WATER ELECTROLYTE IMBALANCE DR SUDHANSHU KOTHADIA NORMAL WATER

WATER & ELECTROLYTE IMBALANCE DR. SUDHANSHU KOTHADIA
")
NORMAL WATER BALANCE Total Body Water in 65 kg man Intracellular Fluid (28 L) 60 -75% Fluid Extracellular Fluid (12 L) 25 -40% Plasma Water (3 L) Interstitial (9 L)

HYPOVOLEMIA It is defined as a state of combined salt and water depletion exceeding intake leading to volume contraction. Etiology : I- ECF Volume Contracted A) Extrarenal Na Loss 1) Gastrointestinal- Vomiting Nasogastric Suction Drainage Fistula Dairrhea
 Skin/Respiratory- Insensible Loss Sweat Burns 3) Hemorrhage B) Renal Na and Water Loss")
2) Skin/Respiratory- Insensible Loss Sweat Burns 3) Hemorrhage B) Renal Na and Water Loss 1) Diuretic 2) Osmotic Diuresis 3) Hypoaldosteronism 4) Salt and Water imbalance C) Renal Water Loss
 ECF Volume Normal or Expanded A) Decreased Cardiac output 1) Myocardial , Valvular")
II) ECF Volume Normal or Expanded A) Decreased Cardiac output 1) Myocardial , Valvular or Pericardial disease B) Redistribution 1) Hypoalbunaemia - Hepatic Cirrhosis - Nephrotic Syndrome 2) Capillary Leak - Acute Pancreatitis - Ischemic Bowel - Rhabdomyolysis C) Increased Venous Capicitance - Sepsis

PATHOPHYSIOLOGY Cardiac Output Hypotension Stimulates barroreceptors in Carotid Sinus & aortic arch Stimulates Renin Angiotensin system Na Reabsorption from tubule & Stimulation Of Angiotensin II GFR

CLINICAL FEATURES Symptoms - vomitting diarrhea polyurea abdominal and chest pain weakness muscle cramps thirst confusion

Signs - Cyanosis Oligourea Diminished Skin Turger Dry Oral mucus Membrane Decreased JVP Postural hypotension Postural tachycardia Cold and Clammy Extrimities Postural Disturbances
 Na Concentration - normal, or 2) Blood urea decreased is severe")
LAB DIAGNOSIS 1) Na Concentration - normal, or 2) Blood urea decreased is severe depletion 3) Urinary sodium – a) In Renal/Adrenal Causes › 20 m. Eq/L b) In extrarenal Causes ‹ 10 m. Eq/L
 Mild Volume Contraction - Oral Route 2) Severe Hypovolemia a) Normonartemic or")
TREATMENT 1) Mild Volume Contraction - Oral Route 2) Severe Hypovolemia a) Normonartemic or mild hyponatremic - Isotonic or normal saline (0. 9%Na. Cl or 154 mmol/L Na) b) Severe Hyponatremia - Hypertonic Saline(3%Na. Cl or 531 mmol/L) c) Hypernatremic - 0. 5 Normal saline or 5% Dextrose (0. 45%Na. Cl or 77 mmol/L Na) 3) Patient With Haemorhage Or Anaemia – B. T

NORMAL Na BALANCE Na is actively pumped out by Na-K- ATpase Total Body Na ECF (85 -90%) ICF (10 -15%)

HYPONATREAMIA It is defined as when serum Na is less than 135 m. Eq/L CAUSES I)PSUDOHYPONATREAMIA A)Normal plasma osmalality 1)Hyperlipidemia 2)Hyperproteinemia 3)Posttransurethral resection of prostate bladder tumor B)Increased plasma osmalality 1)Hyperglycemia 2)Mannitol or
 HYPOOSMOLAL HYPONATREMIA A)Primary Na loss(secondary water gain) 1)Intugumentary loss: sweating, burns 2)GI loss:")
II) HYPOOSMOLAL HYPONATREMIA A)Primary Na loss(secondary water gain) 1)Intugumentary loss: sweating, burns 2)GI loss: vomitting, fistula, diarrhea 3)Renal loss: diuretics, osmotic diuretics, hypoaldosteronism, tubular necrosis B)Primary water gain(secondory Na loss) 1)Primary polydypsia 2)Decreased solute intake 3)AVP released due to pain, nausea, drugs 4)Syndrme of inappropriate secretion 5)Glucocorticoid deficiency 6)Hypothyroidism 7)Chronic renal insuficiency

