Vocal cord palsy evaluation of hoarseness Dr Vishal







, Right")



: lung (>50%), thyroid, esophageal, nasopharyngeal, metastatic neck node Surgical trauma (20%): during")
 Neck Mediastinum Accidental trauma Bronchogenic ca Thyroid disease")
 • Neck trauma • Thyroid disease • Thyroid")
 • Thyroid surgery • Ca thyroid • Cancer")







 & Semon (1881) p “In all progressive organic lesions,")








 Faint whisper Functional adductor paralysis Forced whisper Organic")






 p Fundamental frequency: lowest speech frequency p Shimmer: average")

















 Vocal cord injection: with Teflon /")









 p Type 2 (lateral displacement) p Type")





 = thyroid alar height (mm) – 4 ------------------- 4")






 + ansa")






 Vocal")
")







")

 • Epiglottic flap closure • Epiglottopexy to")












 Used for mutational falsetto")
 Used for raising vocal pitch & ing vocal tension")
")







. No improvement")


- Slides: 125
Vocal cord palsy & evaluation of hoarseness Dr. Vishal Sharma
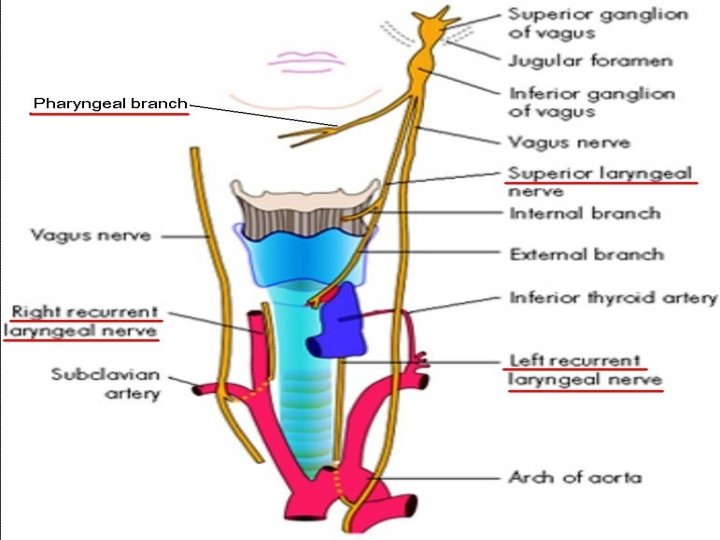
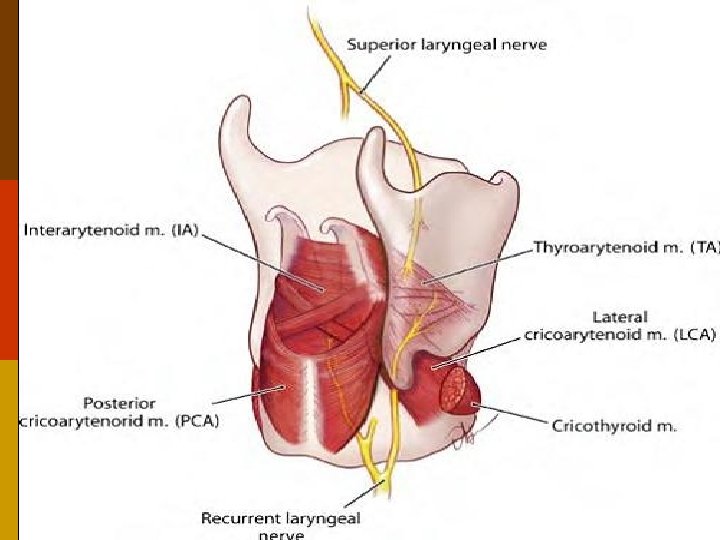
Nerve supply of larynx Motor supply of intrinsic muscles: p Cricothyroid muscle: superior laryngeal nerve p All other muscles: recurrent laryngeal nerve Sensory: p Above vocal cord: superior laryngeal nerve p Below vocal cord: recurrent laryngeal nerve
Recurrent laryngeal nerve Right: p Arises from vagus at level of right subclavian artery & hooks around it Left: p Arises from vagus in mediastinum at level of arch of aorta & loops around it
Development of arterial arches
Final position of B/L RLN
Superior laryngeal nerve p Arises from inferior ganglion of vagus p Descends behind internal carotid artery at level of greater cornu of hyoid bone divides into external & internal branches p External motor branch: to cricothyroid muscle p Internal sensory branch: pierces thyrohyoid membrane to enter larynx
Dual innervation of inter-arytenoid muscles
Classification A. Incomplete paralysis 1. Recurrent laryngeal nerve palsy a. Left (75% ), Right (15%), B/L (10%) b. Abductor, Adductor 2. Superior laryngeal nerve palsy B. Combined paralysis / complete paralysis
Causes of laryngeal paralysis p Supra-nuclear p Nuclear: nucleus ambiguus p High vagal lesions: combined palsy p Low vagal lesions: recurrent laryngeal nerve palsy p Systemic causes p Idiopathic
Causes of combined paralysis Intracranial Neck Tumors of posterior fossa Penetrating injury Basal meningitis (TB) Parapharyngeal tumors Skull base Metastatic neck nodes Fractures Lymphoma Nasopharyngeal cancer Thyroid surgery Glomus tumour
Etiology of recurrent laryngeal nerve palsy
Malignancy (25%): lung (>50%), thyroid, esophageal, nasopharyngeal, metastatic neck node Surgical trauma (20%): during surgeries of lung, heart, thyroid, esophagus, mediastinum Inflammatory (13%): tuberculosis, syphilis Idiopathic (13%): viral neuritis Non-surgical trauma (11%): accidental neck trauma, left atrial enlargement (Ortner), aortic aneurysm Neurological (7%): CVA, head injury, Parkinsonism, multiple sclerosis, alcoholic / diabetic neuropathy Others (11%): rheumatoid arthritis, haemolytic anemia
Causes of left RLN palsy (75%) Neck Mediastinum Accidental trauma Bronchogenic ca Thyroid disease Ca esophagus Thyroid surgery Ca esophagus Lymphadenopathy Aortic aneurysm Lymphadenopathy Enlarged left atrium Intra-thoracic surgery
