Vomiting Diarrhoea Abdominal Pain Fluid Therapy Department of

Vomiting, Diarrhoea, Abdominal Pain & Fluid Therapy Department of Paediatrics CUHK

Vomiting l vomiting – forceful ejection of gastric contents – often preceded by nausea and retching l possetting – gentle expulsion of gastric contents with swallowed air (“wind”) l regurgitation – similar to possetting, but larger loss l retching – laboured rhythmic respiratory activity that precedes vomiting

Mechanism of vomiting Vomiting process • patent upper GI tract • retro-peristalsis • lower esophageal sphincter relaxation • contraction of abdominal muscles and diaphragm

Causes of Vomiting infection/inflammation • gastroenteritis • viral • bacterial • toxin • immunological • cow-milk • coeliac • food allergy • inflammatory • appendicitis • mesenteric adenitis CNS irritation • infection • raised ICP • drugs / poisons • metabolites Incompetent LES • possetting • reflux • hiatus hernia GI obstruction • pyloric stenosis • intussusception • volvulus • strangulated hernia • Hirschsprung • tumour • post-operative ilieus
 and change in character of")
Diarrhoea l Diarrhoea: increase in frequency (> 3 times) and change in character of stool (volume and liquidity) l Lead to rapid dehydration and progressive acidosis l Acute - within 2 weeks l Chronic or persistent - beyond 2 weeks l WHO: 2. 6 episodes/child/year, global mortality 3. 3 million/year

Infective gastroenteritis

Acute gastroenteritis l Morbidity in developed world, yet mortality in developing world l Complicated in developed world with secondary lactase deficiency l Complicated in developing world with recurrent episodes and malnutrition, like deficiency of zinc, vitamin A etc, l Especially affecting children < 2 years

Infective causes of diarrhoea and vomiting Viruses Rotavirus Adenovirus Coronavirus Astrovirus Calcivirus Parvovirus Echovirus Bacteria Enteroinvasive E. coli Camphylobacter jejuni Salmonella sp. Shigella sp. Vibrio cholera Yersinia enterocolitica Protozoa Giardia lamblia Crytosporidium Entamoeba histolytica Malaria Bacterial toxins Enterotoxic E. coli Staphylococcus aureus Bacillus cereus Clostridium difficile
, Shigella (neurotoxin), Yersinia, Campylobacter")
Bacterial Gastroenteritis l Salmonella, E coli (EPEC, EIEC, EHEC, VTEC-0157), Shigella (neurotoxin), Yersinia, Campylobacter l Adherence and invasion of bacteria to gut structures l Bloody diarrhoea, Fever, Tenesmus, Severe or persistent symptoms l Antibiotic use, Clostridium(toxin is common in healthy newborn)

Cholera l cause secretory diarrhoea l enterotoxin production leading to generation of intracellular c. AMP (adenyl cyclase) l result in stimulation of the chloride channel leading to fluid and electrolytes secretion l could also cause increased production of prostaglandins l absorption of fluid and e- remains intact

Virus Gastroenteritis l Rotavirus attacks the villus epithelium of the small intestine l Norwalk virus - vomit l Enteric adenoviruses l increase in epithelial renewal with crypt proliferation, interfering the process of maturation l repair takes 4 - 5 days, affected by chronic proteincalorie malnutrition

Rotavirus gastroenteritis l Most common cause in infants and young children (6 - 12 months), occurs in winter l Within two days of exposure, low grade fever, anorexia, & vomiting lasting up to 48 hours. Watery diarrhea and cramps follow l Highly infective, resistant to drying and chlorine in tap water. Nosocomial outbreaks occur in hospital and nurseries l Fecal-oral transmission

Rotavirus gastroenteritis l Infect the villi of small intestine, causing damage to transport mechanisms, secondary lactase deficiency and malabsorption l Local Ig. A response, no life-long protection l Diagnosis by viral antigen detection l Self-limiting disease with complete recovery l Prevention by improving overall standard of nutrition and hygiene (handwashing, disposal of diapers), ? oral vaccine

