VWOG richtlijn vulvacarcinoom Herfst symposium VVOG Kinepolis Brugge

VWOG richtlijn vulvacarcinoom Herfst symposium. VVOG Kinepolis Brugge Frédéric Amant Namens VWOG bestuur
 •")
Tissue is the issue! • Vulvar intraepithelial disease • Squamous cell carcinoma (90%) • Verrucoid cancer • Basal cell ca • Adenocarcinoma • Paget’s disease • Bartholin gland carcinoma (40% squamous) • Melanoma • Malignant mesenchymal tumors • Metastatic

VIN III: Triad of three P’s: parakeratosis, pigment, papulae

Vulvar Intraepithelial Neoplasia • Low grade VIN: subclinical HPV infection • High grade VIN: - moderate to severe dysplasia - undisputed malignant potential - 30 -50% co-existence with vulvar ca - S/ no, pruritus, burning, pain, dysuria - R/ surgical excision (laser, cold knife)

Diagnostic work-out Ø KO: operability & groin Ø Chest X-ray Ø CT abdomen, inclusive groin Ø SCC in blood Ø On indication: recto- en cystoscopy, CT-thorax

Treatment modalities in vulvar cancer • Stage Ia (< 1 mm depth of invasion 0% + inguin LN partial vulvectomy • Stage Ib-III (partial) vulvectomy inguinofemoral lymphadenectomy/ sentinel node procedure • Stage IVa exenteration/neoadjuvant CT/45 -65 Gy • Stage IVb palliation

Total vulvectomy

The price of less radical surgery • Surgical tumor-free margin – > 8 mm: no vulvar recurrence, n=91 – < 8 mm: 21/44 (48%) vulvar recurrence • Heaps et al. , Gynecol Oncol 1990; 38: 309 -14 • Surgical tumor-free margin – >8 mm: no vulvar recurrence, n=39 – < 8 mm: 9/40 (22. 5%) vulvar recurrence • de Hullu et al. , Cancer 2002; 95: 2331 -8

What is an adequate resection margin? Ibrahim et al. , IGCS 2006, Santa Monica Abstract 36 • 15 consecutive patients • At least 10 mm clear margin macroscopically • Reduction of clear margin – – 15% post resection 15% tissue fixation 15% microscopically Totalling 45% reduction • 1 cm is insufficient as macroscopic margin
 urethral resection de mooij et al. ,")
Impact of partial (< 1. 5 cm) urethral resection de mooij et al. , Int J Gynecol Cancer 2007; 17: 294 -7 With urethral resection (n=18) Without urethral resection (n=17) Preoperative P-value 0. 502 Continent 13(72%) 13(76%) Incontinent 3(17%) 1(6%) Unknown 2(11%) 3(18%) Postoperative 0. 860 Continent 14(78%) 15(88%) Incontinent 4(22%) 2(12%) Questionnaire 0. 494 Continent 6/8 (75%) 9/12(75%) Incontinent 2/8(25%) 3/12(25%)
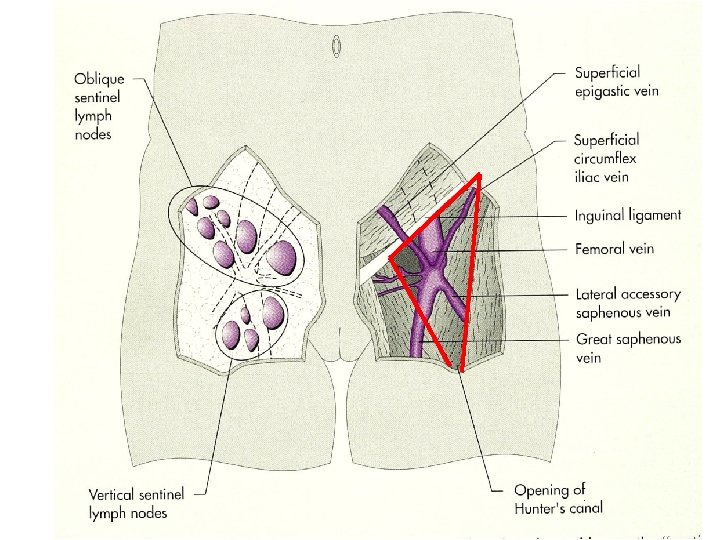
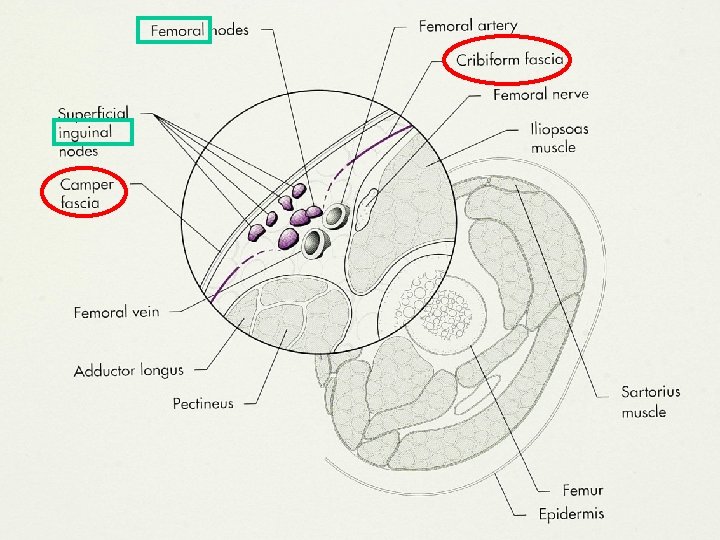