Causes of right RLN palsy (15%) • Neck trauma • Thyroid disease • Thyroid surgery • Ca cervical esophagus • Cervical lymphadenopathy • Aneurysm of subclavian artery • Ca apex right lung • TB of cervical pleura
Causes of B/L RLN palsy (10%) • Thyroid surgery • Ca thyroid • Cancer cervical esophagus • Cervical lymphadenopathy
Congenital vocal cord paralysis Unilateral: birth trauma, congenital anomaly of great vessel or heart Bilateral: Hydrocephalus Meningocoele Arnold-Chiari malformation Cerebral agenesis Intra-cerebral hemorrhage Nucleus ambiguus agenesis
Thyroid surgery Joll’s sterno-thyro-laryngeal triangle for S. L. N. : Lateral = superior thyroid vessels & upper thyroid pole; superior = attachment of strap muscles to thyroid cartilage; medially = midline Beahr’s triangle for recurrent laryngeal nerve: Lateral = common carotid artery; superior = inferior thyroid artery; medial = tracheo-esophageal groove + recurrent laryngeal nerve
Joll’s triangle for SLN
Beahr’s triangle for RLN
Why right RLN commonly damaged in thyroid surgery? p Right recurrent laryngeal nerve more superficial p Right nerves enters thyroid at 450 angle but left lies in tracheo-esophageal groove p Right nerve mostly passes superior to or b/w branches of inferior thyroid artery; left nerve mostly passes deep to inferior thyroid artery
Position of Distance vocal cord from centre Healthy Diseased Median Midline Phonation RLN paralysis Paramedian 1. 5 mm Strong whisper RLN paralysis Intermediate (Cadaveric) 3. 5 mm (neutral position) Paralysis of both RLN & SLN Gentle abduction 7 mm Quiet respiration Paralysis of adductors Full abduction 9. 5 mm Deep inspiration --
Position of vocal cords
Semon’s Law p Rosenbach (1880) & Semon (1881) p “In all progressive organic lesions, abductor fibres of recurrent laryngeal nerve, which are phylogenetically newer, are more susceptible and thus first to be paralyzed compared to adductor fibres. ”
1 st stage: only abductor fibres damaged; vocal folds approximate in midline; adduction still possible (paramedian position) 2 nd stage: contracture of adductors; vocal folds immobilized in median position 3 rd stage: adductors become paralyzed; vocal fold assumes cadaveric position
Why abductors affected first ? p Nerve fibres supplying abductors are in periphery of recurrent laryngeal nerve p Muscle bulk for the abductors is less, more susceptible p Phylogenetically, larynx’s main function is protection, so adductor functions are maintained
Wagner & Grossman Theory p In isolated paralysis of recurrent laryngeal nerve, cricothyroid muscle (which receives innervation from superior laryngeal nerve) keeps vocal cord in paramedian position due to adductor function p In superior laryngeal nerve palsy, cord lies in intermediate (cadaveric) position
Modern theory Final position of paralyses vocal cord is not static & is decided by: p Degree of paralyzed muscle atrophy & fibrosis p Degree of re-innervation following injury p Extent of synkinesis (mass movement) of all intrinsic muscles p Fibrosis & ankylosis of crico-arytenoid joint
Intermediate position of vocal cords in RLN palsy ? p Retrograde atrophy of vagus nerve occurs up to nucleus ambiguus p Stretching of RLN by enlarged intra-thoracic lesions pulls vagus nerve down from skull base, injuring superior laryngeal nerve
