Vision Impairment from an Acquired Brain Injury Presenter

Vision Impairment from an Acquired Brain Injury Presenter: Xenia Holland, OTR/L Occupational Therapist November 6 th, 2016


Brain- lobes and functions

Vision as a process Visual Pathway

Vision • Takes us farthest and fastest into the environment • Provides speed for decision making- can convey a lot of info in seconds • Allows us to anticipate and plan for situations • Allows us to adapt to dynamic environments • Helps to elicit and guide movement • Early warning system- helps us maintain postural control
 deficits")
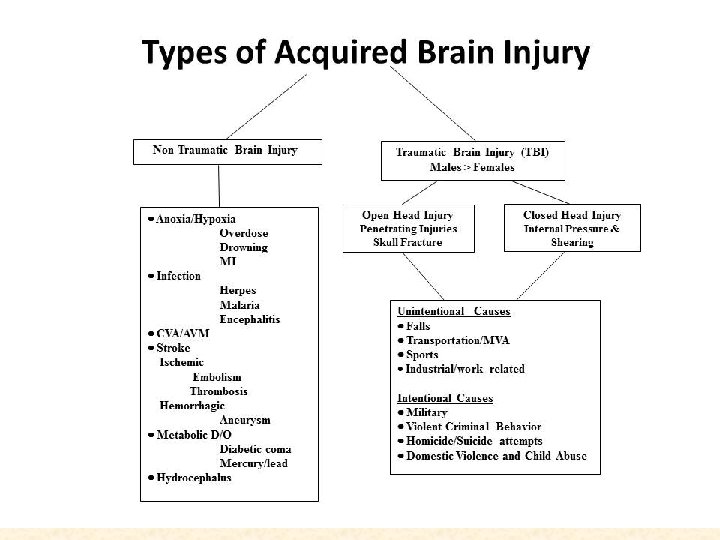
Common visual problems in ABI • Visual acuity deficits • Oculomotor (eye movement) deficits • Visual field loss Leads to: Difficulty completing vision-dependent activities

Visual acuity deficits associated with acquired brain injury • Blurred vision – corneal scarring, trauma induced cataract, vitreous hemorrhage • Focusing difficulties – “accommodation” changes after stroke • Damage to retina – “stroke” of eye, trauma related detachment Quality of image sent to brain for processing is damaged to varying degrees

If oculomotor system is working normally… • Six pairs of muscles that attach to the eye ball – – – Medial rectus Lateral rectus Superior rectus Inferior rectus Superior oblique Inferior oblique • Work together to move the eye through the 9 cardinal points of gaze • Binocular function • Innervated by 3 cranial nerves – Oculomotor Nerve (CN III) – Trochlear Nerve (CN IV) – Abducens Nerve (CN VI)
")
If not working normally, double vision can occur • • The Oculomotor (eye movement) system works to keep the target on the fovea to ensure that it is clearly seen Eye movements are under a complex combination of cortical, brainstem and cerebellar control All control is exerted via the 3 cranial nerves that control the extraocular muscles that move the eyes If system is affected, 2 images may occur leading to double vision

Oculomotor deficits associated with acquired brain injury. Lesions of cranial nerve 3, 4 or 6 • Complete lesions result in “tropia”- eye turned in/out • Incomplete lesions result in “phoria”- tendency of eye to turn in/out • 3 rd and 6 th cranial nerve lesions cause lateral double vision (images split side by side) • 4 th cranial nerve lesion causes vertical double vision (images split up and down) • Functional complaints often involve reading, eye hand coordination and mobility • Most CN lesions resolve within 6 months of injury
Lesion Client is looking straight ahead at target; left eye")
Examples of CN 3 (Oculomotor)Lesion Client is looking straight ahead at target; left eye is deviated outward in exotropic position; pupil is dilated compared to the right. Ptosis: drooping eyelid on left side • Decreased up/down eye movements • Horizontal double vision for near/distance • Exotropic eye- in outward position • Drooping eyelid • Fixed, dilated pupil* • Decreased accommodation • Difficulty near tasks, reading
 Lesion • Impaired down and out eye movement •")
Example of CN 4 (Trochlear) Lesion • Impaired down and out eye movement • Vertical double vision for near/distance* • Hypertropic (elevated) eye position • One sided lesion: may observe a head tilt to opposite side • Two sided lesion: may observe downward head tilt • Most vulnerable cranial nerve to injury – Difficulty reading – Difficulty going down stairslacking down and out eye movement needed to monitor support surface

Unilateral CN 4 Lesion: Head is tilted slightly towards shoulder on non involved left side to avoid diplopia Head is tilted towards deficit right side causing right eye to assume hypertropic position Bilateral CN 4 Lesion: Assumes a head down position to avoid diplopia
Lesion • Unable to move eye outwards • Esotropia or")
Example of CN 6 (Abducens)Lesion • Unable to move eye outwards • Esotropia or Esophoria – Cross-eyed • Complains of lateral (side) double vision for distance • Limitations in – Driving – Ambulation – Activities completed at a distance • Image From http: //www. aapos. org/term s/conditions/100

