Vocal cord paralysis Dr Deekshith RM 15102019 Vocal



Motor supply Cricothyroid – superior laryngeal nerve (external) All other")


left 75% b)right 15% c)")















 U/L PALSY Paralyzed Cord in cadaveric position – Hoarseness Glottic incompetence Hoarseness,")


 Chest X-Ray PA view")




















- Slides: 54
Vocal cord paralysis Dr. Deekshith RM 15/10/2019
Vocal cords are twin infoldings of mucous membrane which stretches horizontally across the larynx Between vocal process of arytenoids and middle of thyroid cartilage Functions 1. Protection of lower airways 2. Phonation 3. Respiration adduction abduction
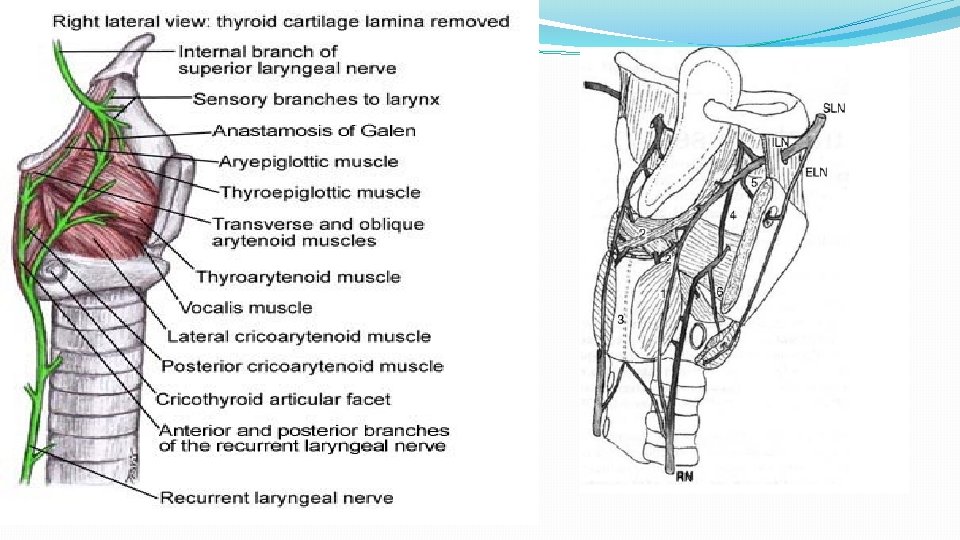
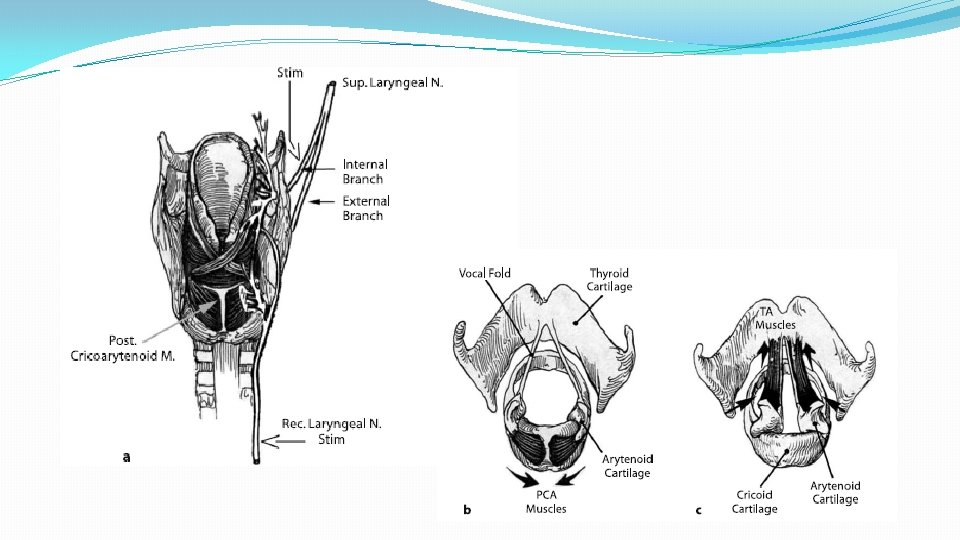
Muscles of vocal cord Abductor – posterior cricoarytenoid Adductor – lateral cricoarytenoid, inter arytenoid, thyroarytenoid (external part) Tensors – cricothyroid, vocalis (internal part of thyroarytenoid).