M Pectineus m adductor longus M abdominis, sheet femoral artery and vein M sartorius

Apex of the femoral triangle Femoral vein Sartorius muscle Femoral artery

Ipsilateral superficial inguinal lymphadenectomy Stehman et al. , Obstet Gynecol 1992; 79: 490 -7 Ø Prospective evaluation Ø N = 155 Ø 7. 3% inguinal recurrence rate Ø Historical control: 0% inguinal recurrence rate Recurrence rate varies from 0 -8. 6% (Berman 1989; Stehman 1992; Burke 1995; Gordinier 2003; Kirby 2005) Number of recurrences attributable to decision to leave the femoral nodes


Sentinel node dissection is safe in the treatment of early-stage vulvar cancer: morbidity Van der Zee et al. , JCO 2008; 26: 884 -9 Morbidity SLN dissection only SLN plus lymphadenectomy P 264 47 Wound breakdown, n (%) 31 (11. 7) 16 (34. 0) <. 0001 Cellulitis, n (%) 12 (4. 5) 10 (21. 3) <. 0001 8. 4 13. 7 <. 0001 Total N° of patients 264 119 Lymphedema, n (%) 5 (1. 9) 30 (25. 2) <. 0001 Recurrent erisipelas, n (%) 1 (0. 4) 19 (16. 2) <. 0001 Short term Total N° of patients Hospital stay, days Long term
 Cumulative proportion of groin recurrences in patients with unifocal vulvar cancer")
Fig 2. (A) Cumulative proportion of groin recurrences in patients with unifocal vulvar cancer < 4 cm and negative sentinel node (dark blue line); 95% CIs are also given (light blue lines) 6/259 (2. 3%) 97% 3 y survival Van der Zee, A. G. J. et al. J Clin Oncol; 26: 884 -889 2008