The Visual Field • Area of visual world that can be seen when looking straight ahead • About 180 degrees horizontally • About 135 degrees vertically • Pathway traverses the entire length of the brain from the retina to the calcarine fissure of the occipital lobe • Most deficits results from damage along this pathway
 associated with acquired brain injury • VFD in Adults are")
Visual field deficits (VFD) associated with acquired brain injury • VFD in Adults are due to – Stroke- infarction (63%) – TBI (12%) – Hemorrhage (11%) Most commonly leads to: • Hemianopia-homonymous hemianopia, binasal, bitemporal • Quadrantanopia- superior, inferior

Visual Field Deficits * 75% result in homonymous hemianopia * 70% with complete hemifield impairment * 30% macular sparing PCA Lesion

Visual field deficits

Effect of Visual Impairment on functional performance • 1. Change in speed of information processing • 2. Change in decision making • 3. Change in response to the environment. The changes in these various areas may affect all aspects of daily living and mobility from performance of the simplest self-care task to the ability to resume driving and return to work.

Functional Implications of visual field loss * 1. Frequently bumps into objects like door-frames or people • 2. Difficulty and uneasiness in moving about in crowded areas. • 3. Unsure of footing while walking and may trip or stumble. • 4. Often startled by moving objects or people appearing suddenly. • 5. May have bruises on shoulder or arm from colliding with door-frames. • 6. Frequently loses place in reading. • 7. Struggles to find or misjudges the start or end of a line of print in reading. • 8. Frequently spills drinks when eating. • 9. Unsteady balance in walking and may report dizziness. • 10. Problems in finding things on desks, counter tops, cabinets or closets. • 11. Fear or anxiety in walking through unfamiliar areas. • 12. Uneasiness or even panic attacks in crowded area. • 13. Withdrawal from going to stores or other crowded areas. • 14. Gets around well at home, but avoids outside activities.

Changes in Behavior • Anxiousness and uncertainty in responding to the environment • Decreased confidence in ability to complete activities • Increased passiveness in decision making

Changes in Orientation • Insufficient visual input to accurately map space on involved side – May result in perceptual completion – Inability to scan fast enough to comprehend scene as a whole • Tendency to get lost – Very uncomfortable navigating alone – Avoids independent travel

Changes in Mobility • • • Hesitant, uncomfortable, anxious Stiff, uncertain gait Shoe gazing Coming very close to obstacles Uncertain on subtle features Stopping to search

Pre-intervention plan • Check eyeglasses • Referrals to OD/MD, other disciplines as needed • If prisms/occlusion/lenses prescribed, then know why, when, how to use • Review any eye reports and medical history

Intervention: Visual Acuity & Oculomotor • Modify environment to increase visibility – Increase contrast – Optimal illumination – Reduce pattern • Reduce demands on vision – Organize environment and tasks – Eliminate steps in task that depend on vision • Create predictable environments – Maximize organization and structure

Ways to reduce visual demands. . Take frequent breaks when doing near tasks Use magnification Increase contrast Avoid bothersome light sources Reduce glare Avoid visual overload Use organization tools- “a place for everything and everything in it’s place” • Use alternative sources such as audio devices, screen readers, phone apps etc • •

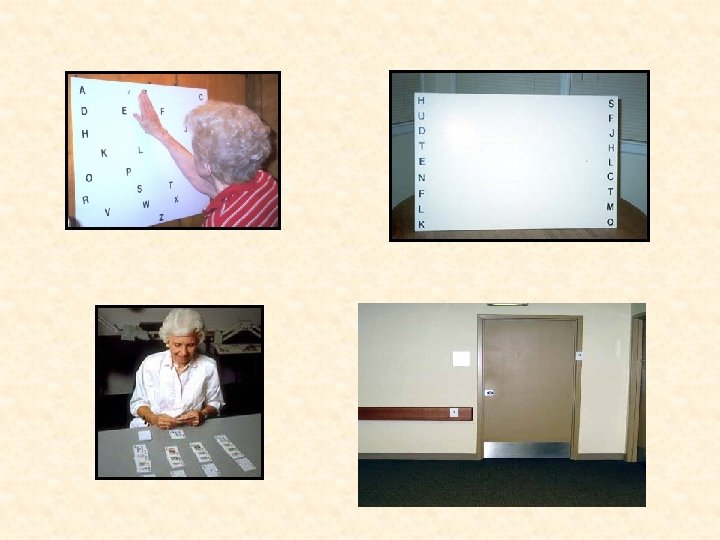
Intervention in visual field loss. Improve search strategies • Focus on developing efficient search strategies to compensate for field deficit • Work in contextual situations • Specifically increasing – Width, efficiency, accuracy of head turn – Visual anticipation/attention towards side of visual loss • Goal is that client automatically employs search strategies without explicitly thinking about them – Search strategies become second nature • Requires over practicing visual skills