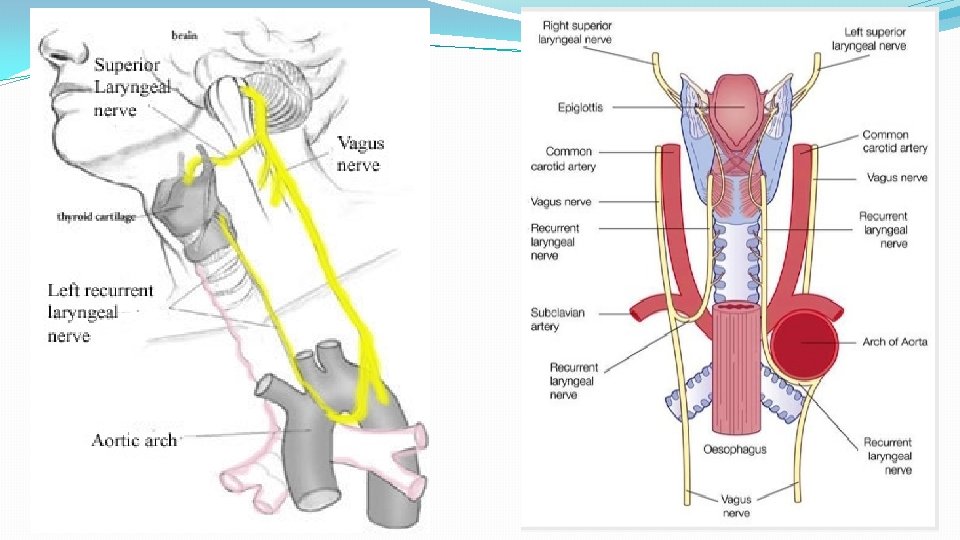
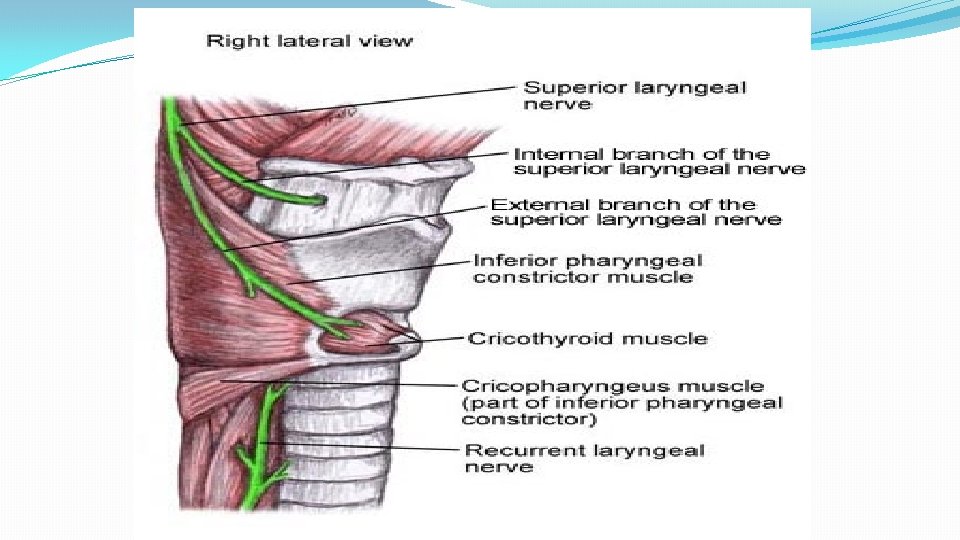
NERVE SUPPLY OF LARYNX A)Motor supply Cricothyroid – superior laryngeal nerve (external) All other muscles – recurrent laryngeal nerve B) Sensory supply Above vocal fold – superior laryngeal nerve (internal) Below vocal fold – recurrent laryngeal nerve. BOTH ARE BRANCHES OF VAGUS NERVE
Specific learning objective Describe the course of vagus nerve, recurrent laryngeal nerve and superior laryngeal nerve Define vocal cord paralysis Classify vocal cord paralysis Describe in brief the clinical feature of each type of vocal cord paralysis Enlist the investigations for an idiopathic vocal cord palsy Describe management of unilateral vocal cord palsy Describe the management of bilateral vocal cord palsy Enlist the surgical options for bilateral adductor palsy Brief about congenital vocal cord palsy Summary
Vocal cord palsy is a sign of disease and not a diagnosis
