Veterinary Dental Radiology Dr Murat ALIKAN Patient positioning
























- Slides: 26
Veterinary Dental Radiology Dr. Murat ÇALIŞKAN
Patient positioning The first step in creating quality dental images involves positioning of the patient. Utilize sand bags, v-trays and other implements to improve stability and placement of the patient.
• Maxillary teeth = ventral recumbency. • Mandibular canine and incisor teeth = dorsal recumbency. • Mandibular premolar and molar teeth = lateral recumbency with the affected side ‘up’.
Techniques for various individual teeth Parallel technique for mandibular premolar/molar teeth in a dog.
Bisecting angle radiograph for the maxillary canine in a dog. The purple line is the angle of the tooth root and the green line is the bisecting angle between it and the film. Note that the beam is aimed perpendicular to the green line, not the film.
Improper angulation of the radiographic beam. The angle of beam to film is too small. Note the elongation of the roots.
Improper angulation of the radiographic beam. The angle of beam to film is too great Note the foreshortening of the premolar roots.
• Parallel technique is only used for mandibular premolars and molars. • The maxillary cheek teeth are at an approximately 90° angle to the film. • The incisors and canines have crowns with approximately 90° angles to the film; however, the root angles are close to 40°.
Opened dental film packet. From left: paper, film, lead. Chair-side developer.
Proper parallel technique for the mandibular premolars and molars.
Proper bisecting angle technique for the mesial mandibular premolars. This will image the entire root system without distorting the image unduly.
Proper bisecting angle technique for the mandibular canines and incisors.
Proper bisecting angle technique for the maxillary incisors.
Normal dental radiographic anatomy Normal alveolar bone will appear gray and relatively uniform throughout the arcade. It is slightly more radiopaque than tooth roots, and appears slightly but regularly mottled. Bone should completely fill the area between the roots (furcation) and end at the ‘neck’ or cementoenamel junction (CEJ) of the teeth.
The root canals should all be the same width, allowing for differences in the diameters of the roots. There should be no radiolucent areas in teeth or bone. A thin dark line (periodontal ligament) should be discerned around the roots of the teeth.
Normal dental radiograph of the mandibular premolars of a dog. This shows normal bone which completely fills the furcation and regular periodontal ligaments.
Differential diagnoses There are several normal anatomical findings that are commonly misinterpreted in dental images as pathological. In views of: • Mandibular cheek teeth: a horizontal radiolucent line will be seen near the ventral cortex, which is the mandibular canal. There are two circular radiolucent areas seen in the area of the apices of the first three premolars. These are the mental foramina (middle and caudal)
Mesial mandibular premolars of a dog. Note the radiolucent circle apical to the mesial root of P 2. This is a mental foramen.
Mandibular incisal area: a radiolucent line will be observed between the first incisors which is the fibrocartilaginous mandibular symphysis Mandibular canine/incisor radiograph of a dog. The black line in the center is the mandibular symphysis
Rostral maxillary area: there are paired radiolucent areas distal to the second incisors. These are the palatine fissures Maxillary 100 incisor area of a cat. Note the paired radiolucent areas, these are the palatine fissures (arrows).
At the apex of the canine teeth: there is commonly a significant widening of the periodontal ligament. This may appear to be a periapical lesion, but is differentiated from pathology because it is very regular and v shaped, as opposed to irregular and round. These ‘chevron effect’ is a normal finding. If any doubts persist as to a lesion being pathological, obtain radiographs of the contralateral tooth for comparison. ‘Chevron effect’ at the apex of a maxillary canine (arrow).
