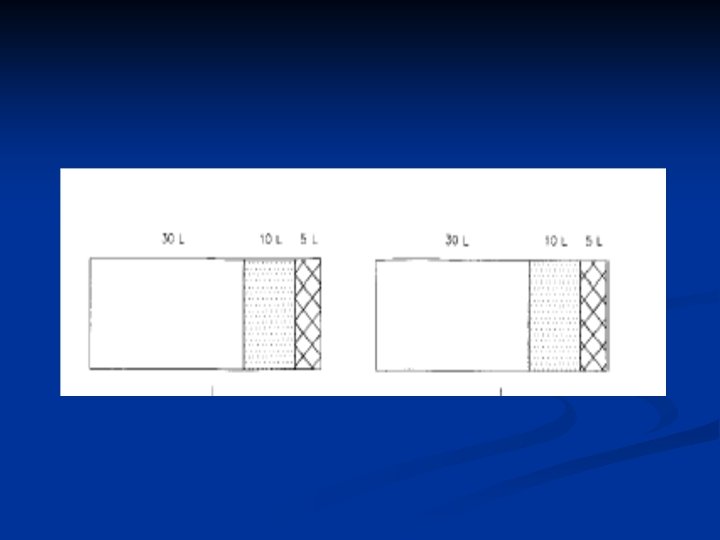
Water and electrolyte disturbances n TBW M 50

Water and electrolyte disturbances

n TBW M= 50% BW F= 60% BW

n Sodium is the chief extracellular cation and is critical to regulate extracellular and intravascular volume. n The sodium concentration itself is the single ion that best represents serum osmolality; n Essentially all of the clinically relevant symptoms of dysnatremia are secondary to alterations in osmolality.

n Osmolality measures all of the solutes in solution, n tonicity only includes particles that are unable to cross from the intracellular to the extracellular compartment. It is these particles which are osmotically active, and by drawing water across compartments they may alter cell volume. n Sodium and potassium are the primary determinants of tonicity.

n There is tight control despite variable fluid and solute intake n Water balance is maintained by thirst and antidiuretic hormone (ADH).

n n n Following a water load, osmolality falls and osmoreceptors in the hypothalamus suppress thirst and ADH release. The latter signals the kidney to produce dilute urine to clear the water load. In states of water deprivation (or a solute load) osmoreceptors detect the rise in osmolality and increase thirst and ADH. The kidney regulates osmolality and sodium concentration by diluting or concentrating urine.

U osmolality 50 – 120 mosm/ Kg H 2 O n UOP 0. 5 – 20 L/ day n

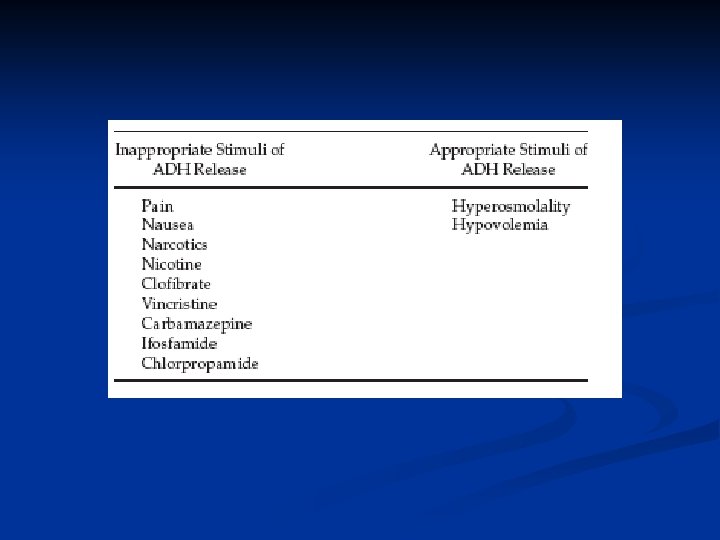
n n n Release of ADH follows increases in osmolality or dramatic drops in blood pressure or effective arterial blood volume. serum osmolality of 1% (2 m. Osm/kg) Loss of 7% to 10% of blood volume When osmolality suppresses and volume depletion stimulates ADH release, volume effects predominate Osmolality is a more sensitive ADH stimulus, while volume is a more potent ADH stimulus.