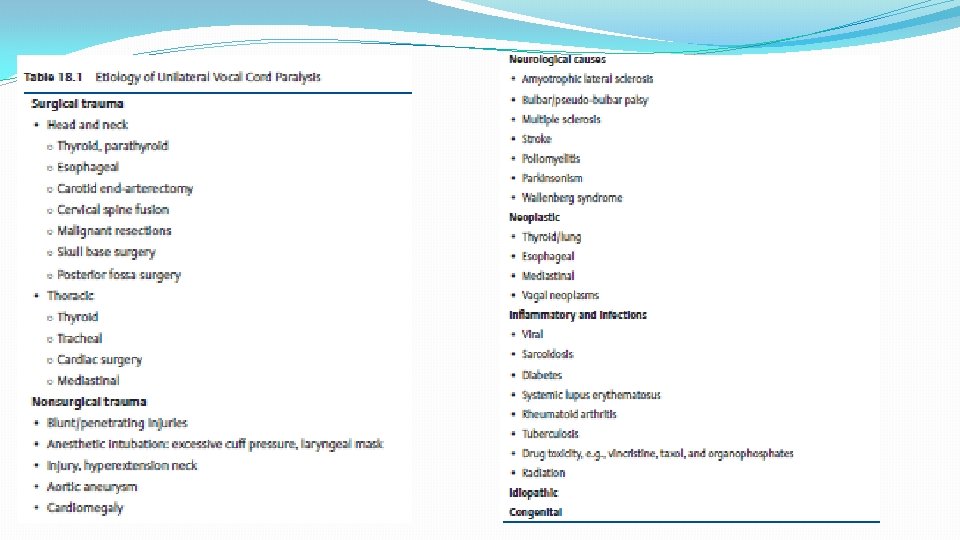
Classification Of Vocal Cord Palsy Unilateral or bilateral RLN a)left 75% b)right 15% c) bilateral 10% a)abductor b) adductor SLN Combined – RLN+SLN
CLASSIFICATION Supranuclear palsy Nuclear PALSY High vagal palsy Low vagal palsy / Recurrent laryngeal nerve palsy Systemic causes – Diabetes, Diphtheria, Typhoid, Streptococcal, Viral or Lead poisoning Idiopathic – 30%
Supra Nuclear palsy Above nucleus ambigous Rare Bilateral symmetric lesion causes vocal cord palsy Spastic paralysis of cord and vocal cords are widely abducted Etiology : - Tumors of posterior fossa , basal meningitis.
Nuclear palsy At the level of nucleus ambigous Associated with other lower cranial nerve palsy (9, 11, 12) MC etiology is wallenberg syndrome
High Vagal Palsy Lesions at the level of jugular foramen below nucleus. Lesion in skull at the exit from jugular foramen or para pharyngeal space. RLN, SLN & pharyngeal branches involved.
