Viareggio 5 7 Aprile 2019 Multiple sclerosis MS

: a probabilistic diagnosis There is no single pathognomonic clinical feature or")


 • dissemination in space and time (DIS &")

































- Slides: 39
Viareggio 5 -7 Aprile 2019
Multiple sclerosis (MS): a probabilistic diagnosis There is no single pathognomonic clinical feature or diagnostic test • • Clinical, biological, MRI, cerebrospinal fluid (CSF) examination and electrophysiological data, taken together, are the basis of the different diagnostic classifications Compston A et al. Mc. Alpine's Multiple Sclerosis, 4 th Edition. London 2005; Solomon, Neurology 2019
EVOLVING DIAGNOSTIC CRITERIA OF MULTIPLE SCLEROSIS Mc. Donald 2005 Mc. Donald 2001 Mc. Donald 2010 Mc. Donald 2017 revisions ‘ 80 Poser Clinical & Paraclinical 1868 clinical diagnosis/autopsy gold standard 1965 Schumacher criteria MRI Clinical diagnosis Schumacher Ann NY Acad Sci 1965; Poser, Ann Neurol 1983; Mc. Donald Ann Neurol 2001; Polman Ann Neurol 2005; Polman Ann Neurol 2011
Rationale for the 2017 revisions to simplify or clarify components of the 2010 Mc. Donald criteria to facilitate earlier diagnosis with earlier fulfillment of the 2010 diagnostic criteria To preserve the specificity of the 2010 Mc. Donald criteria To minimize errors To talk a «common language» For clinical research Thompson, Lancet Neurol 2018
Key Concepts Key concept (from Schumacher) • dissemination in space and time (DIS & DIT) • NO BETTER EXPLANATION!!! Thompson, Lancet Neurol 2018
Key Concepts “…the Panel stressed that the Mc. Donald Criteria should only be applied in those patients who present with a TYPICAL CLINICALLY ISOLATED SYNDROME (CIS) suggestive of MS or symptoms consistent with a CNS inflammatory demyelinating disease…” Correct interpretation of symptoms and signs is a fundamental prerequisite for diagnosis. ” Polman et al. , Ann Neurol 2011, Thompson Lancet Neurol 2018
DIS: ≥ 1 T 2 lesions in ≥ 2 locations periventricular cortical/ juxtacortical infratentorial spinal cord Changes from the 2010 Mc. Donald Criteria: • No distinction between symptomatic and asymptomatic lesions • Both cortical and juxtacortical lesions can be utilized Thompson AJ, et al Lancet Neurol. 2018 Feb; 17(2): 162 -173.
Demonstration of DIS by MRI Filippi et al. , Neurology 2010
Demonstration of DIS by MRI This has been reassessed in a MAGNIMS multicentre cohort (n=86) with CIS adding the evaluation of ICLs improves specificity of the diagnostic criteria preserving sensitivity and accuracy The assessment of ICLs is likely to reduce current MS misdiagnosis Increased consistency in acquisition protocols may improve scoring agreement Preziosa et al. , JNNP 2017; Geurst, Neurology, 2011
Demonstration of DIS by MRI 954 CIS patients with single symptomatic lesion a similar risk compared to patients with 1 asymptomatic lesion Tintorè, Neurology 2016 Including lesions in the symptomatic region in DIS increases the sensitivity of MRI without compromising specificity Brownlee, Neurology 2016
Demonstration of DIS by MRI The 1 PV cut-off shows good specificity and sensitivity to predict a second attack DIS specificity with ≥ 1 PV lesions was slightly lower than with ≥ 3 PV Arrambide et al, Neurology 2017
Demonstration of DIS by MRI Arrambide et al, Neurology 2017 However, drops in specificity using the 1 PV cut-off in older age populations
Demonstration of DIS by MRI when assessing DIS plus DIT no found differences in specificity Arrambide et al, Neurology 2017
Demonstration of DIS by MRI Neurology 2017 the 2017 Mc. Donald criteria maintain the requirement for one periventricular lesion For some patients—eg, older individuals or those with vascular risk factors including migraine— it might be prudent for the clinician to seek a higher number of periventricular lesions Thompson, Lancet Neurol 2018
• Simultaneous presence of gadolinium-enhancing and non-enhancing lesions at any time OR • A new T 2 -hyperintense or gadolinium-enhancing lesion on follow-up MRI with reference to a baseline scan, irrespective of the timing of the baseline MRI Changes from the 2010 Mc. Donald Criteria: • No distinction between symptomatic and asymptomatic lesions • The presence of CSF-specific oligoclonal bands does not demonstrate DIT per se but can substitute for the requirement for demonstration of this measure Thompson AJ, et al. Lancet Neurol. 2018