Vocal cord paralysis Cricoarytenoid joint fixation 1. Floppy, vocal cords with bowing 1. Absent 2. Arytenoids falls antero-medially 2. In position 3. Vocal cord at a higher level 3. Same level 4. Tilting of larynx paralysed side 4. Absent 5. Flickering of cord on phonation 5. Absent 6. Shallow pyriform fossa 6. Normal 7. Fixed in specific position 7. Any position 8. Arytenoids can be moved 8. Arytenoids fixed
Clinical Features
Lesion above pharyngeal branch p Inability to elevate soft palate, nasal intonation, nasal regurgitation & nasal emissions p Gag reflex reduced or absent due to palsy of internal branch of superior laryngeal nerve p Hoarseness due to palsy of intrinsic muscles of larynx
p Asymptomatic (1/3 rd unilateral paralysis) Faint whisper Functional adductor paralysis Forced whisper Organic adductor paralysis Voice tires with use Unilateral abductor paralysis Stridor & aspiration Bilateral abductor paralysis
U/L S. L. N. palsy • Disability in professional voice user only • Voice weak, breathy, inability to raise pitch • Anterior commissural tilt to healthy side • Short & flabby vocal fold • Flapping cord during respiration B/L S. L. N. palsy • Professional voice compromised • Voice weak, breathy, inability to raise pitch • Absence of anterior commissural tilt • Cough & choking due to aspiration
U/L combined palsy • Cord in cadaveric position hoarseness • Glottic incompetence ineffective cough B/L combined palsy • B/L cords in cadaveric position aphonia • Glottic incompetence ineffective cough • Total anesthesia of • Partial anesthesia of larynx aspiration + bronchopneumonia
Specific Investigations
Voice assessment 1. Magnetic tape recording: for self assessment 2. Performance assessment by examiner: maximum phonation time & range of speech frequencies 3. Phonetogram: plot of pitch vs. intensity of voice 4. Aerodynamic analysis: phonatory airflow rate, subglottic pressure & laryngeal resistance
Phonetogram
Aerodynamic analysis
5. Fourier’s Spectral analysis (Spectrogram) p Fundamental frequency: lowest speech frequency p Shimmer: average cycle to cycle difference in amplitude of sound p Jitter: average cycle to cycle difference in duration of glottal cycle In hoarseness there is increased shimmers & jitters
Spectrogram
Shimmer & Jitter
Analysis of cord movement 1. Rigid 700 video-telescopy ↓LA 2. Fibreoptic video-laryngoscopy 3. Stroboscopy: Intermittent flash light focussed on vocal cords during phonation. Frequency of light made 2 msec slower to cord frequency. Produces slow motion movement of vocal cords for better analysis of cord movement
Video-stroboscopy
4. Electro-glottography: 2 electrodes placed on both sides of thyroid cartilage & current passed b/w them. Recorded waveform shows impedance across larynx & is highest during contact b/w vocal cords. Records closing phase of glottal cycle. 5. Photo-glottography: fibreoptic light source passes light via glottis & is received by photo-sensor on neck skin. Light received glottic chink. Records opening phase of glottal cycle.
Electroglottography
Photoglottography
Radiological p Submento-vertical skull base view p X-ray neck AP & lateral view p Chest X-ray PA view p Barium swallow AP & lateral oblique view p High resolution CT scan with contrast from skull base to mid thorax: gold standard p M. R. I. : ideal for skull base lesions p Thyroid scan