Clinical features Laryngeal & pharyngeal paralysis Intermediate position of paralyzed cord -aspiration Swallowing affected Soft palate droops on ipsilateral side and does not rise on phonation Absent gag reflex
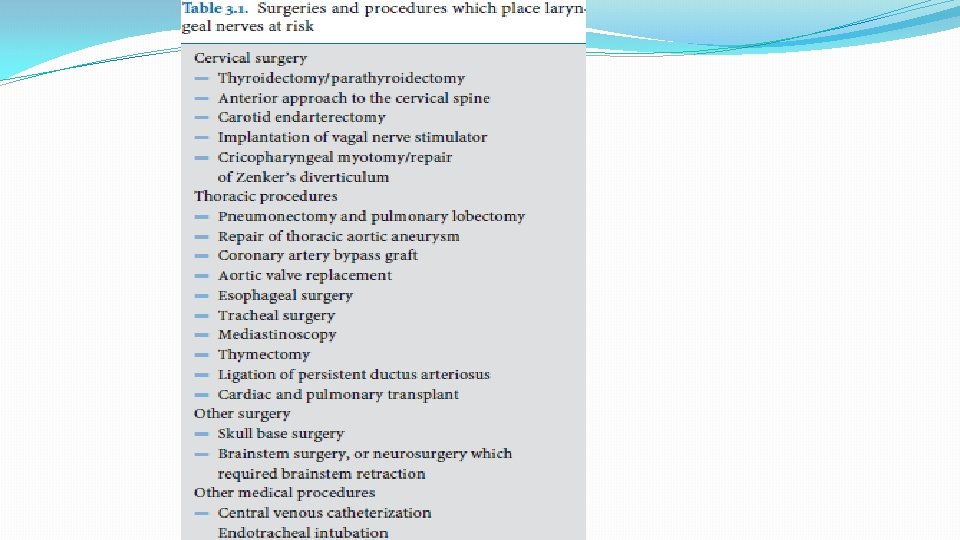
Thyroidectomy is the most common iatrogenic cause of vocal cord palsy 2 important triangles for identifying RLN & SLN JOLLS triangle for SLN BEAHR’S triangle for RLN
POSITIONS OF VOCAL CORD
Unilateral RLN palsy Ipsilateral paralysis of all muscles except the cricothyroid and inter arytenoid Vocal folds median /paramedian position Semon’s law/ Wagner or Grossman theory
Semons law In all progressive organic lesions, abductors fibres of RLN, which are phylogenetically newer are more susceptible and thus first to be paralyzed compared to adductor fibres. Nerve supplying abductors are in periphery of RLN Muscle bulk for abductor is less, more susceptible Phylogenetically, main function of larynx is protection, so adductor function is maintained
Wagner’s and Grossman Theory In isolated paralysis of RLN , cricothyroid muscle(receives innervations from SLN) keep vocal cord in paramedian position due to its adductor function
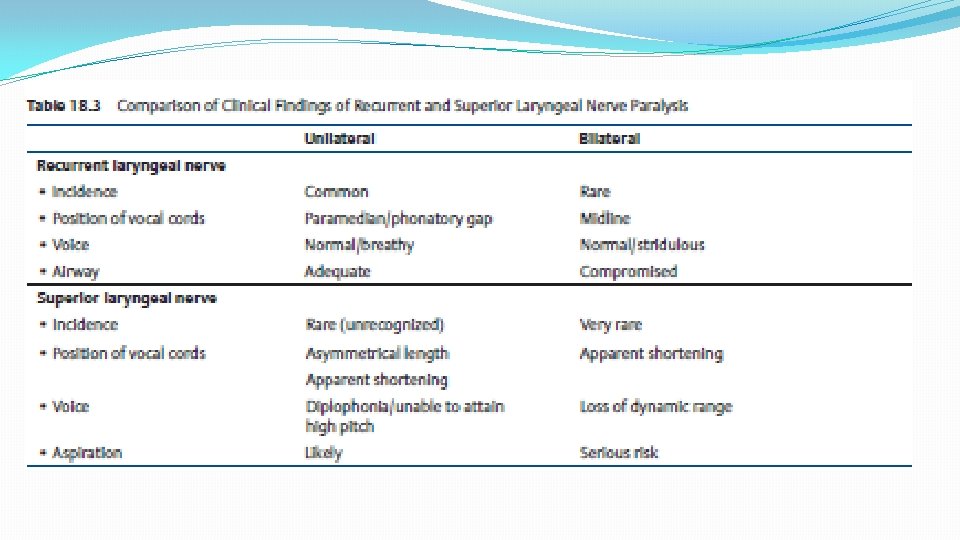
Unilateral RLN palsy Slight hoarseness and voice fatigability Voice improves with compensation by normal cord No aspiration or respiratory obstruction Cord in paramedian position Normal arytenoid crosses midline
BILATERAL RLN PALSY Most common cause is thyroidectomy, Neuritis All muscles are paralyzed except for cricothyroid Cords lie in para median position/median Voice is good, no aspiration Inadequate airway –dyspnea , Stridor precipitated by URTI
UNILATERAL SLN PALSY Isolated SLN palsy is very rare Cricothyroid paralysis with anesthesia of I/L larynx above vocal cord External branch injury during thyroid surgery, neuritis, diphtheria Weak breathy with inability to raise pitch, diplophonia. Frequent throat clearing, paroxysmal coughing, vague foreign body sensation