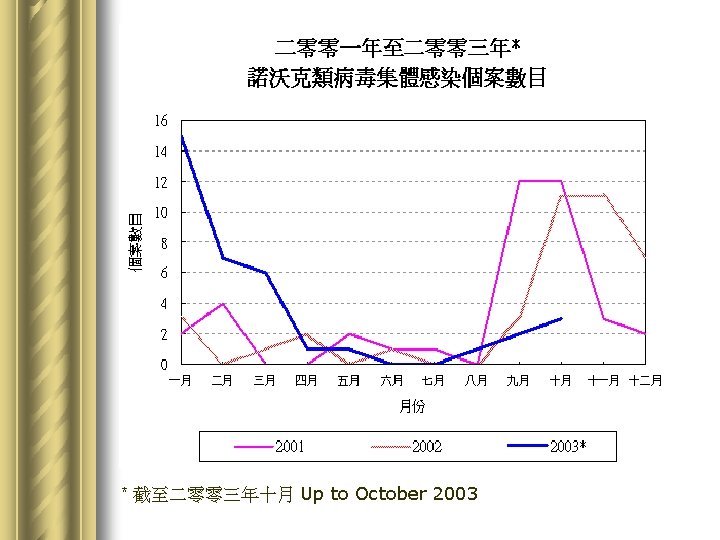
Norwalk / Norwalk-like / Norovirus l Norwalk virus was named after the strain that was responsible for an outbreak of gastroenteritis in a school in Norwalk, Ohio, USA l Recently approved name: Norovirus, a RNA virus l More common during cooler months l As of November 17, there were 41 reported cases of viral gastroenteritis caused by Norwalk-like virus, affecting about 1, 000 persons and occurring in institutions like schools, child care centres and homes for the elderly.

二零零三年* 受諾沃克類病毒影響人數 Number of Persons Affected of Norwalk-like Disease 2003* 中學 Secondary school 4% 醫院 Hospital 1% 小學 Primary school 19% 安老院舍 Elderly home 幼稚園 Kindergarten 4% 幼兒中心 Child care centre 48% 10% 院舍 Institutions 9% *截至二零零三年十月。 *Up to October 2003 家居 Home 5%

Norovirus gastroenteritis l Incubation 1 - 2 days l Usually self-limited, lasts 1 - 10 days l Symptoms • Vomiting • Diarrhoea • Fever • Abdominal cramps • Headache

Clinical Approach to a child who presents with vomiting or diarrhoea

History: Vomiting l Onset • Present since birth ? • Present since weaning ? • Present since introduction of new food? • Sudden or gradual ? l Vomit • Size, frequency and timing to feed • Undigested food ? bile ? blood ? coffee-ground ?

History: Diarrhoea l Onset • Sudden or gradual ? l Stool • Volume, frequency and timing to feed • Loose, watery, rice watery • Blood, mucus, steatorrhoea

History: l Associated symptoms • Abdominal pain / Abdominal distension • Fever • Change in appetite / feeding habit • Weight loss ? or gain ? • General: playfulness, activities, urine output l Social history • Family members having vomiting / diarrhoea • Recent traveling

Examination l Full examination is necessary in all children l General examination • Activity • Nutritional status • Weight and Height (and compare with previous) • Temperature • Anaemia • Jaundice • Degree of dehydration • Cleft palate • Neurological

Mild Moderate Severe Body weight <5% 5 -10% > 10% General Appearance Thirsty, Alert Thirsty, restless or lethargic Drowsy, cold, sweating Tears Present Absent Anterior Fontanelle Normal Sunken Very sunken Eyes Normal Sunken Very sunken Tissue Turgor Normal Absent Moist Dry Very Dry Pulse Normal Rapid, weak, may be impalpable Urine flow Normal Reduced, concentrated Oliguria Blood pressure Normal or low Low, may be unrecordable Fluid deficit 50 ml/kg 60 -90 ml/kg 100 ml/kg Mucous Membranes

l In hypertonic dehydration, signs not prominent because of intracellular dehydration; skin of doughy consistency with abnormal behaviour

