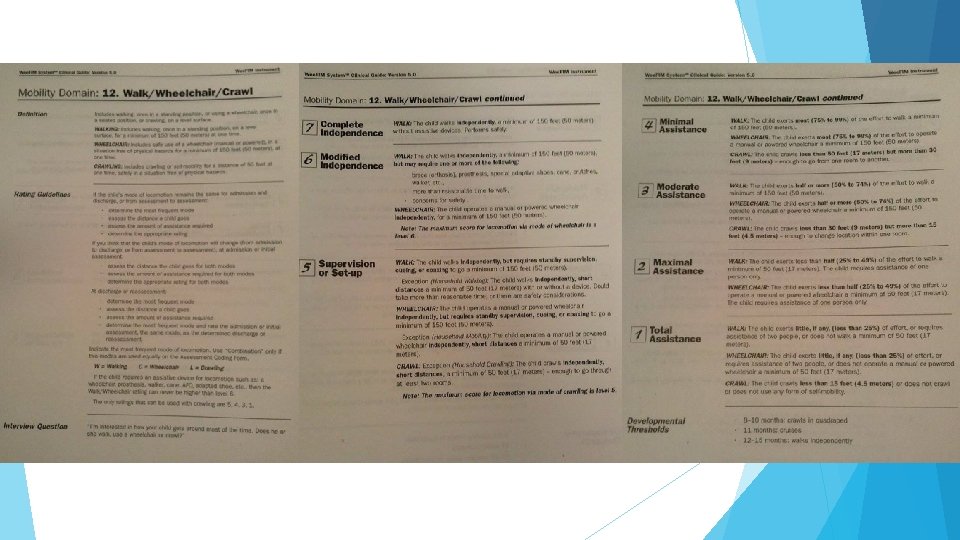
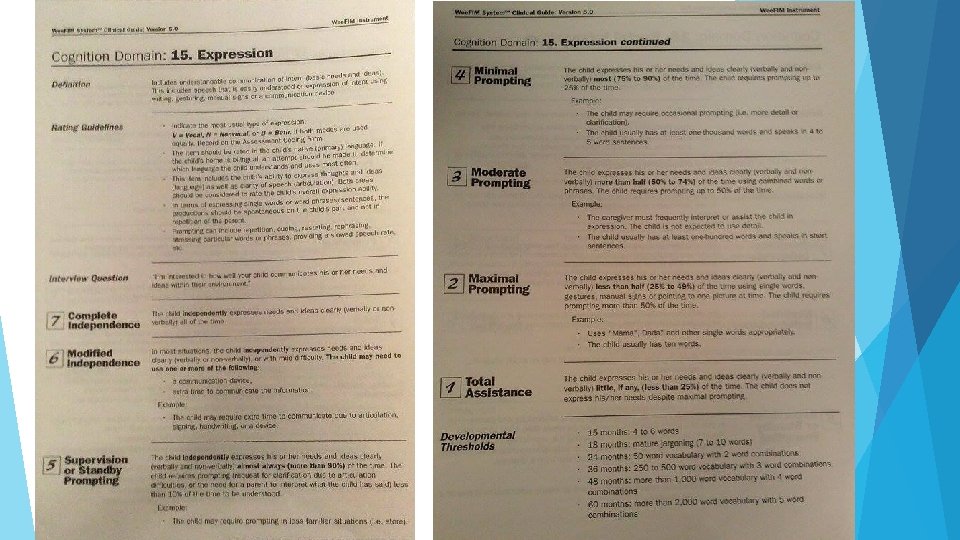
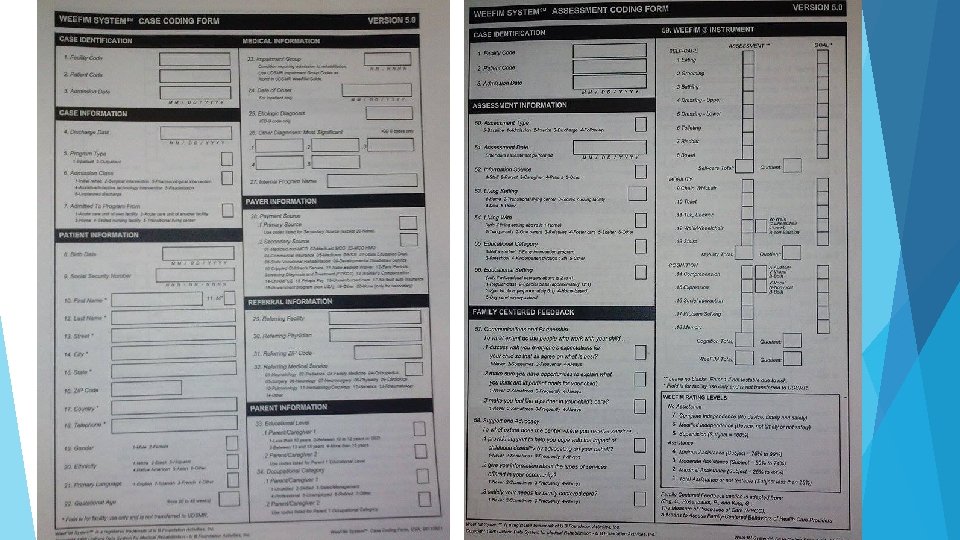
Measurement 18 items measured within 3 domains: Self-care Mobility Cognition All 18 must be rated
Scoring 7 -level 1= ordinal scale Total assistance (child performs >25% of task) 2=Maximal assistance (25 -49%) 3=Moderate assistance (50 -74%) 4=Minimal assistance (<75%) 5=Supervision/setup 6=Modified independence 7=Complete independence
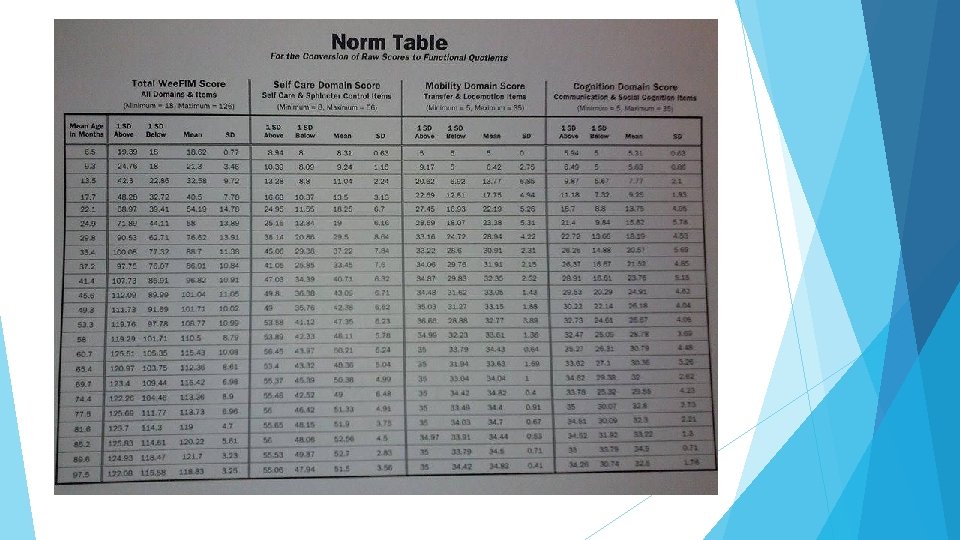
Rating & Interpretation Calculate Wee. FIM items (self-care, moblility, cognition) & total raw score Convert (raw scores to functional quotients score ÷ age-based norm score) x 100 Refer to norm table and graphs for data
Psychometric Properties Normative sampling of over 400 children without disabilities ages 6 months to 8 years Statistically significant correlation between Wee. FIM ratings and chronological age Studies of children with disability Test/retest & inter/intrarater reliability Equivalence reliability
Research: Cerebral Palsy in Turkey 134 children ages 6 months to 16 years Varying degrees of CP Wee. FIM has strong: Test-retest Internal reliability consistency Interrater reliability
Research: Norms for Children in China 445 typically developing children Ages As 6 month to 7 years age progresses, so does independence Concluded environmental and cultural differences in level of independence by age
Research: Equivalence Reliability 30 children with developmental disabilities Ages 19 -71 months Assessed with direct observation and parental interview Agreement between the two methods was found Established usefulness of interviewing
0 -3 Module Measures the precursors to functioning Contains 36 items in 3 domains (motor, cognitive, behavioral) Used when child is rating is less than 30 on Wee. FIM Uses a four-level rating system: 3=Usually 2=Sometimes 1=Rarely 0=Never
Group Activity Case EDIT studies THIS TO INCLUDE THE 3 ITEMS WE WANT THEM TO SCORE