UNILATERAL SLN PALSY Paralyzed cord is shortened, bowed and depressed below level of normal vocal cord Floppy cord which moves with respiration.
BILATERAL SLN PALSY Least common – trauma, neuritis, neoplastic lesions Voice weak, breathy, diplophonia and inability to raise pitch Cough and choking due to aspiration Bronchopneumonia
COMBINED (RLN+SLN) U/L PALSY Paralyzed Cord in cadaveric position – Hoarseness Glottic incompetence Hoarseness, aspiration of liquids Ineffective cough Partial anesthesia of larynx and aspiration COMBINED (RLN+SLN) B/L PALSY Paralyzed Cords in cadaveric position – Aphonia Glottic incompetence -Aspiration Ineffective cough –retention of secretion in chest Anesthesia of larynx and aspiration
INVESTIGATIONS
Analysis of cord mobility 1. Rigid 70 degree video telescopy LA 2. Fibreoptic video laryngoscopy
Serology CBC with ESR (Blood count to r/o lymphoma, TB) Chest X-Ray PA view - any lung disease, particularly carcinoma Barium swallow - Esophageal neoplasms
Radiology HRCT with contrast from skull base to mid thorax – GOLD STANDARD Investigation If an intracranial pathology -> MRI is required.
Treatment of phonatory gap in u/l abductor Cause for vocal fold paralysis is known , damage is permanent and there is no chance for return of function, immediate management. When the cause is idiopathic - wait and observe the patient for 6 -12 months before surgical intervention is applied.
1. Voice Therapy 2. Vocal cord injection 3 Medialization thyroplasty 4. Arytenoid Adduction 5. Artenoidopexy
Voice therapy - These methods are utilized to reduce the vocal and laryngeal hyper function that results in an attempt to compensate for lack of glottic closure.