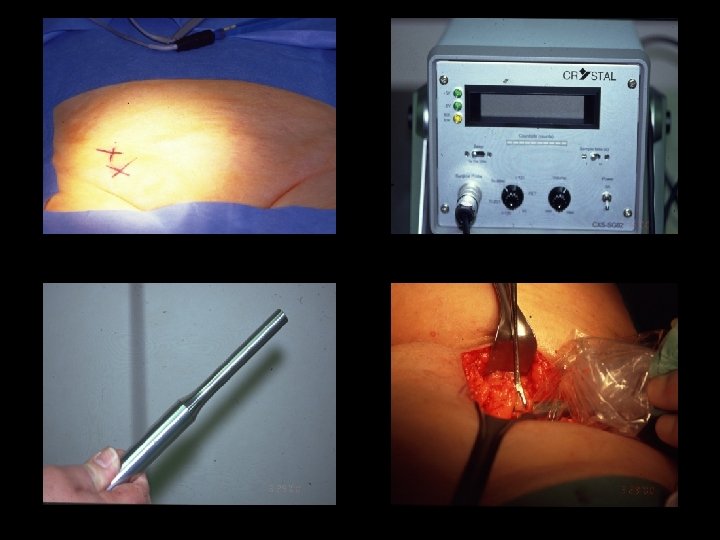
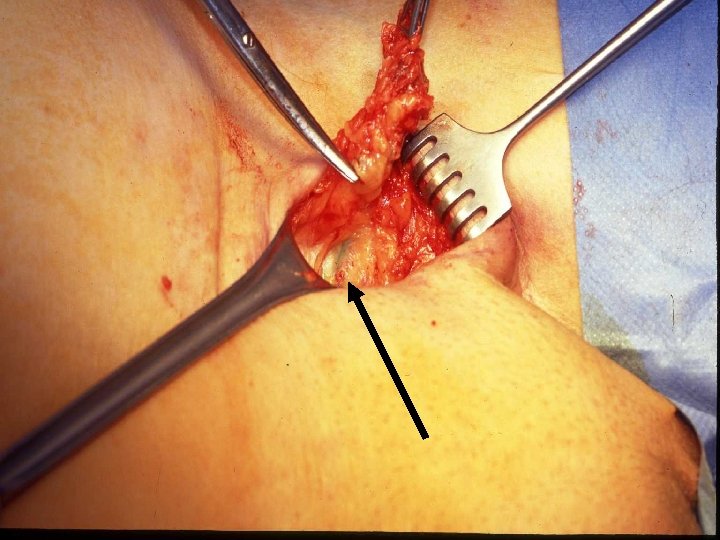
Sentinel node dissection is safe in the treatment of early-stage vulvar cancer: quality control at each step Van der Zee et al. , JCO 2008; 26: 884 -9 Injection of radioactive tracer Interpretation of lymphoscintigram Surgeon: 10 patients/year/surgeon Pathology: experience with ultrastaging

Flow chart sentinelklierprocedure de Hullu et al. , Gynecol Oncol 2004; 94: 10 -5 Patient met T 1 of T 2 (<4 cm) vulvair carcinoom zonder verdachte liezen Radiologie (Ct of MR) om verdachte klieren te identificeren; zo verdacht echografie + fijne naald aspiratie Metastase: volledige lymphadenectomie Geen metastase Geen sentinel lymfeklier: technisch falen? Logistiek probleem? Nee: volledige inguinofemorale lymphadenectomie Ja: herhaal procedure Zo meer dan 1 intranodale metastase of extranodale groei: postoperatieve radiotherapie FOLLOW-UP -Sentinel lymfeklier procedure met gecombineerde techniek (preoperatief lymphoscintigraphy met 99 m Technetium gelabeld nanocolloid en patent blauw). -Verwijderde SLNs voor vriescoupe. -Intraoperatieve palpatie om vaste lymfeklieren te voelen. -Patholoog informeert gynaecoloog over aantal SLN’s. -Brede locale excisie. -In liezen met een positieve SLN bij vriescoupe een volledige inguinofemorale lymphadenectomie. -Bij problemen ter identificatie van de SLNs eerst verwijderen primaire tumor om radioactiviteit te verminderen en nadien de SLN’s -Definitieve pathologie: (micro) metastase in SLN(‘s): secundaire volledige lymphadenectomie.

Indications for postop radiochemotherapy of the groin and ipsilateral hemipelvis Vulvar Inguinofemoral > 4 cm Ø < 8 mm resection margin Significant lymfatic permeation Macrosc + nodes 2 microscopic nodes
- Slides: 23