Voorkamerfibrillatie Wanneer verwijzen voor ablatie Dr Johan Vijgen

Voorkamerfibrillatie Wanneer verwijzen voor ablatie? Dr. Johan Vijgen Electrofysioloog Hartcentrum Hasselt

Casus 1: • 75 jarige patiënte • Voorgeschiedenis – Diabetes type II – Arteriële hypertensie • Linker ventrikelhypertrofie 1. 5 cm • Behandeling Tenormin, ACE-I • Problematiek: – Sinds 2 weken beperkte malleolaire oedemen – Indruk van dyspnoe bij inspanning • KO: onregelmatig hartritme

t a l b A ? ie

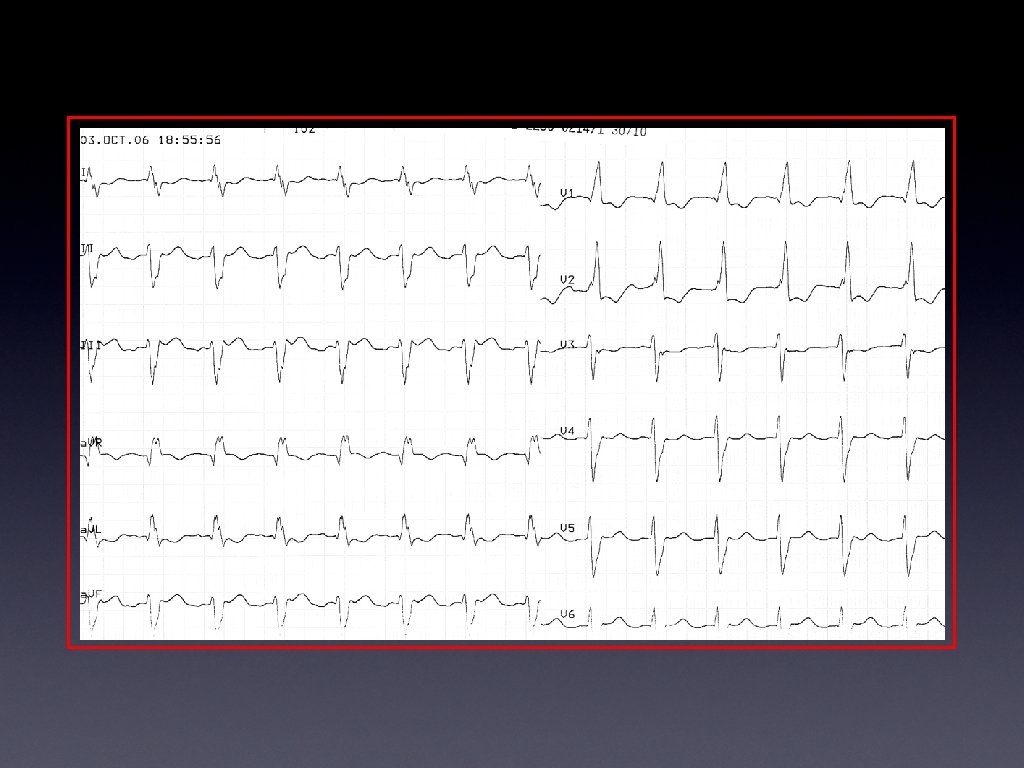
Casus 2: • 82 jarige patiënt • Voorgeschiedenis – Ischemische cardiomyopathie • ACE-I, Beta-blocker, Aldactone, Statine, Marevan – Voorkamerfibrillatie in 2002 en 2004 • Cordarone • Problematiek: – Sinds 3 dagen toenemende dyspnoe – Uitgesproken malleolaire oedemen

Voorkamerflutter A ? e i t a l b

Casus 3: • 42 jarige patiënt • Voorgeschiedenis – Lange-afstand loper – Paroxysmale voorkamerfibrillatie (sinds 2004) – Normale echocardio en cyclo • Problematiek: – Enkele recidieven per week – Duur enkele uren – Begint vaak ‘s nachts – Ondanks rytmonorm, sotalol, flecaïnide

Effect op Levenskwaliteit SF-36 score from Qo. L Questionnaire 120 *p<0. 05 vs. controls 100 88 80 78 60 54* 59 68* 70 85 92 71* 68* 76 81 40 20 0 General health Physical function AF patients (n=152) Dorian P et al. J Am Coll Cardiol. 2000; 36: 1303 -1309. Social function Post MI patients (n=69) Mental health Healthy subjects (n=47) 22

a l b A ? it e

Vraag 1: welke patiënt is de beste kandidaat voor ablatie? 1. De 75 -jarige patiënte: na een succesvolle ablatie hoeft er niet meer geanticoaguleerd te worden! 2. De 82 -jarige patiënt: de flutter resulteert in hartfalen en flutter is vaak refractair aan medicatie! 3. De 42 -jarige patiënt: de paroxysmale VKF heeft een belangrijke impact op zijn leven! 4. Ik stuur ze alle drie.