PATHOPHYSIOLOGY It is due to either retention of water or loss of Na Mechanism Excessive ingestion SIADH Of water excretion of water slow urine flow due to Kidney failure in kidney failure
Headache 2)Lythargy 3)Confusion")
CLINICAL FEATURES Symptoms mainly depends on severity and rapidity of hyponatremia 1)Headache 2)Lythargy 3)Confusion 4)Stupor 5)Siezures 6)Coma-generaly if Na falls below 120 m. Eq/L acutely
Plasma osmalality a)In primary hyponatreamia-decreased (If not decreased rule out psudohyponatremia) II)Urine osmalality")
DIAGNOSIS I)Plasma osmalality a)In primary hyponatreamia-decreased (If not decreased rule out psudohyponatremia) II)Urine osmalality a)Primary polydypsia -urine osmalality less than 100 mmol/Kg -specific gravity less than 1. 003 (If not then suspect impaired free water exceation) III)Urinary Na concentration-if more than 20 mmol/L -a)salt wasting nephropathy b)diuretic therapy c)hypoaldosteronism d)occasionaly vomitting IV) Urinary K Low For SIDAH – hyposmotic hyponatremia - urinary Na › 40 mmol/L
 Main Points we have to remember dur ing T/t 1) Rapid correction")
TREATMENT A) Main Points we have to remember dur ing T/t 1) Rapid correction leads to vascular overload & brain shrinkage 2) Rate of correction should be around 0. 6 MEq/L 3) It requires either addition of Na or removal of water or 4) when slow correction of hyponatremia in volume expanded subject is desired, best to restrict fluids- if not possible then use Loop Diuretics
 Hypertonic Saline a) For Symptomatic – 3% hypertonic saline b) For chronic –")
B) Hypertonic Saline a) For Symptomatic – 3% hypertonic saline b) For chronic – rate should not exceed 0. 5 m. Eq/L c) For A. C. – 1 -2 m. Eq/L d) Na level check after 2, 3, 6 hrs C) Vasopressin V₂ receptor Antagonist a) Tolvaptan – orally useful in chronic hyponatremia b) S/E - urine flow, thirst and dry mouth

HYPERNATREMIA An elevation in the serum Na concentration above 145 m. Eq/L is Hypernatremia. CAUSES 1) Decreased Intake – coma, depression, inability to swallow 2) Loss From Skin – fever, hyperthyroidism, hot environment 3) Respiratory Loss – Hyperventilation 4) Loss In Urine – Diabetes Insipidus, medullary cystic disease

PATHOPHYSIIOLOGY Hypernatremia is much less common than Hyponatremia because even a small increase in the serum Na concn. is a potent stimulus to thirst. Elevated Na conc. develops only in those patients who are unable to experience thirst or are unable to gain access to water. EFFECTS OF HYPERNATREMIA ON BRAIN : Within minutes after the development of hypertonicity, brain cells loss water causing shrinkage of the brain and an incerase in osmorality. Rapid adaptation occurs within a few hours as elecrolyte enter the brain cells causing partial increase in brain volume. Over several days, the brain volume becomes normal due to intracellular accumulation of organic compounds. Slow correction of the hypertonic state does not induce cerebral oedema as the accumulated solutes are gradually shifted out of the brain cells. In contrast, rapid correction may result in cerebral oedema as brain uptakes water from the relatively hypotonic extracellular fluid.
 2) 3) 4) 5) 6) 7) 8) 9) Altered mental state")
CLINICAL FEATURES 1) 2) 3) 4) 5) 6) 7) 8) 9) Altered mental state Weakness Neuromuscular irritability Focal neurological deficit Occasionally coma and seizures Exessive sweating Diarrhoea Osmotic diuresis Polyurea and thirst Morality rate associated with Na conc › 180 mmol/L
 2) 3) 4) Haematocrit usually › 50% Blood urea levels Plasma")
LAB DIAGNOSIS 1) 2) 3) 4) Haematocrit usually › 50% Blood urea levels Plasma Na Urine specific gravity › 1. 010 Water deficit – plasma Na conc – 140 Total Body Water