Examination l Abdomen: Inspection • Distension • Constipation • Gastroenteritis • Obstruction / Ileus • Coeliac Disease • Surgical Scar

Examination l Abdomen: Palpation • Local tenderness • Generalized tenderness • Guarding and rebound tenderness • Peritoneal irritation • Masses • Organomegaly • Pyloric mass • Sausage shaped mass • Hernial orifices • Genitalia

Examination l Abdomen: Auscultation • Bowel sounds • Normal • Hyperactive: irritation, obstruction • Diminished, absent: paralytic ileus l Abdomen: Rectal examination • Anal fissures • Sphincter • Faeces • Blood • Masses

Investigations l Ordered according to index of suspicion • Examine stool for consistency, blood, mucus, and steatorrhoea • Stool for bacterial culture and virus isolation Positive yield ~50% • Commonest: rotavirus • Commonest bacterial: Salmonella • Stool for Clostridial difficile toxin • Blood for cell counts, U&Es, culture

Investigations • Test feed for infant 2 to 10 weeks • Examine urine for RBC, WBC and organism under microscope, urine for culture • AXR: Supine, Erect for intestinal obstruction • USG abdomen

Treatment l Rehydration fluid and electrolytes • Oral glucose-electrolyte solution • Intravenous glucose-electrolyte solution • Nutritional treatment - continuation of breast feeding (lactadherin), or formula feeding

Principles of fluid replacement : volume required = maintenance + deficit + ongoing loss

Daily fluid requirement Fluid First 10 kg Second 10 kg After first 20 kg 100 ml/kg/day 50 ml/kg/day 20 ml/kg/day Increase by 10% per degree Celcius rise in body temperature Electrolytes Sodium Potassium 3 mmol/kg/day 2 mmol/kg/day For a 25 -kg boy Daily fluid requirement for a 25 -kg boy = 1000 ml + 500 ml + 100 ml = 1600 ml Daily Na requirement = 75 mmol Daily K requirement = 50 mmol

Fluid deficit calculation Volume depleted = estimated % of dehydration x body weight For a 25 kg boy with 10 % dehydration Volume deficit (1 L water = 1 kg) = 10% x 25 kg = 2. 5 L

Fluid ongoing loss l Most difficult l Measure stool output and volume of vomitus

Oral versus intravenous fluid replacement therapy

AAP Practice Parameter 1996 l ORS is the preferred treatment for fluid and electrolyte losses caused by diarrhoea in children who have mild to moderate dehydration l Use of cola, fruit juice and sports beverages is not recommended – Inappropriate electrolyte content – Too much carbohydrate

ORS l Commercially available ORS contain 45 -50 mmol/l of sodium – Best suitable for maintenance – Can also be used in mild to moderate dehydrated otherwise healthy children – Taste better than the saltier solution l WHO recommended ORS – High sodium content 90 mmol/l – Suitable for secretory diarrhoea eg. Cholera

ORS Therapy in mild to moderate dehydration l 50 -100 ml/kg ORS to be given over a 4 -hour period l Replacement of stool (10 ml/kg for each stool) and vomitus will require adding appropriate amounts of solution to the total l Administering in small but frequent amounts – 10 ml every two minutes = 500 ml over 4 hours l Labour intensive, time consuming