75 jarige patiënte Diabetes type II Arteriële hypertensie Linker ventrikelhypertrofie 1. 5 cm Behandeling Tenormin, ACE-I Sinds 2 weken beperkte malleolaire oedemen Indruk van dyspnoe bij inspanning Belangrijkste actie? Anti-coagulatie Ablatie > nadien antico stoppen? Neen

82 jarige patiënt Ischemische cardiomyopathie ACE-I, Beta-blocker, Aldactone, Statine Voorkamerflutter Voorkamerfibrillatie in 2002 en 2004 Cordarone Sinds 3 dagen toenemende dyspnoe Minder symptomen? Minder risico op trombi? Medicatie zeer efficient? 3 x NEEN Ablatie eerste keus

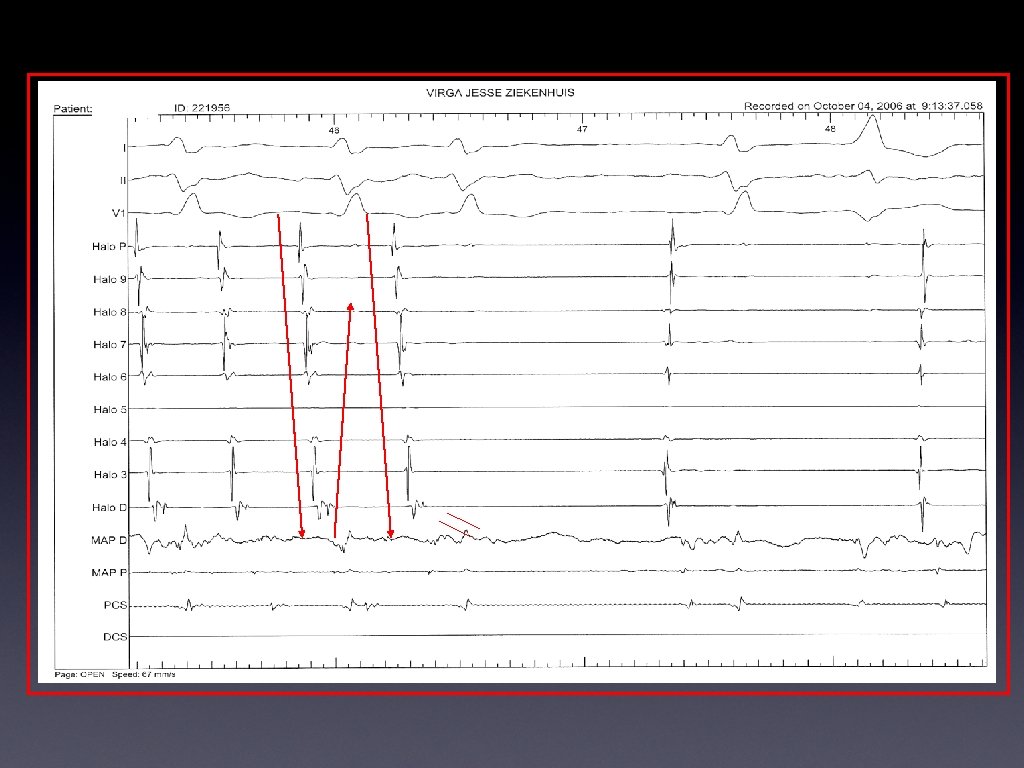
Flutter circuit in het rechter atrium 7 6 8 5 9 P 4 3 CS 2 D

Onderbreking van het fluttercircuit

Ablatie voorkamerflutter • Succes procedure > 90 % • Risico is zeer laag • Indien gemengd voorkamerflutter en -fibrillatie – klinisch succes afhankelijk van medicamenteuze therapie van voorkamerfibrillatie • Indien voorkamerfibrillatie onder invloed van anti-aritmica overgaat naar flutter – klinisch succes onder anti-aritmica > 75% • Anti-coagulatie voor en na ablatie – in functie van CHA 2 DS 2 -VASc score