MANANGMENT In patients with gradual onset of depletion of water over more than 2 days, correction should be done slowly as rapid lowering of Na produces shift of water from ECF into brain cells. The rate of correction should not exceed 0. 7 m. Eq/L/hr When hypernatremia is associated with hypotension due to volume depletion, the initial solution should be isotonic saline so as to increase the ECF volume. However, if neurological features are also present, therapy should be started with N/2 saline. As a rough guide, the box on next slide shows the requirment of fluids in 65 -kg person.
 Fluid and route of administration Quantity & time for replacmnt water by")
Severity 1) Fluid and route of administration Quantity & time for replacmnt water by mouth or 5% glucose IV 2 L, over 6 -12 hrs 5% glucose IV 2 -4 L, over 24 hrs Severe 0. 9% Na. Cl IV 1 L, over 1 hour (4 -10 L deficit) 5% Dextrose IV 3 L, over 2 hours 5% Dextrose IV 4 L, ovr 24 -48 Mild depletion (1 -2 L deficit) 2) Moderate (2 -4 L deficit) 3) hrs Relief of thirst, urine output more than 1500 m. L/24 hrs and normal plasma Na levels indicate adequate correction.

NORMAL POTTASIUM BALANCE Normal K⁺ - 3. 5 – 5 mmol/L Almost 98% of it is present in ICF. Abundent in meat, oranges, lemon, grapes, bananas and dry fruits. PHYSIOLOGY 1) 2) 3) 4) Mainly intracellular cation & maintained by Na-K stimulated ATP ase system. Greatly influences neuromuscular function as latter depends upon ratio of ICF: ECF For loss or gain of 100 -200 m. Eq, the plasma K reduces or increases by 1 m. Eq/L Renal Excretion mainly by secretion at the levels of collecting ducts.

HYPOKALEMIA It is defined as plasma K⁺ conc. ‹ 3. 5 mmol/L CAUSES – 1) Decreased Intake a) starvation b) clay ingestion 2) Redistribution Into Cells a) Acid Base 1) Metabolic alkalosis b) Hormonal 1) Insulin 2) β₂ Adrenergic agonists 3) α Adrenergic antagonists c) Anabolic State 1) Vitamin B₁₂ or Folic Acid 2) Granulocyte-macrophase colony stimulating factor 3) Total parental nutrition d) Other 1) Psuedohypokalemia 2) Hypothermia 3) Hypokalemic Periodic Paralysis 4) Barium Toxicity
 Increased Loss A) Nonrenal 1) Gastrointestinal loss(diarrhea) 2) Integumentary Loss(Sweat) B) Renal 1)")
3) Increased Loss A) Nonrenal 1) Gastrointestinal loss(diarrhea) 2) Integumentary Loss(Sweat) B) Renal 1) Increased distal flow : diuretics, osmotic diuresis 2) Increased secreation of pottasium a) minaralocorticoid excess: primary & secondary hyperaldosteronism, renin-screting tumors, renal artery stenosis b) Distal delivery of non-reabsorbed anions : vomitting, nasogastric suction, diabetic ketoacidosis c) Other : amphotericin B, hypomagnesemia
 Generalised muscle weakness & depression of tendon reflexes 2) Paraesthesiae, apathy,")
CLINICAL FEATURES 1) Generalised muscle weakness & depression of tendon reflexes 2) Paraesthesiae, apathy, confusion & coma 3) Paralytic ileus 4) Rhabdomyolysis 5) ECG changes of hypokalemia include flattening & inversion of T waves, satgging of the ST segment, and appearance of U wave 6) Atrial & ventricular arrythmias may occur, especially in patients receiving digitalis 7) Death may occur due to respiratory paralysis or cardiac arrest
 T/t must be directed at correcting hypokalemia & eliminating the cause of")
MANAGEMENT 1) T/t must be directed at correcting hypokalemia & eliminating the cause of K loss. K supplimentation can be given orally or IV in the form of KCL. 2) Patients with mild hypokalemia with K bet. 3 -3. 5 m. Eq/L are usually asymptomatic & don’t need urgent treatment. these patients should be advised to take a diet rich in potassium. 3) Patients with mild hypokalemia with K bet. 2. 5 -3 m. Eq/L should receive oral pottasium in a dose of 60 -80 m. Eq/day in divided doses(20 m. L of KCL oral solution contains 15 m. Eq of K) 4) If patient cant tolerate oral pottasium or GI losses are massive, IV K supplimentation is required. patients with symptomatic moderate or severe hypokalemia with K below 2. 5 require IV K. 5) Isotonic saline (500 m. L) containing 20 m. Eq of K(as chloride) should be given over 2 -3 hrs. Repeted measurments of plasma K are necessary to determine whether further KCL is required. It is also preferable to monitor the patient using cardiac monitor.

