Vestibular Rehabilitation using a Wide FOV Virtual Environment

Vestibular Rehabilitation using a Wide FOV Virtual Environment PJ Sparto, JM Furman, SL Whitney, LF Hodges, MS Redfern Sponsors Eye and Ear Foundation NIH: P 30 DC 005205, R 21 DC 005372, K 23 DC 005384, K 25 AG 001049

Rationale for use of VR l Inner ear disorder will result in dysfunction of the vestibulo-ocular reflex (VOR), which allows us to maintain stationary gaze position during head turns l Recovery of abnormal VOR requires visual input and head movement l Viirre et al. (1996) and Kramer et al. (1998) proposed use of VR for vestibular rehab l Stimuli can be delivered in controlled manner

Rationale for use of VR l Greater incidence of anxiety and panic disorders in people with dizziness l Dizziness/anxiety often induced by complex visual environments – – – l Grocery stores, shopping mall Driving through tunnels Head movements and optic flow Habituation/exposure therapy is a common treatment strategy for these patients

Rationale for wide FOV l Wide FOV – – l Peripheral motion cues provide greater sense of vection, which is important for postural control Higher cost and greater space HMD – – – Cost-effective Eyestrain, headache, binocular vision changes Maladaptive response because of extra inertia
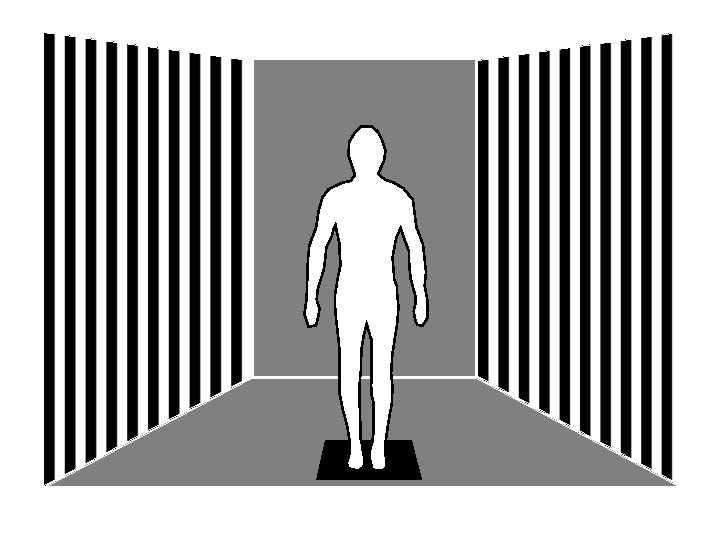
 3 back-projected screens 1 front-projected floor 180 o Horiz x 90")
Balance NAVE (BNAVE) 3 back-projected screens 1 front-projected floor 180 o Horiz x 90 o Vert FOV Surface: rotate and translate
 10 8 6 4 2 0 -2 -4 -6 -8")
Anterior-Posterior Head Sway (cm) 10 8 6 4 2 0 -2 -4 -6 -8 -10 0 10 20 30 40 50 Time (s) 60 70 80 90

Clinical research flow chart l Development of environments l Determine if user interfaces are safe – – l wide FOV HMD What is efficacy of rehab?

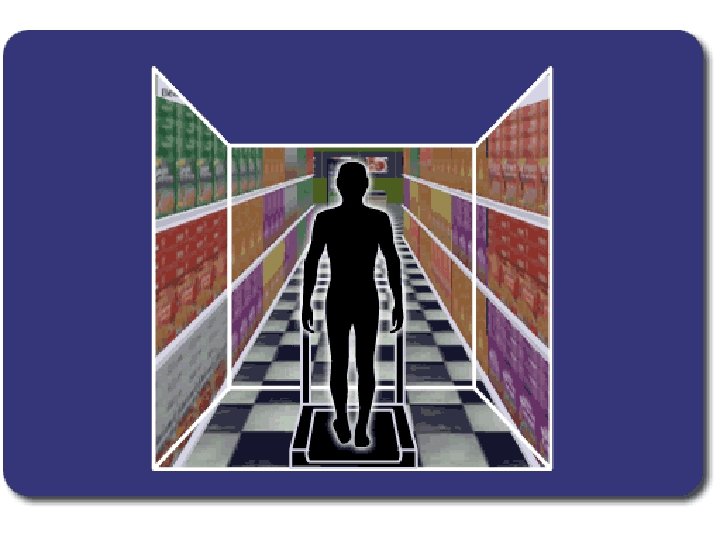
Development of environments l Extract elements from real grocery store l Design geometric models l Model virtual grocery store