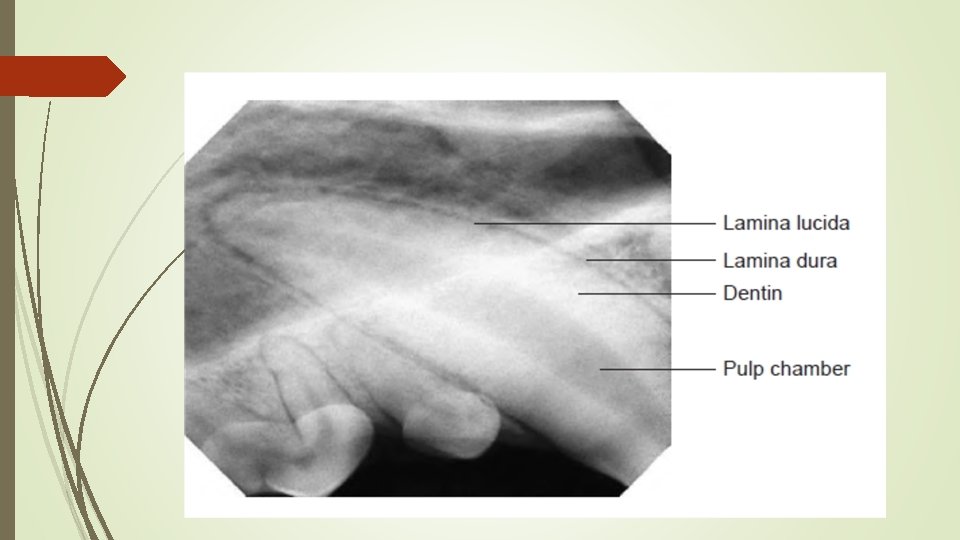
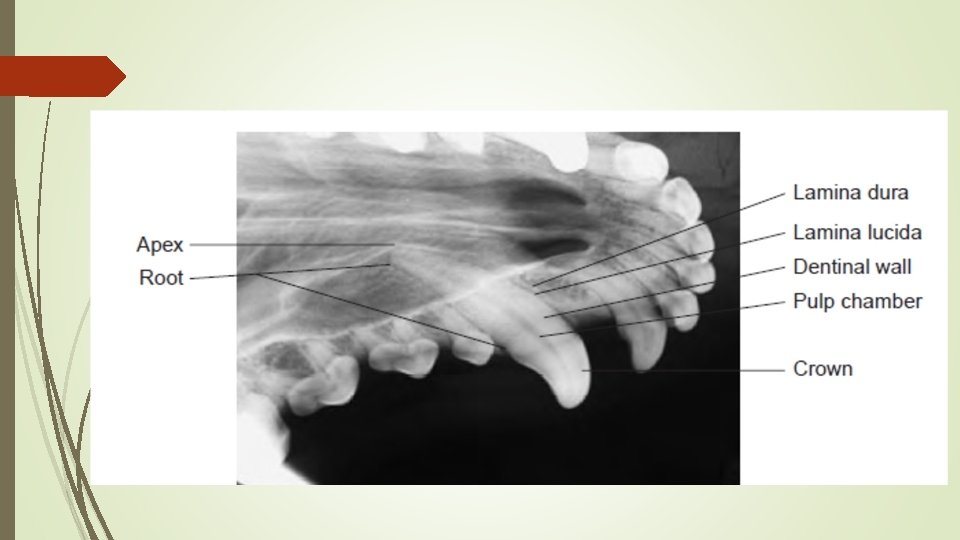
Normal Young Patient • In a young patient, the dentinal wall is thin and the pulp chamber is large. • As the tooth develops, after apexogenesis is complete, odontoblasts that line the pulp chamber will produce secondary dentine. This will thicken the dentinal wall and reduce the size of the pulp chamber and root canal. The apex may be open, depending on the age of the patient.
• In the young patient, the dense cortical alveolar bone forming the wall of the socket appears radiographically as a distinct, opaque, uninterrupted, white line parallel to the long axis of the tooth root(s). This is known as the lamina dura. • The radiolucent image between the lamina dura and the tooth root is the periodontal space and is known radiographically as the lamina lucida. It is occupied by the periodontal ligament. • The trabecular pattern of interdental bone should also be studied
Normal Older Animal • The dental radiograph of a healthy adult will show a decreased pulp canal size and increased dentinal wall thickness. • With age, the lamina dura disappears. • Generally, the width of the lamina lucida will become thinner. • Although an apex is present, the apical delta or apical foramen usually is not seen. • There may be thinning of the alveolar crest.