Alternatief: Ablatie van de AV-geleiding plus Pacing Sinusknoop His

Klinisch Resultaat na His-bundel Ablatie Meta-Analyse Bij slechte linker ventrikel functie: His ablatie plus Biventriculaire Pacing Mark A. Wood, MD; Chris Brown-Mahoney, Ph. D; G. Neal Kay, MD; Kenneth A. Ellenbogen, MD: Circulation 2000, 101, 1138

Casus 3: • 42 jarige patiënt • Voorgeschiedenis – Lange afstand loper – Paroxysmale voorkamerfibrillatie (2004) – Normale echocardio • Problematiek: – Enkele recidieven per week – Duur enkele uren – Begint vaak ‘s nachts – Ondanks rytmonorm, sotalol, flecaïnide

Curatieve behandeling van voorkamerfibrillatie? ? ? Multipele reëntry circuits in beide atria

1994: een mijlpaal voor catheter ablation van voorkamerfibrillatie First 3 ever reported focal AF ablation cases 1994 Haïssaguerre The ‘driver’ hypothesis Diagram of the sites of 69 foci triggering atrial fibrillation in 45 patients. Haïssaguerre M et al. N Engl J Med 1998; 339: 659 -66
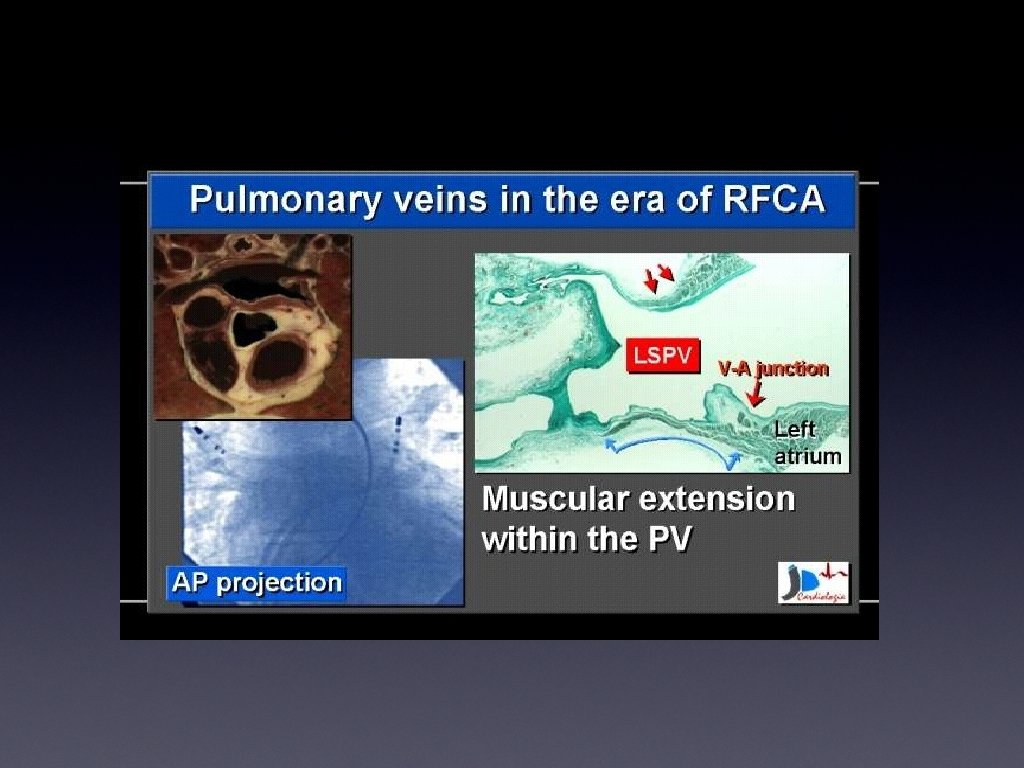

Focal ablation LUPV Circumferential ablation LUPV LLPV 6/13

Risico voor PV stenose!

