VOMITING WITH PREGNANCY Dr Sherif Anis Hebisha Professor

VOMITING WITH PREGNANCY Dr. Sherif Anis Hebisha Professor of Ob/Gyn, Alexandria.

Background Nausea and vomiting are common occurring in 70 -85% of all gravid women. Hyperemesis gravidarum is a severe and intractable form of nausea and vomiting in pregnancy. Severe hyperemesis requiring hospital admission occurs in 0. 3 -2% of pregnancies It is a diagnosis of exclusion and may result in weight loss; nutritional deficiencies; and abnormalities in fluids, electrolyte levels, and acid -base balance.

The peak incidence is at 8 -12 weeks of pregnancy, and symptoms usually resolve by week 20. Uncomplicated nausea and vomiting of pregnancy is generally associated with a lower rate of miscarriage, but hyperemesis gravidarum may affect the health and well-being of both the pregnant woman and the fetus.

Causes of vomiting in pregnancy Simple vomiting Hyperemesis gravidarum Vomiting due to obstetrical complication; 1. 2. 3. a) b) c) d) e) f) Acute yellow atrophy of the liver Pre-eclampsia Red degeneration of fibroid Accidental hge Rupture uterus Pyelonephritis

Accidental Hge

Uterine fibroids

Fibroid with pregnancy

Pre-eclampsia

4. Vomiting due to associated conditions: a. twisted ovarian tumor b. acute appendicitis c. gastritis d. cholecystitis e. cerebral tumors

Ovarian cyst with pregnancy

Twisted ovarian cyst

Simple vomiting in pregnancy It is a feeling of nausea or vomiting on getting up in the morning during the first trimester of pregnancy Etiology 1. Toxemic theory 2. Neurosis 3. Vitamin B 1, 6 deficiency 4. Hormonal 5. Allergic

Treatment Assurance Diet … dry toast, low fat and protein and high CHO diet Vitamin B 6 supplement Anti-emetics …. Meclozine 25 mg

Hyperemesis gravidarum Ø 1. 2. 3. 4. Excessive vomiting in early pregnancy affecting the general condition producing loss of weight, dehydration, starvation ketosis and hypokalemia Theories of hyperemesis: Cytokines: Inc. TNF α, IL-4. Increased cell free DNA in maternal plasma Genetics: Twins, siblings, ethinic, inhereted glycoprotein receptor defect Embryo protection theory

Risk Factors The cause of severe nausea and vomiting in pregnancy has not been identified. Hyperemesis may have a genetic component, as sisters and daughters of women with hyperemesis have a higher incidence. Hyperemesis is also associated with hyperemesis in prior pregnancy, female gestation, multiple gestation, triploidy, trisomy 21, current or prior molar pregnancy, and hydrops fetalis.

Nuchal translucency

Risk Factors Women with history of motion sickness, migraine headaches, psychiatric illness, pregestational diabetes, being underweight pregestation, hyperthyroidism, pyridoxine deficiency, and gastrointestinal disorders are also at an increased risk. Some studies have suggested that Helicobacter pylori infection may play a role in hyperemesis. Cigarette smoking and maternal age older than 30 years appear to be protective.

Race Hyperemesis patients are more likely to be nonwhite. Age Patients younger than 30 years are more likely to experience hyperemesis.

Hydrops fetalis

Vesicular Mole

Vesicular mole

Pathology I. Electrolyte changes a. Reduced extracellular fluid volume b. Decreased plasma volume c. Reduced blood sodium and chloride d. Raised blood urea

Metabolic changes: a. CHO def. glycogen depletion incomp. consumption of fat Inc acetone and acetic acidosis b. Necrosed liver cells are unable to de-aminate proteins Inc urea

Changes in different organs: Liver : fatty degeneration & necrosis Kidneys : toxic nephrosis , tubular degen.

Changes in different organs Heart : muscle atrophy Brain : congestion & peticheal hge.

Vicious circle Vomiting Acidosis Starvation Liver degeneration

Clinical picture: Symptoms: Excessive vomiting Constipation & colics Oliguria due to dehydration Fainting and easy fatigability Drowsiness and visual blurring

Signs: Progressive loss of weight Tachycardia, fever Low blood pressure Dehydration, sunken eyes, dry tongue, sordes on lips � Decreased skin turgor � Postural changes in blood pressure (BP) and pulse Enlarged tender liver

Diffrential Diagnosis Appendicitis, Acute Ovarian Torsion Cholecystitis and Biliary Colic Pancreatitis Diabetic Ketoacidosis Preeclampsia Gastritis and Peptic Ulcer Disease Urinary Tract Infection Gastroenteritis Hepatitis Obstruction, Small Bowel Pyelonephritis Molar pregnancy Pseudotumor cerebri Acute fatty liver of pregnancy


Investigations Urine: 1 - oliguria, 2 - increased albumin, 3 - decreased chlorides, 4 - increased specific gravity, 5 - bile pigments and salts, 6 - urinary casts and acetone.