Endoscopy 1. Rigid 700 Telescopy ↓ LA 2. Fibreoptic Laryngoscopy ↓ LA 3. Pan-endoscopy ↓ GA (for metastatic node): a. Nasopharyngoscopy b. Micro-laryngoscopy: probe test on arytenoids c. Bronchoscopy & bronchial washings d. Hypopharyngoscopy e. Oesophagoscopy
Fibre-optic laryngoscopy paralyzed vocal fold is foreshortened, lateralized & flaccid
B/L abductor palsy Inspiration Expiration
Biopsy for suspected malignancy 1. F. N. A. B. from enlarged lymph nodes 2. Punch biopsy from visible growth 3. Blind biopsy from (if metastatic node present): p Fossa of Rosenmuller p Base of tongue p Pyriform fossa p Laryngeal ventricles p Bronchial carina
Respiratory function test 1. Conventional spirometry 2. Flow-Volume Loop analysis p Variable extra-thoracic obstruction: ↓ed inspiratory flow p Intra-thoracic obstruction: ↓ed expiratory flow p Fixed obstruction: ↓ed inspiratory + expiratory flow
Flow volume loop analysis
Other investigations Blood: ESR, serology for syphilis Electromyography of intrinsic laryngeal muscles: a. Normal: Joint fixation, post - scarring b. Fibrillation: Denervation (bad prognosis) c. Polyphasic: Synkinesis, Re-innervation (good prognosis)
Electromyography
Treatment for phonatory gap in U/L abductor or adductor palsy
Speech therapy: for 2 -12 months (usual treatment) Vocal cord injection: with Teflon / fat / collagen Medialization thyroplasty (Isshiki type I) Arytenoid adduction: for posterior approximation Arytenoidopexy: medial rotation + fixation
Indications for immediate surgical intervention p Electromyography shows fibrillation (complete loss of function with no signs of recovery) p Vocal cord palsy due to nerve entrapment in thyroid / bronchial malignancy where recovery is not expected
Per-oral Teflon injection p Kleinsasser’s microlaryngoscope introduced p Bruning’s syringe loaded with Teflon paste p Needle pushed lateral to thyroarytenoid muscle p First injection at postero-lateral angle of middle third of vocal cord, 2. 5 mm lateral to cord margin p Second injection (0. 2 ml) made at antero-lateral angle till both cords approximate in phonation p I. V. Dexamethasone given for 24 hours
Per-oral Teflon injection
Vocal fold Teflon injection
Percutaneous Teflon injection p Needle introduced in midline through cricothyroid membrane angled 300 - 450 upward & laterally into vocal cord p Direct lateral penetration of larynx through thyroid ala is alternate route of injection p Vocal cord entered under endoscopic control
Percutaneous Teflon injection
Midline & lateral routes
Vocal fold fat injection
Vocal fold collagen injection
Isshiki’s Thyroplasty p Type 1 (medial displacement) p Type 2 (lateral displacement) p Type 3 (shortening or relaxation) p Type 4 (elongation of tensioning) Thyroplasty is reversible, does not invade vocal folds nor alters their mass or stiffness unlike vocal fold injection
Thyroplasty type I
Thyroplasty type I
Thyroplasty type I Horizontal skin incision made over mid-point of thyroid cartilage lamina (from a point 2 cm lateral to midline on opposite side to posterior margin of thyroid cartilage on affected side) Subplatysmal flaps elevated & strap muscles retracted laterally to expose thyroid cartilage Window made in thyroid lamina with scalpel or 1 mm cutting burr, as per Koufman’s formula
p Window’s superior border lies at level with vocal cords (midpoint b/w thyroid notch & inferior margin of thyroid cartilage) & its anterior border situated 8 mm posterior to midline p Cartilage removal started postero-inferiorly p Inner perichondrium elevated off thyroid cartilage & silastic prosthesis inserted p Patient asked to phonate while moving silastic prosthesis into its optimal position under flexible laryngoscopy guidance