Strengths & Weaknesses Strengths: Weaknesses: Abundance of research across ethnicities and diagnoses in support of the reliability and validity Still could be some room for subjectivity in scoring Parents may not give true/accurate depiction of their child’s abilities Can be administered by a variety of healthcare professionals Training program for facilities is very expensive Can be administered in a variety of healthcare settings Scoring sheet is confusing and difficult to navigate Helps determine goals for client and monitor gains in functioning Short administration time Information and norms may need to be updated since this evaluation tool was established almost thirty years ago
References Niemeijer, A. S. , Reinders-Messelink, H. A. , Disseldorp, L. M. , & Nieuwenhuis, M. K. (2012). Feasibility, reliability, and agreement of the Wee. FIM instrument in Dutch children with burns. Physical Therapy. 93(7), 958 -966. Occupational Therapy for Children Assessment Portfolio. (2013). Pediatric functional independence measure (Wee. FIM). Retrieved from http: //otforchildrenassessmentportfolio. blogspot. com/2013/04/pediatric-functionalindependence. html Sperle, P. A. , Ottenbacher, K. J. , Braun, S. L. , Lane, S. J. , & Nochajski, S. (1997). Equivalence reliability of the Functional Independence Measure for Children (Wee. FIM) administration methods. The American Journal of Occupational Therapy. 51(1), 35 -41. Tur, B. S. , Kucukdeveci, A. A. , Kutlay, S. , Yavuzer, G. , Elhan, A. H. , & Tennant, A. (2009). Psychometric properties of the Wee. FIM in children with cerebral palsy in Turkey. Developmental Medicine and Child Neurology, 51(9), pp. 732 -738. DOI: 10. 1111/j. 1469 -8749. 2008. 03255. x Uniform Data System for Medical Rehabilitation. (2009). The Wee. FIM II teaching guide, version 1. 0. Buffalo, NY: UDSMR. Wee. FIM System Clinical Guide: Version 5. (1998). Buffalo, NY: University at Buffalo Wong, V. , Wong, S. , Chan, K. , & Wong, W. (2002). Functional Independence Measure (Wee. FIM) for Chinese children: Hong Kong Cohort (Abstract). Pediatrics (Evanston). 109(2), pp. 309 -310.