PV isolatie anno 2002

PV isolatie anno 2002
 • 44% recurrence • after second procedure: 73% success")
Resultaten • Haissaguerre: (Circ 2000) • 44% recurrence • after second procedure: 73% success without drugs • follow-up 4 ± 5 months • Chen: (JCE 2000) • 50 % recurrence • after second procedure: 75 % success • follow-up 8 months • Hasselt: (2002) • 10 patiënten • 50 % succes

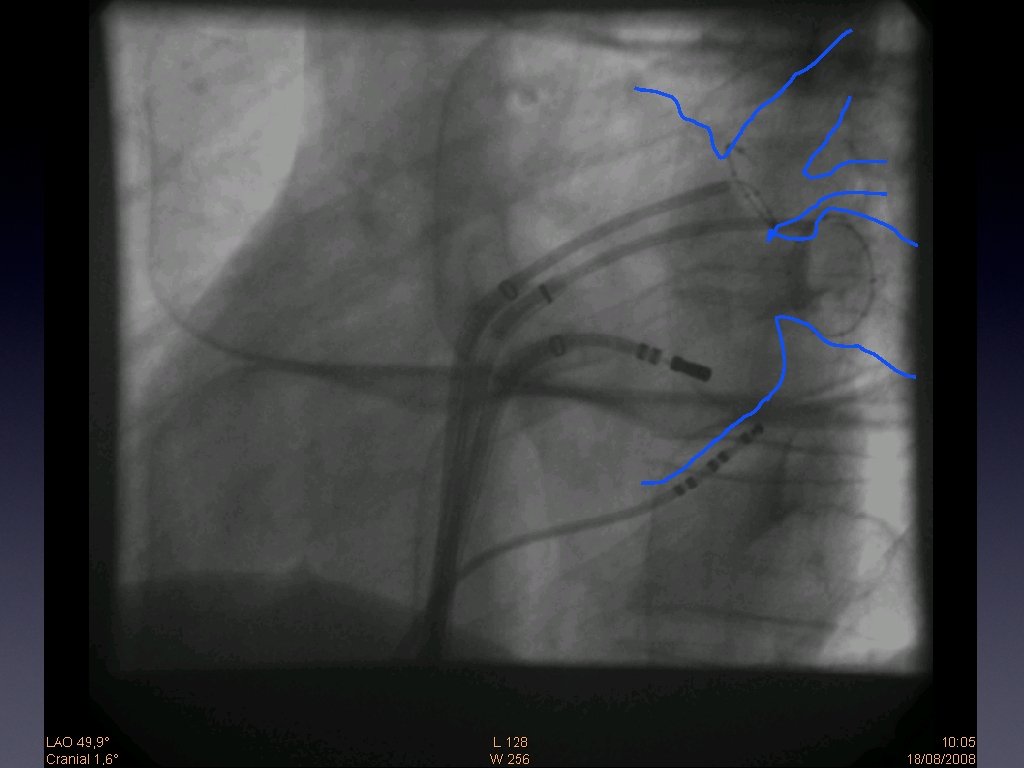
2003: Circumferentiële Ablatie met behulp van 3 D-navigatiesysteem CARTO