1 Translocation Glucose 0. 016 - 0. 024 Glycerine, mannitol n n n Protein 0. 025 Lipid 0. 002

2

Urinary sodium. 3 n n n Hypovol <20 renal losses >20 extrarenal losses n n n Hypervol <20 ht failure, cirrhosis, nephroyic syn >20 renal failure
 hyponatremia")
n The diagnosis of SIADH requires four criteria: 1. Hypotonic (<270 m. Osm/kg) hyponatremia (<135 mmol/L) 2. Inappropriately concentrated urine (>100 m. Osm/kg) 3. Elevated urine sodium 4. No underlying adrenal, thyroid, pituitary, or renal disease.
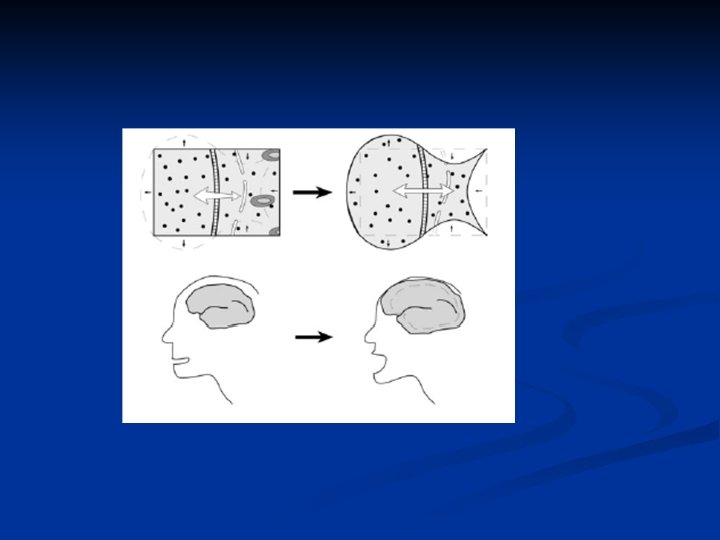

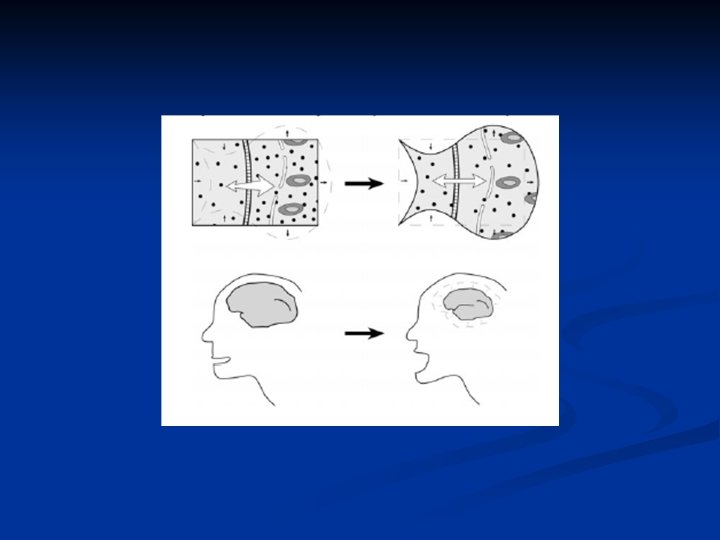
n one must balance the risk of cerebral edema from the hyponatremia against the risk of ODS from treating compensated hyponatremia.

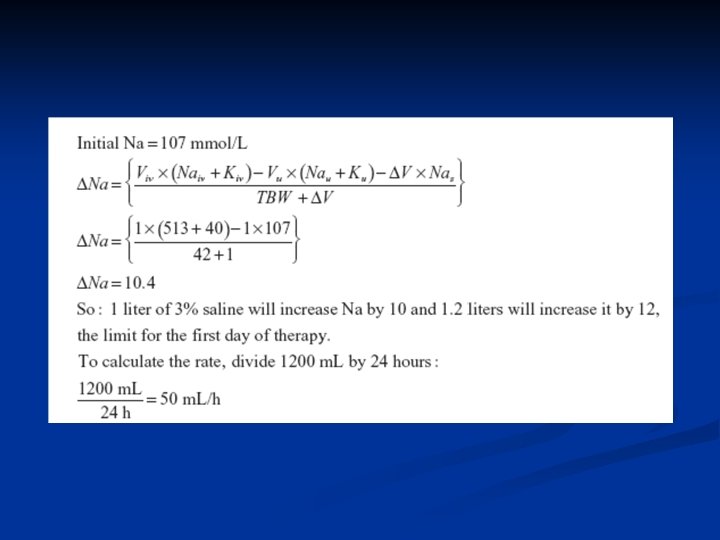
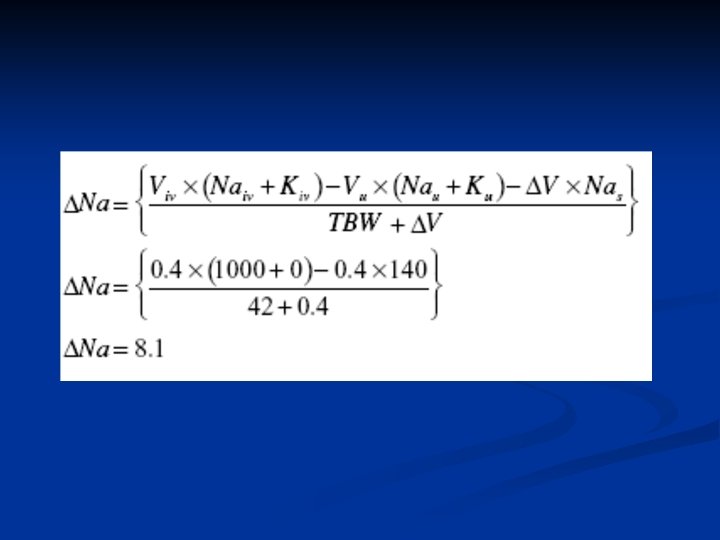
<48 sympt; Sodium levels should be initially raised rapidly until symptoms abate or the serum sodium has been raised by 4 to 6 m. Eq/L. the sodium should be raised no more than 12 m. Eq/L in the first 24 hours. n Consider lasix n > 48 sympt; 10 % (<12) 0. 5 – 1 /h n