Intravenous fluid therapy l Although oral rehydration is encouraged, clinician must be prepared to administer IV fluids who do not respond to oral regimen l Severely dehydrated or who are in a state of shock must receive immediate and aggressive intravenous fluid therapy
 10 -20 ml/kg 0. 9% Na.")
Phase I: Treat shock (0 - 30 minutes) 10 -20 ml/kg 0. 9% Na. Cl Reassess Improved Phase II: Initial Rehydration (½ - 8 hours) No Change Measure plasma electrolytes Calculate fluid deficit and maintenance Initial replacement with saline-dextrose solution Half the calculated fluid deficit plus maintenance Phase III: Continued Replacement (8 - 24 hours) Review plasma electrolytes and fluid status Replacement with saline-dextrose solution Half the calculated fluid deficit plus maintenance
![Sodium replacement l Sodium deficit in mmol required = (140 - [Na+] x 0.](http://slidetodoc.com/presentation_image_h2/7256f1b12dc9d596b2c2cf23497d2d55/image-41.jpg "Sodium replacement l Sodium deficit in mmol required = (140 - [Na+] x 0.")
Sodium replacement l Sodium deficit in mmol required = (140 - [Na+] x 0. 65 x body weight in kg) • 0. 65 is the volume of distribution of Na l Sodium replacement = sodium daily requirement + sodium deficit l If due to water intoxication (iatrogenic, SIADH) • Restrict fluid
")
Treatment of metabolic acidosis For full correction of acidosis, Na. HCO 3 required (mmol) = Base deficit x body weight x 0. 3 In most cases, metabolic acidosis is self-corrected once dehydration corrected and hence effective circulation volume restored In rare situation, half of the calculated required Na. HCO 3 may be given: watch out for Na overload and pulmonary oedema

Hypertonic dehydration l Difficult to assess degree of dehydration, unless the child in clinically shock (>10% dehydration) l The plan – Fluid resuscitation 10 -20 ml/kg Na. Cl over first 1 hr – replace total fluid deficit plus maintenance slowly over 48 -72 hours – To lower serum sodium slowly: 10 mmol/L/day l Rapid correction may cause cerebral oedema

Monitor l l l l Body weight Vital signs, heart rate, blood pressure, respiratory rate Subsidence of signs of dehydration Input and output charts Continuous loss Serum electrolytes In severe cases blood glucose, blood gases, osmolality

Antibiotics in special circumstance l l l Salmonella GE in infant Shigella with trimethoprim-sulfamethoxazole Campylobacter with erythromycin Cholera with tetracycline Amoebic dysentery - giardiasis (metronidazole) NB: drug resistance, promote carrier state, worsen the course of diarrhoea

Refeeding l Children who have diarrhoea and are not dehydrated should continue to be fed regular diet l Children who require rehydration should be fed regular diet as soon as they have been rehydrated l Early feeding of regular diet does not worsen the course or symptoms of mild diarrhoea and may reduce the duration of diarrhoea modestly

Refeeding l Avoid fatty foods and foods high in simple sugars l Rice, wheat, potatoes, bread and cereals (complex carbohydrate), lean meats, yogurt, fruits and vegetables are usually well tolerated l Most children who have diarrhoea will tolerate fullstrength milk l Lactose-free formula may be used if secondary lactase deficiency is suspected

Antidiarrhoeal compounds l l l Decrease stool water and electrolyte losses Change toward more formed stool Relieve discomfort False sense of security Delaying more effective therapy Generally not recommended

Drugs that alter intestinal motility l l l Loperamide Decreases transit velocity Increases the ability of gut to maintain fluid Reduces stool losses, shortens the course of diarrhoea Associates with serious adverse effect – Lethargy, ileus, respiratory depression and coma – Death has been reported

Drugs that alter secretion l l l Bismuth compounds, eg. Bismuth subsalicylate Inhibit intestinal secretion Modest beneficial effects Dose of every 4 hours for 5 days Theoretical risk of Reye syndrome from salicylate absorption

Drugs that absorb fluid and toxins l l l Kaolin-pectin, fiber, activated charcoal, attapulgite Adsorb bacterial toxins Bind water Serious toxic effects are not a concern Evidence of their efficacy has been contradictory

Agents that alter intestinal microflora l Patients with diarrhoea undergo reduction fecal flora, which leads to increased water losses l Lactobacillus sp. – Alter the bacterial colonization of the gut therapeutically l Toxic effects are not a concern l However efficacy of lactobacillus-compounds in treating diarrhoea yet to be demonstrated

Treatment outcome/evaluation l l l hospitalization or not extent of investigation effectiveness of rehydration (IV <=> PO) use of antimicrobials relief of symptoms - frequency of stools, duration of diarrhoea, weight gain l prevention strategy • Public health measures - sanitation • Food preparation and storage • Promotion of breast feeding