HYPERKALEMIA Hyperkalemia is defined as a plasma K⁺ conc. › 5 mmol/L. CAUSES : Renal Failure Decreased distal flow(i. e; decreased effective circulating arterial volume 3) Decreased K⁺ secretion A) Impaired Na⁺ reabsorption a) primary hypoaldosteronism : adrenal insufficiency, adrenal enzyme deficiency b) Secondary hypoaldosteronism : hyponatremia, drugs(NSAIDs, heparin, ACE inhibitors c) Resistance to aldosterone : pseudohypoaldosteronism B) Enhanced Cl⁻ reabsorption(chloride shunt) a) Gordon syndrome b) Cyclosporine 1) 2)
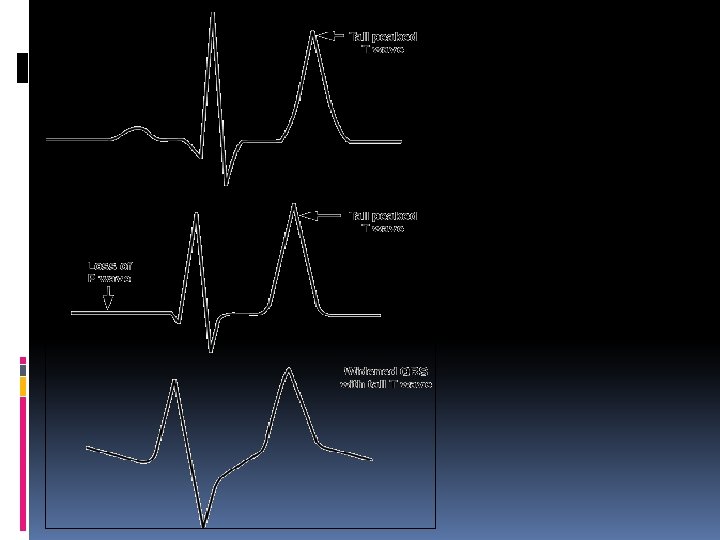
 The common clinical features include cardiac arrythmias, muscular weakness progressing to")
CLINICAL FEATURES 1) The common clinical features include cardiac arrythmias, muscular weakness progressing to flaccid paralysis & respiratory embarrassment. 2) ECG manifistations : a) Tall, peaked T waves b) Prolongation of PR interval c) Reduced height of P waves d) Prolongation of QRS complex e) ‘Sine wave’ pattern 3) Terminally ventricular fibrillation and standstill may occur.
 2) 3) 4) 5) 6) 7) Identification and elimination of underlying cause.")
MANAGEMENT 1) 2) 3) 4) 5) 6) 7) Identification and elimination of underlying cause. When there are marked ECG changes, 10 m. L of 10% calcium gluconate solution is given IV slowly over 2 -5 min. It stabilises the myocardial cells. IV administration of glucose along with insulin encourages shift of pottasium from extracellular compartment to intracellular compartment. a) 50 m. L of 50% glucose plus 10 units of soluble insulin(plain) may be given IV as a bolus. b) Alternatively, 500 m. L of 20% glucose plus 10 units of soluble insulin may be given as an infusion over 6 -12 hrs. IV administration of 50 -100 m. L of 8. 4% sodium bicarbonate is useful in renal failure patients with hyperkalemia & acidosis. Nebulisation of β-agonists also can reduce pottasium levels by producing shift of pottasium to intracellular compartment. Dose of salbutamol is 10 -20 mg over 10 min & can be repeted every 2 -6 hrs. Cation exchange resins such as sodium polystyrene sulphonate are helpful in the removal of K⁺. The resins can be given orally or as enema. If these measures fails then haemodialysis is done.

THANK YOU
- Slides: 34