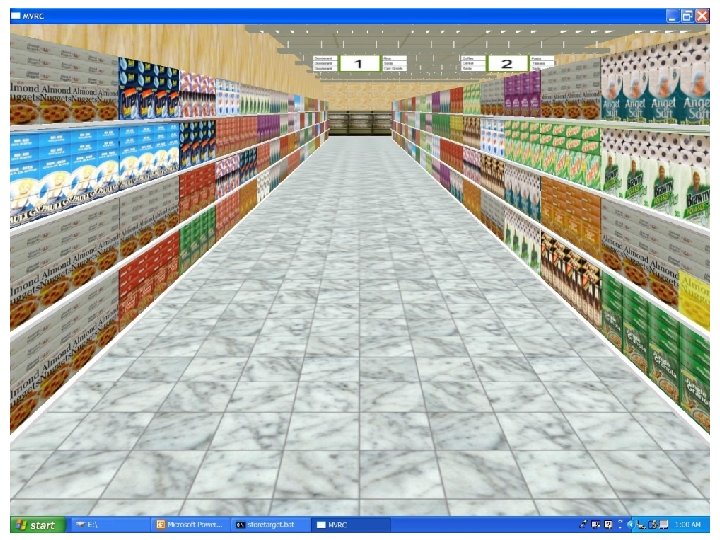


Virtual grocery store l Complexity of store can be easily changed – – – Size of product Height of shelves Width of aisle Pattern on floor Reflection of light on floor

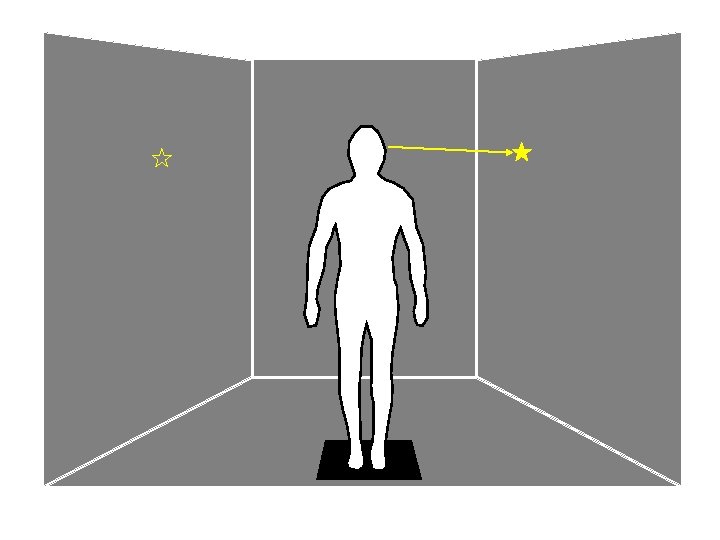
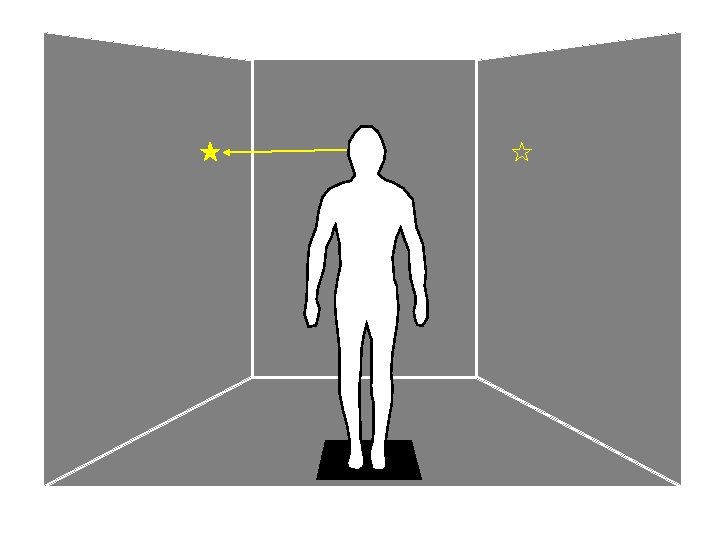
Device safety l l l Can subjects perform coordinated head/eye movements without getting sick 9 healthy subjects performed 8 different coordinated head and eye movements on each visit 6 visits, consisting of a different background – – – 1: Solid background 1: Geometrical elements (stripes), stationary 4: Optic flow (moving stripes)
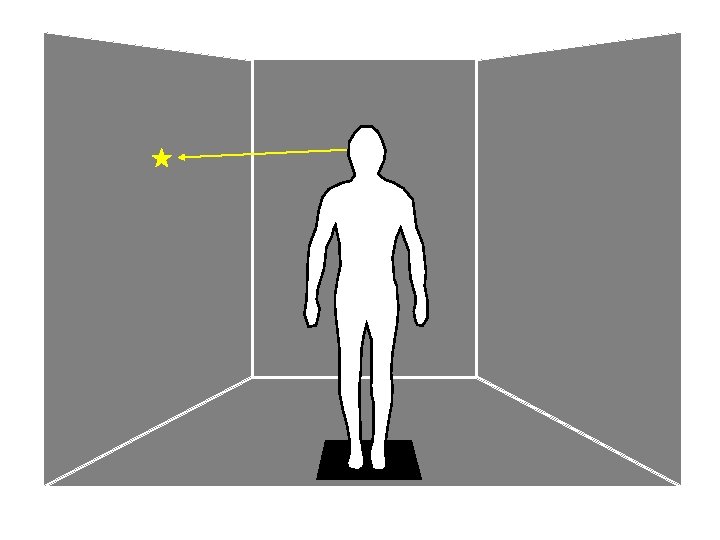