Other common paediatric gastrointestinal conditions

l l l Gastro-oesophageal reflux Pyloric stenosis Cyclic vomiting Chronic diarrhoea Constipation Acute abdominal pain

Gastro-oesophageal reflux l Small, effortless vomits of semi-digested milk soon after feeding l Common in infants because of • immature lower oesophageal sphincter • short intra-abdominal length of oesophagus l Usually resolve by 1 year old l Usually mild but severe cases with complications: • pulmonary aspiration • oesophagitis, peptic stricture • failure to thrive, feeding problems

Gastro-oesophageal reflux l Investigation – usually not required – 24 -h oesophageal p. H monitoring • contrast study

Gastro-oesophageal reflux l management • often requiring no treatment • mild: positioning at 30° head-up prone & thickening agent • drugs enhancing gastric emptying • H 2 antagonists • fundoplication

Pyloric Stenosis l l hypertrophy of pylorus presented between 2 and 7 weeks of age M: F = 4: 1 presentation • large, non-bilious, projectile vomiting after each feed • dehydration, weight loss

Pyloric Stenosis l visible peristalsis l “olive”-shaped mass at right upper quadrant

Pyloric Stenosis l Investigation • ultrasonography & contrast study elongated pyloric canal antrum thickened pyloric muscle

Pyloric Stenosis l Management • fluid resuscitation • electrolyte correction • hypochloraemic alkalosis with hypokalaemia • Ramstedt’s pyloromyotomy

Persistent & Chronic Vomiting l CNS: raised intracranial pressure • early morning vomiting • headache worsen on lying down l Appendicitis • uncommon before 3 years old • atypical presentation in retrocaecal and pelvic appendices

Persistent & Chronic Vomiting l Cyclical vomiting • psychogenic, with stressful factors • of school age • prodromal symptoms: pale, withdrawn • associated with migraine l Anorexia or bulimia nervosa – adolescent – deranged body image – weight-fear – induced vomiting

Chronic Diarrhoea Birth to 6 mo Infection Secondary lactose deficiency Persisting diarrhoea Cow’s milk intolerance Other food intolerance Cystic fibrosis In-born errors Antuoimmune enteropathy Surgery

Chronic Diarrhoea 6 mo to 1 yr 1+ years 10+ years Infection Coeliac disease Giardia lamblia Surgery Post-infection Coeliac disease Giardia lamblia Inflammatory bowel disease

Chronic diarrhoea l Postinfectious diarrhoea - persistence of diarrhoea and failure to gain weight more than 7 days after admission l Due to disaccharide intolerance(brush-border damage), cow milk protein hypersensitivity(� -lactoglobulin), persistent infection l Managed by soy-base formula, lactose-free formula, or semielemental diet

Chronic nonspecific diarrhoea l l l l “Toddler” diarrhoea affecting children 6 months to 2 years self-limiting pass 4 - 10 loose stool per day may be intermittent, explosive May contain undigested food Negative stool culture and reducing substances growth and development normal

Acute abdominal pain: “Does the child require emergency surgery? ” l Signs of peritonism, appendicitis – Fever, localized tenderness, guarding, rebound tenderness, absent bowel sounds – The younger the child the more vague the signs l Signs of obstruction – Vomiting, abdominal distension, high pitch bowel sounds, empty rectum l Gastrointestinal bleeding – Haematemesis, bloody stool, “Current-jelly” stool, malaena

Require early surgical referral Abdominal cause but does not require immediate surgical referral Systemic cause Appendicitis Peritonitis Intussusception Volvulus Strangulated hernia Trauma GI Bleeding Gastroenteritis Infantile colic Ingestion Constipation Peptic ulcer Pancreatitis / mumps Cholecystitis / cholangitis Urinary tract infection Nephrotic syndrome Hepatitis Dysmenorrhoea Any febrile illness but especially ENT infection Lower lobe pneumonia Abdominal migraine Diabetic ketoacidosis Sexual abuse Porphyria Lead poisoning Henoch Scholein purpura

- Slides: 71