48 asympt; Ø Euv; water restriction, demeclocyclin, Na + lasix, V 2 receptor antagonist Ø Hyper; water restriction- loop not thiazide Ø Hypo; normal saline Ø

Hypernatremia Hyperosmolar n Volume status n

Urinary Na n Hypov n hyper
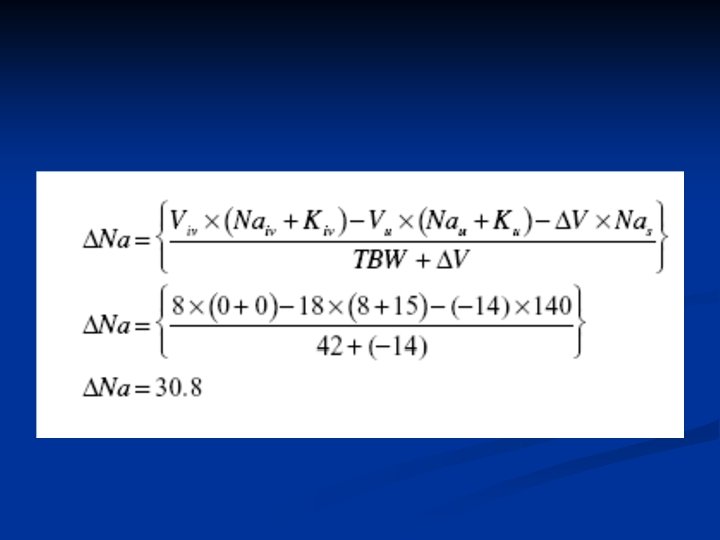

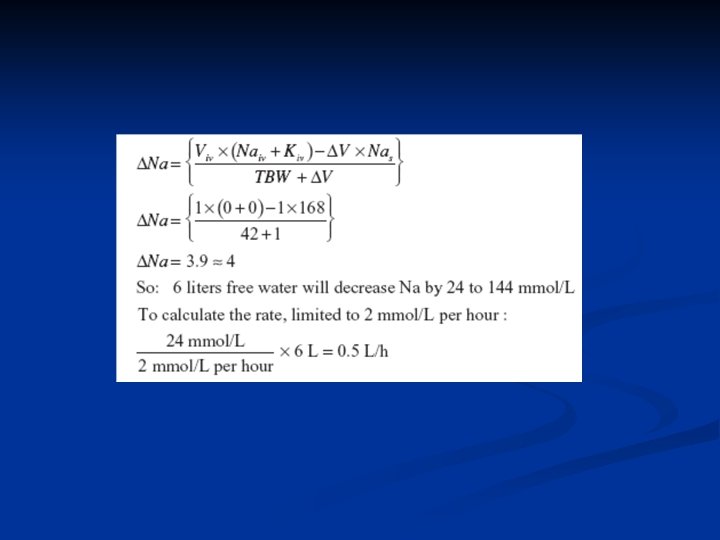
n n n The enteral route is preferred, Though the optimum speed of correction has not been rigorously determined, studies on infants and children showed no seizures when sodium was corrected at less than 0. 5 mmol/L per hour. The sodium can be safely lowered by 10 mmol in the first day of therapy. Patients with acute increases in sodium (e. g. , from hypertonic bicarbonate infusions) can safely be corrected at 1 mmol/L per hour.

+ Correct any ongoing looses n Hyprr; hypotonic fluid, loop diuretics dialysis n
- Slides: 30