Type I thyroplasty
Koufman’s formula Window height (mm) = thyroid alar height (mm) – 4 ------------------- 4 Window width (mm) = thyroid alar height (mm) – 4 ------------------ 2 Average = 12 X 6 mm (male); 10 X 5 mm (female)
Insertion of prosthesis
Insertion of silastic prosthesis
Silastic implant
Arytenoid adduction p Portion of posterior thyroid cartilage margin cut to expose muscular process of arytenoid p Two 4 -0 Prolene sutures passed through muscular process & through thyroid cartilage p Sutures pulled parallel to lateral cricoarytenoid p After optimal medialization of vocal fold, sutures tied on external aspect of thyroid lamina
Arytenoid adduction
Arytenoid adduction
Laryngeal re-innervation p Neuromuscular pedicle of superior belly of omohyoid (or sternohyoid) + ansa hypoglossi nerve transferred into thyro-arytenoideus for vocal fold medialization; or posterior cricoarytenoideus for lateralization (Tucker) p Neural anastomosis of ansa hypoglossi nerve directly to recurrent laryngeal nerve (Crumley)
Neuromuscular pedicle
Neuromuscular pedicle
Neuromuscular pedicle
Ansa-R. L. N. anastomosis
Combination surgeries p Neuromuscular pedicle re-innervation + Thyroplasty type 1 p Thyroplasty type 1 + arytenoid adduction Arytenoid adduction has advantage of posterior glottic approximation unlike thyroplasty
Treatment of stridor in B/L abductor paralysis
Tracheostomy: temporary / permanent in acute stridor Vocal cord lateralization: endoscopic, external (King) Vocal cordectomy: external, endoscopic Endoscopic vocal cordotomy: knife, cautery, laser Arytenoidectomy: endoscopic, external (Woodman) Lateralization thyroplasty (Isshiki type II) Laryngeal re-innervation: ansa hypoglossi-omohyoid pedicle transfer into posterior crico-arytenoideus
Vocal cord lateralization (laterofixation / cordopexy)
Vocal cord lateralization p Thyroid cartilage exposed via horizontal incision p 16 -gauge IV cannula inserted through thyroid cartilage 4 mm anterior & 2 mm below mid-point of oblique line, into laryngeal lumen, just above tip of vocal process, under M. L. S. guidance p Another 16 -gauge IV cannula inserted 5 mm below 1 st cannula, just below tip of vocal process
Vocal cord lateralization p 1 -0 Prolene suture threaded through inferior cannula into laryngeal lumen p Suture thread brought out with forceps into laryngeal lumen & inserted into superior cannula p External traction put on both suture ends to pull vocal cord laterally to give a 5 mm airway p Threads tied over thyroid lamina 8 times
Cordectomy
Cordectomy + lateralization
Posterior cordotomy
Arytenoidectomy
Cordotomy + arytenoidectomy
Thyroplasty type II (lateralization)
Treatment for bilateral adductor paralysis causing chronic aspiration
• Endolaryngeal stenting (solid & vented) • Epiglottic flap closure • Epiglottopexy to posterior pharyngeal wall • Epiglottic tube laryngoplasty • Glottic closure • Sub-perichondrial cricoidectomy • Tracheo-esophageal diversion • Laryngo-tracheal separation • Narrow field laryngectomy
Endolaryngeal stent
Epiglottic flap closure
Epiglottopexy
Epiglottic tube laryngoplasty
Glottic closure
Subperichondrial cricoidectomy