Huidige Techniek in Hartcentrum Hasselt Transseptale Punctie CAVE Tamponade

CAVE Thrombi Start Heparine

CAVE Aorta

Veiliger Techniek door CT-integratie

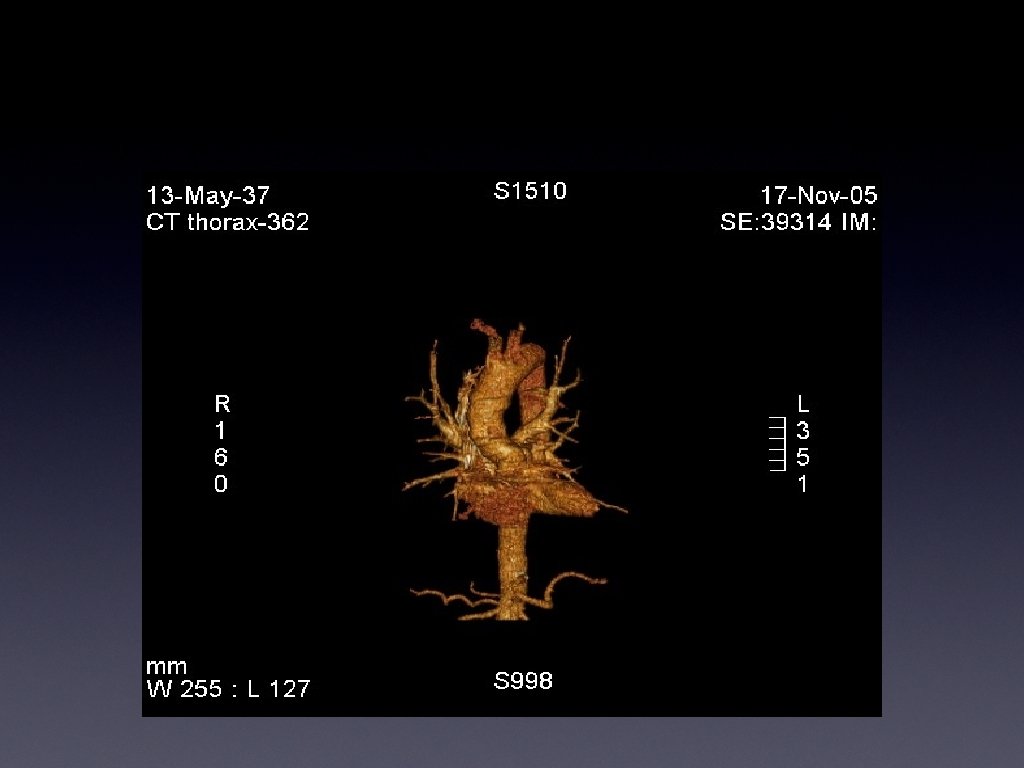

Veiliger Techniek door CT-integratie

Identificatie Hartoortje !

Start 3 D-mapping

Mapping Hartoortje

Rechter Pulmonale Venen

Tagging Slokdarm !!!

Reconstructie Atrium

Samenvoegen CT 3 D

Mapping PVpotentialen

Ready for ablation

Begin ablatie

Isolatie LIPV

Isolatie LSPV inside

Ablatie RPV’s

Ablatie RPV’s

Ablatie onder RIPV

Beginnende isolatie RIPV

Isolatie RSPV

Einde Procedure
")
Efficiëntie Catheter Ablatie voor Par VKF Review of Single Center Observational Studies (1998 -2006) Free of Sympt AF w/o AA Drugs after last Procedure (%) 100 70 -90% Success 90 10 -25% Redo 80 70 60 50 40 30 20 10 0 Haissaguerre % Paroxysmal LAD (mm) Oral Marrouche Arentz Mansour Vasamreddy Karch Pappone Kottkamp Karch Vasamreddy Duytschaever Ouyang 100% 83% 50% 67% 75% 56% 90% 80% 32% 90% 100% 80% N. R. 40 mm 42 mm N. R. 40 mm 41 mm 47 mm ? mm 40 mm 42 mm 47 mm 43 mm 42 mm
 Free")
Efficiëntie van Catheter Ablatie voor VKF Ablation vs Drugs (RCT in drug-resistant patients) Free of AF (%) 100 Ablation P<0. 001 Drugs P<0. 001 90 P<0. 0001 80 70 P<0. 001 60 50 40 30 20 10 0 Pappone et al JACC 2006 N=198, Off drugs Stabile et al EHJ 2006 N=137, Amio Jais et al Ciculation 2008 N=112, Off drugs Wazni et al JAMA 2005 N=70, Off Drugs

Efficiëntie van Catheter Ablatie voor p. VKF A New RCT, now Multi-Centric, The THERMOCOOL AF study! • Multicentre • Randomised (2: 1) • N=167 • Par AF (100%) Sympt and Drug Res AF • FU = 9 M • Freedom of Sx AF( 70% vs 13%) • PVI (Thermocool) • Only FDA approved catheter for AF Wilber et al, JAMA; 2010; 303: 333 -340

Efficiëntie Catheter Ablatie voor VKF Lange Termijn Resultaat? Wokhlu et al: Journal of Cardiovascular Electrophysiology Volume 21, Issue 10, pages 1071– 1078, October 2010

1/2

Time Course and Management of AF

Indications for LA Catheter Ablation

Indications for LA Catheter Ablation

Atrial Fibrillation in Athletes

Conclusies • Ablatie nuttige aanvulling op medicamenteuze therapie: – Recidiverende voorkamerflutter • Ablatie van het fluttercircuit – Moeilijk controleerbaar ventriculair antwoord • His ablatie met pacemakerimplantatie. – Symptomatische focale voorkamerfibrillatie: • Succes percentage van 70% • Indien bereid tot redo: kans op succes 85% • Patiënt op de hoogte van de mogelijke complicaties • Bij patiënten met hoog risico op trombo-embolische complicaties is ablatie geen vervanging voor anticoagulatie

Have we done enough to prevent atrial fibrillation ?
- Slides: 68