Blood: . 1 - heamoconcentration, 2 - increased urea, 3 - decreased chlorides, 4 - hypokalemia , Normal serum potassium is 3. 5 to 5. 5 m. Eq/L. Muscle weakness and flaccid paralysis may be present. Patients may have depressed or absent deep-tendon reflexes. Hypoactive bowel sounds may suggest hypokalemic gastric hypomotility or ileus. 5 - hypoglycaemia. The normal range for blood sodium levels is 135 to 145 milliequivalents per liter (m. Eq/L). Fundus examination: retinopathy

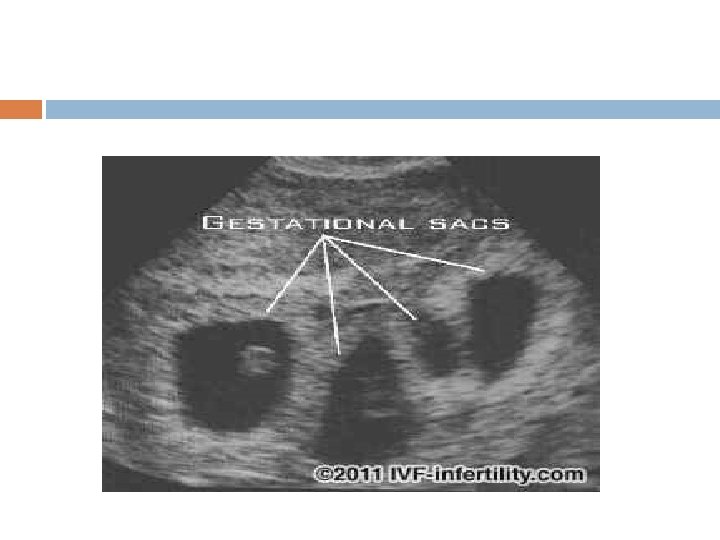
• Ultrasound Twin pregnancy Vesicular mole

Polyhydraminos
. Pneumothorax Mallory weiss tear of the")
Complications Wernicke’s encephalopathy (diplopia, nystagmus, disorientation, confusion, coma). Pneumothorax Mallory weiss tear of the oesophagus Oesophageal rupture Splenic avulsion Acute tubular necrosis Cardiac dysfunction

Treatment Moderate cases: home treatment. Severe cases: hospitalization. Bowel regulation. Emotional support. Fluid therapy. Proper diet Drug therapy Observation and follow up

The American College of Obstetrics and Gynecology recommends that first-line treatment of nausea and vomiting of pregnancy should start with pyridoxine (vitamin B-6) with or without doxylamine Pyridoxine in combination with doxylamine 10 mg, the active ingredient in many over-thecounter sleep agents, has been shown in randomized, placebo-controlled trials to have a 70% reduction in nausea and vomiting
, while pregnancy Class B, has become the most common parenteral and")
Ondansetron (Zofran), while pregnancy Class B, has become the most common parenteral and oral antiemetic used in US emergency departments due to its efficacy, and it has become the first choice in hyperemesis in the last several years. It is a serotonin antagonist and is dose responsive. Starting dosage is 4 mg, either IV or PO, and that dose may be repeated every 15 -30 minutes until symptoms improve.

Other typical antiemetics such as promethazine 12. 5 -25 mg IV or PO every 4 hours or prochlorperazine 25 mg rectally every 12 hours are also acceptable second-line agents.

Corticosteroids have a possible benefit in the treatment of hyperemesis gravidarum. Steroids have been considered a last resort in patients who will require enteral or parenteral nutrition due to weight loss. The most common regimen is methylprednisolone 16 mg, orally or intravenously, every 8 hours for 3 days. Patients who do not respond within 3 days are not likely to respond.

For those who do respond, the course may be tapered over 2 weeks. Some recent studies have demonstrated an association between oral clefts and methylprednisolone use in the first trimester. The current recommendation is that corticosteroids be used with caution and avoided before 10 weeks' gestation.

Ginger is a common remedy for nausea and vomiting in pregnancy. Ginger capsules of 250 mg taken 4 times a day have been demonstrated to be effective against nausea and vomiting of pregnancy as well as hyperemesis when compared with placebo, without evidence of significant side effects or adverse effects on pregnancy outcomes

Practitioners of traditional Chinese medicine believe that stimulation of acupuncture point P 6 can relieve nausea. Acupressure can be used as an alternative or complement to medications Sea Band is an easy over-the-counter product that stimulates the P 6 site.

Termination of pregnancy 1. 2. 3. 4. No improvement under Treatment Progressive vomiting and weight loss Temperature>38 Pulse >100 Persistant hypotension Progressive oliguria, anuria, albuminuria, ketonuria, bile salts and pigments High blood urea, Jaundice Optic neuritis and retinopathy
- Slides: 46