Tracheo-esophageal diversion p Proximal trachea anastomosed with esophagus p Distal trachea opens into permanent tracheostomy
Laryngo-tracheal separation p Proximal trachea closed p Distal trachea opens into permanent tracheostomy
Narrow field laryngectomy
Other procedures for aspiration • Double cuff tracheostomy • Laryngeal suspension • Feeding Gastrostomy • Feeding Jejunostomy • Vocal cord injection • Medialization thyroplasty • Laryngeal re-innervation • Tympanic / Chorda tympani neurectomy
Laryngeal suspension
Other vocal cord surgeries
Thyroplasty type III (shortening) Used for mutational falsetto
Thyroplasty type IV (elongation) Used for raising vocal pitch & ing vocal tension
Evaluation of Hoarseness (dysphonia)
Causes of Hoarseness
Mechanism of hoarseness p Loss of approximation of vocal cords: in paralysis, fixation or intervening tumor / lesions p Alteration of size of vocal cord: ed in edema, tumor; ed in partial surgical excision, fibrosis p Alteration of stiffness of vocal cord: ed in spasmodic dysphonia, fibrosis; ed in paralysis p Improper vibration of vocal cord: hyperemia, vocal nodule, vocal polyp
10 organic dysphonia 20 organic dysphonia 1. Congenital * 1. Laryngitis * 2. Laryngeal tumor * 2. Vocal nodule 3. Vocal cord palsy 3. Vocal polyp 4. Spasmodic 4. Reinke’s edema 5. Muscular * Functional dysphonia 6. Neurological * 1. Psychogenic 7. Endocrine * 2. Habitual 8. Senile 3. Puberphonia 9. Fixation by arthritis 4. Ventricular * 10. Traumatic * 5. Malingering
p Congenital: laryngomalacia, laryngocoele, haemangioma, web p Laryngeal tumor: papilloma, malignancy p Muscular: myasthenia gravis p Neurological: Parkinsonism, Multiple sclerosis, cerebro-vascular accident, bulbar palsy p Endocrine: hypothyroidism, inter-sex, pregnancy p Traumatic: accidental, foreign body, intubation p Laryngitis: bacterial, viral, TB, allergic, GERD p Ventricular: dysphonia plica ventricularis
History taking 1. Duration: > 3 weeks in pt > 40 years is laryngeal malignancy until proven otherwise 2. Progression: due to mass effect or malignancy 3. Voice quality: a. Forced whisper: Organic adductor paralysis b. Faint whisper: Functional adductor paralysis c. Tires with use: U/L abductor paralysis, myasthenia
4. Associated symptoms: a. Stridor: B/L abductor paralysis b. Aspiration: B/L adductor paralysis c. Dysphagia + exertion dyspnea: Ortner’s syndrome d. Hemoptysis: lung malignancy, tuberculosis e. Nasal regurgitation & intonation: high vagal lesion 5. Past history: a. Trauma: accidental, foreign body, intubation b. Surgery: thyroid, intra-thoracic c. Viral upper respiratory tract infection, smoking
Physical Examination p Listening to patient’s voice: for hoarseness p Indirect laryngoscopy: laryngeal lesions p Otoscopy: rule out glomus tumor p Neck: lymph node enlargement, thyroid disease p Chest: lung malignancy, tuberculosis p Cardiovascular: mitral stenosis p Neurological: Parkinsonism, multiple sclerosis
Manual compression test Improvement in voice = do thyroplasty (anterior medialization procedure). No improvement in voice = do arytenoid adduction (posterior medialization procedure)
Routine investigations p Fibre-optic laryngoscopy p Microlaryngoscopy: crico-arytenoid joint mobility p CT scan skull base to diaphragm: best p X-ray chest: for hemoptysis p Ba swallow: for dysphagia p Thyroid scan: for thyroid enlargement p Panendoscopy: in presence of hard neck node
Thank You