Intervention in visual field loss improve navigation/mobility Problem • Does not accurately assess dynamic environment in timely manner resulting in • Collisions • Disorientation • Dangerous maneuvers Desired behaviors – Wider head turn – Increased head movement indicating increase in anticipatory behavior – Organized, efficient search pattern – Before entering an environment, scan thoroughly to locate potential hazards – Increased attention to visual details

Consideration of hemi-neglect and hemi-inattention • Hemi-neglect is a perceptual deficit not a visual one • Person cannot attend to or process the visual information received • Can be coupled with a hemianopia, the person can not or does not readily/spontaneously scan into the area of the hemianopia. • No awareness that a hemi field loss exists • Says doesn't see out of the eye (on the side of the neglect) • Bumps into things on side of the hemianopia but doesn't learn to compensate for the problem • Misses parts of words on the side of the neglect when reading • Misses parts of eye chart line on the side of the neglect • Tendency to orient head or body turned away from the neglect, and the patient may ambulate/drift in direction away from the neglect.

Hemi-neglect leads to limitations in … • Locating items • Completing tasks • Multi-tasking • Rapidly and accurately assessing situations Affecting… Participation in driving, sports, work and many activities of daily living

Interventions for: Hemi-Neglect • Scanning exercises to side of neglect. • “Closed eye” throwing movement. • Encourage awareness of the "feel" of their eyes when gazing as far toward the neglect as possible. • Walk in direction toward the neglected side. • Flashlight aimed at each side while moving around. • “Real” board games or cards, they engage tactile sense. • Use a "beeper-timer" wristwatch as reminder to scan • Facilitate sustained attention- reduce distractions, use familiar tasks and places • Select emotionally meaningful activities- increases motivation • Create attention supporting environments and activities!!!

Take Home Messages Visual impairments due to ABI: • can vary from mild to severe and can affect one or many areas along visual pathway. • they alter quality and amount of visual input to brain and alter the way brain uses that information. • Increasing knowledge of how and why they occur can help in developing an intervention.

Intervention Resources • • • www. eyecanlearn. com www. hemianopsia. net www. positscience. com www. lumosity. com www. sharpbrains. com www. cogmed. com

Slide references *****Slides 5 -20, 22, 23, 24, 26, 28, 29, 30, 31 & 33 Received permission from Mary Warren to use the material/information included in these slides: Mary Warren Ph. D, OTR/L, SCLV, FAOTA Associate Professor, Occupational Therapy Director, Graduate Certificate in Low Vision Rehabilitation Co-Director, UAB Center for Low Vision Rehabilitation University of Alabama at Birmingham External websites and links: • http: //www. cdc. gov/traumaticbraininjury/pdf/Blue. Book_factsheet-a. pdf • http: //braininjurysociety. com/information/acquired-brain-injury/understanding-the-brain/ • http: //www. lowvision. org/traumatic_brain_injury. htm • https: //aapos. org/terms/conditions • https: //www. youtube. com/watch? v=h. Db. WV 0 EZCAU • http: //www. braininjuries. org/hemianopsia_field_loss. html • http: //www. braininjuries. org/brain_injury_double_vision. html • http: //www. braininjuries. org/traumatic_brain_injury. html • http: //www. hemianopsia. net/symptomschecklist/

Clinical References • • • “Introduction to Vision and Brain Injury” by Thomas Politzer, OD. https: //nora. cc/for-patients -mainmenu-34/vision-a-brain-injury-mainmenu-64. html Neuro-Optometric Rehabilitation Association website: www. nora. cc “Loss of Visual Field due to Brain Injury Hemianopsia and Neglect” by Dr. Errol Rummel, FAAO, FCOVD, FNORA. http: //www. braininjuries. org/hemianopsia_field_loss. html Spatial Rehabilitation Using Field Enhancement Prism Systems by NORA Webmaster, 2008 https: //nora. cc/visual-field-loss-rehabilitation-mainmenu-78/spatial-rehabilitationmainmenu-182. html Rehabilitation: Bitemporal hemianopsia: https: //nora. cc/content/view/125/183/ https: //nora. cc/content/view/122/180/ Books: • Zoltan, Barbara. Vision, Perception and Cognition: A manual for the Evaluation and Treatment of the Neurologically Impaired Adult. 3 rd Edition. Slack Incorporated, New Jersey, 1996 • Ophtho. Book: An Introduction to the Eye. 2010 Edition.

Special thank you to Mary Warren for her kind permission to use her information and resources. Mary Warren Ph. D, OTR/L, SCLV, FAOTA Associate Professor, Occupational Therapy Director, Graduate Certificate in Low Vision Rehabilitation Co-Director, UAB Center for Low Vision Rehabilitation University of Alabama at Birmingham
- Slides: 38