Indication for immediate surgical intervention 1. EMG Fibrillation complete loss of function with no signs of recovery 2. Vocal cord palsy due to nerve entrapment in thyroid/bronchial malignancy where recovery not expected
VOCAL CORD MEDIALIZATION PER ORAL TEFLON INJECTION Percutaneous teflon injection
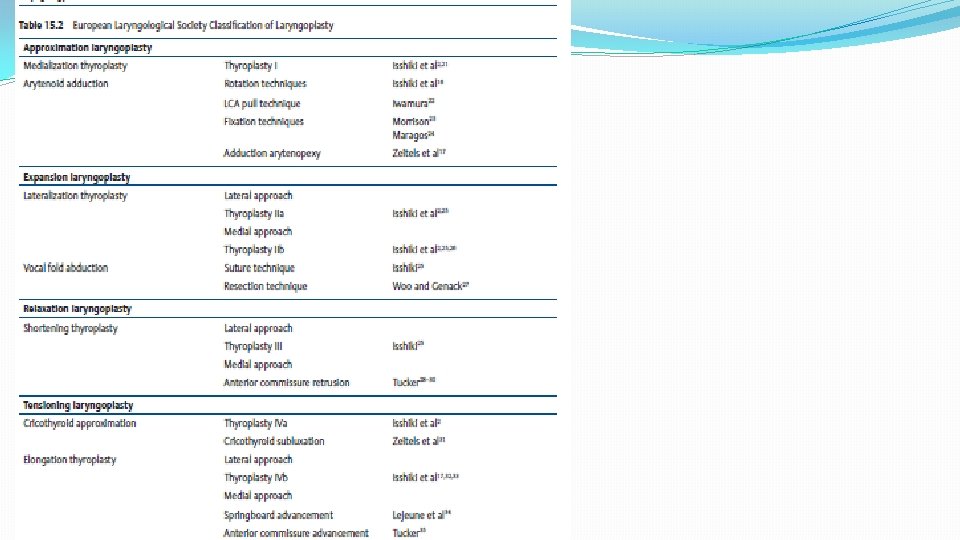
TYPE 1 THYROPLASTY -medialization thyroplasty
Arytenoid adduction
LARYNGEAL RE-INNERVATION Neuromuscular pedicle of superior belly of omohyoid or sternohyoid + ansa cervicalis nerve transferred Thyroarytenoid muscle for vocal cord medialization Neural anastamosis of ansa cervicalis nerve directly to RLN
Combination surgery NM pedicle re-innervation + thyroplasty type 1 Thyroplasty type 1 + arytenoid adduction Arytenoid adduction has advantage of posterior glottic approximation unlike thyroplasty
TREATMENT OF B/L ABDUCTOR PALSY Tracheostomy – temporary or permanent in acute stridor. Endoscopic vocal cordotomy – knife, cautery, laser. Arytenoidectomy – endoscopic or external. Type II laterization thyroplasty. Laryngeal re-innervation.
Cordotomy
Type II thyroplasty
Laryngofissure with arytenoidectomy
RE-INNERVATION Ansa Hypoglossi – Omohyoid pedicle transfer to posterior cricoarytenoid
TREATMENT FOR B/L ADDUCTOR PALSY CAUSING CHRONIC ASPIRATION
PROCEDURES Tracheostomy Gastrostomy Epiglottopexy Vocal cord plication Total laryngectomy Diversion procedure –trachea at 3 /4 th ring is anastamosed to esophagus and lower part of trachea brought as tracheostome
Congenital vocal cord palsy Unilateral or bilateral Unilateral – trauma or congenital anomaly of great vessel or heart Bilateral – hydrocephalus, Arnold Chiari malformation, meningocele, cerebral haemorrhage, nucleus ambiguous agenesis Bilateral –bilateral abductor paralysis - tracheostomy
summary Vocal cord paralysis occurs from interrupted nerve impulse to laryngeal muscles It can affect phonation and respiration. Etiology include trauma during surgery, viral infections and cancers Treatment include voice therapy and surgery depending upon the neve affected and duration of disease
Reference. . 1. Disease of Ear, Nose, Throat &Head and Neck surgery – PL Dhingra, Shruthi Dhingra Acknowledgement Images from google images and text book(Disease of Ear, Nose, Throat &Head and Neck surgery – PL Dhingra, Shruthi Dhingra)