Objective: to explore the value of oligoclonal bands in the context of the 2010 Mc. Donald criteria, in patients fulfilling dissemination in space at baseline 566 patients CIS with Ig. G oligoclonal bands and sufficient data on baseline brain MRI to assess dissemination in space and time
a. HR for fulfilling 2010 Mc. Donald MS over time Arrambide, Brain 2018
If no better explanation CIS + clinical or MRI evidence of DIS and DIT CIS + clinical or MRI evidence of DIS but not DIT 2 nd event or new MRI with DIT CIS but no clinical or MRI evidence of DIS and DIT CSF: OCBs * 2 nd event or new MRI with DIS and DIT Multiple sclerosis * Similar to Poser laboratory-supported definite MS CIS: clinical isolated syndrome Thompson AJ, et al. Lancet Neurol. 2018.
The 2017 Mc. Donald criteria If criteria are applied robotically Patients with MS may not fulfill diagnostic criteria but still the underlying disease is MS Patients with other conditions may fulfill diagnostic criteria but the underlying condition is not MS Thompson, Lancet Neurol 2018
CADASIL Krabbe Chronic Progressive External Ophtalmoplegia Migraine Steinert Leber Antiphospholipid antibodies Hypertension Hyperhomocysteinemia Behcet Fabry Adrenoleukodystrophy Cerebrotendinous Copper Deficiency Vit B 12 Deficiency Xanthomatosis Courtesy of Nicola De Stefano
Warning about the risk of misdiagnosis Thompson, Lancet Neurol 2018
Clinical syndromes typical and atypical for MS Solomon, Neurology 2019; Thompson Lancet Neurol 2018
Warning about the risk of misdiagnosis • Each one can raise red flags and lead to consider alternate diagnoses • Much worse to overdiagnose patients with MS rather than waiting to have enough confidence in the diagnosis Thompson, Lancet Neurol 2018
Diagnoses and syndromes mistaken for MS Solomon, Neurology 2016
Warning about the risk of misdiagnosis Thompson, Lancet Neurol 2018
MS Red flags “think a twice” age ethnicity < 11 years African (ADEM/ anti. MOG-spectrum) > 50 years Latin American Validation studies for the 2017 Mc. Donald criteria were conducted largely in “patients under 50 within Europe, United States, and Canada” Siva Neurol Clin 36 (2018); Thompson Lancet Neurol 2018
Paraclinical MS Red flags Biological presentation • Blood • Systemic inflammation • • Antinuclear antibodies (ANA) • positive in 20 -30%, low titers (≤ 1: 320). No specificity Might reflect only dysregulation in the immune response Siva, Neurol Clin 36 (2018) 69– 117
Paraclinical MS Red flags Biological presentation although not specific for multiple sclerosis CSF supports the diagnosis and to rule out differential diagnoses • Cerebro-spinal fluid examination • pleiocytosis > 50 WBC/mm 3; Polymorphonuclear cells • • CSF Proteins > 1 g/L Isoelectrofocusing and immunofixation Ig. G (the most sensitive approach) • No Ig. G oligoclonal bands • < 5 -10% in MS • 30% in CIS presence of OCBs is associated with a markedly increased risk of conversion to MS • 92% in Behcet, 75% in Lupus, 50% in sarcoidosis Siva, Neurol Clin 36 (2018) 69– 117; Link et Huang, 2006; Dobson, J Neurol Neurosurg Psychiatry 2013; Mc Lean et al. 1995
MS Red flags MRI presentation Geraldes R, et al. Nat Rev Neurol. 2018
MRI Red flags 32 i. MIMICs mnemonic Geraldes R, et al. Nat Rev Neurol. 2018
MRI Red flags 33 i. MIMICs mnemonic If the criteria for DIS are not met, other diagnoses should be considered according to the imaging features Geraldes R, et al. Nat Rev Neurol. 2018
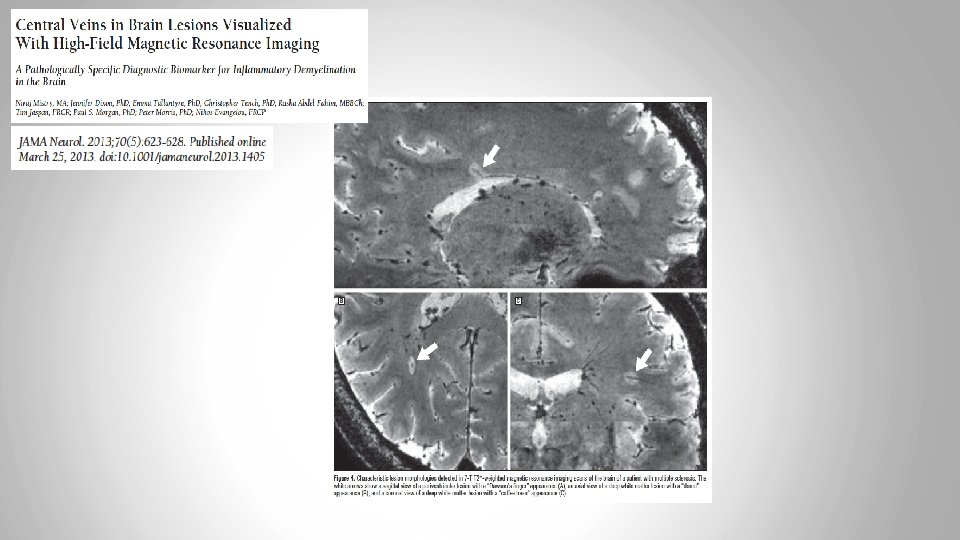
central vein is thought to be characteristic of MS lesions central veins can detect in ~80% of MS lesions at 3 T Sati, NATURE REVIEWS | NEUROLOGY 2016
a cut-off of 50% is highly predictive in distinguishing MS from other diseases that mimic this condition Sati, Nature Reviews Neurology 2016; Maggi et al, Ann Neurol 2018
MRI Red flags Migraine MS FLAIR SWI central vein sign lower in migraine 22% than in MS 84% Sati, NATURE REVIEWS | NEUROLOGY 2016
The MAGNIMS proposed modifications • Susceptibility-weighted MRI Central vein visibility • Three or more periventricular lesions? • One or more optic nerve lesion
130 with optic neuritis CIS The DIS criteria that included optic nerve involvement were more sensitive (95% vs 83%) than the Mc. Donald 2017 DIS criteria but less specific (57% vs 68%). In combination with DIT criteria, the modified DIS criteria remained more sensitive (83% vs 74%); the specificity was the same (77%)