Clinical research flow chart Show box target
 l – 0")
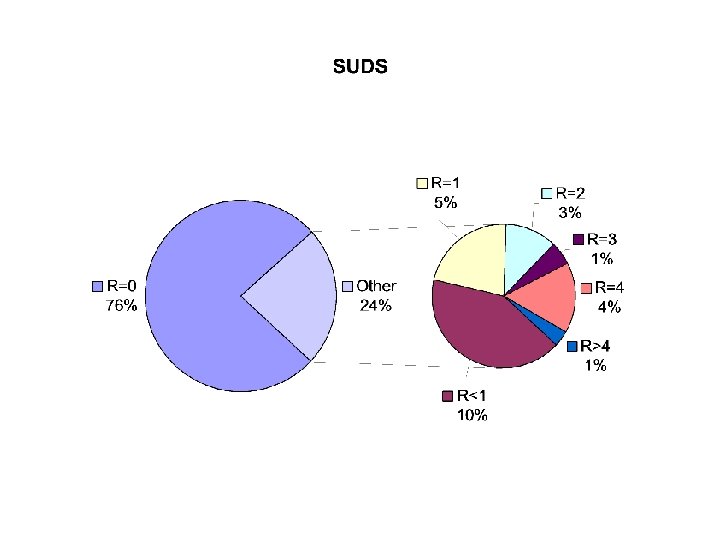
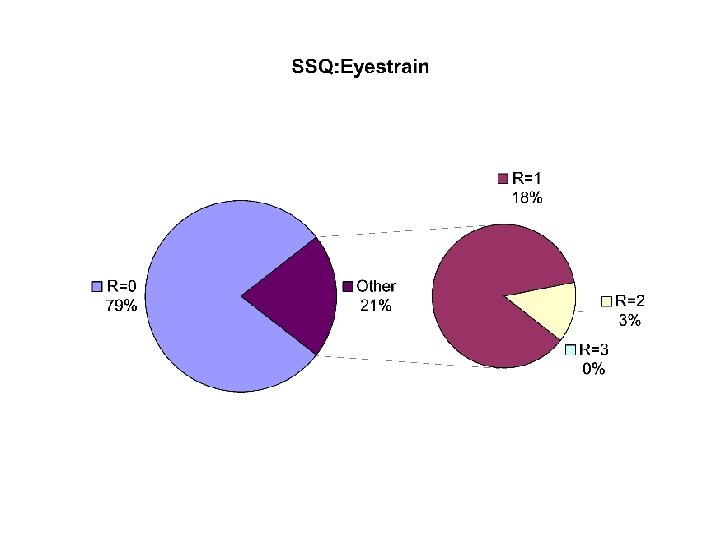
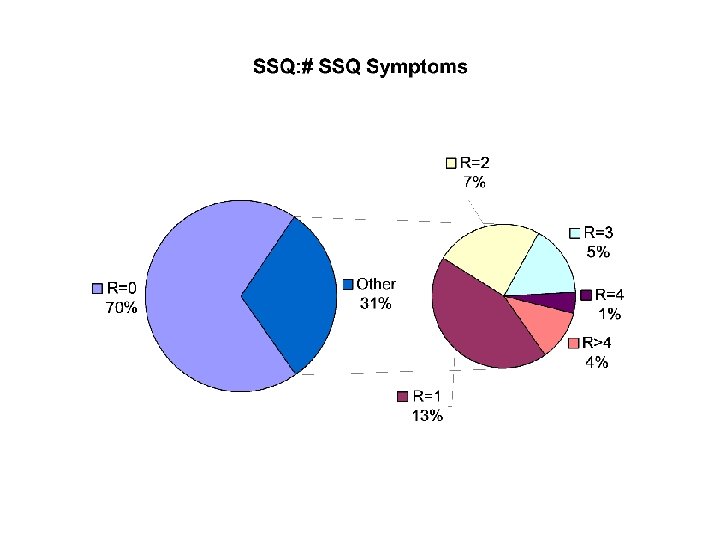
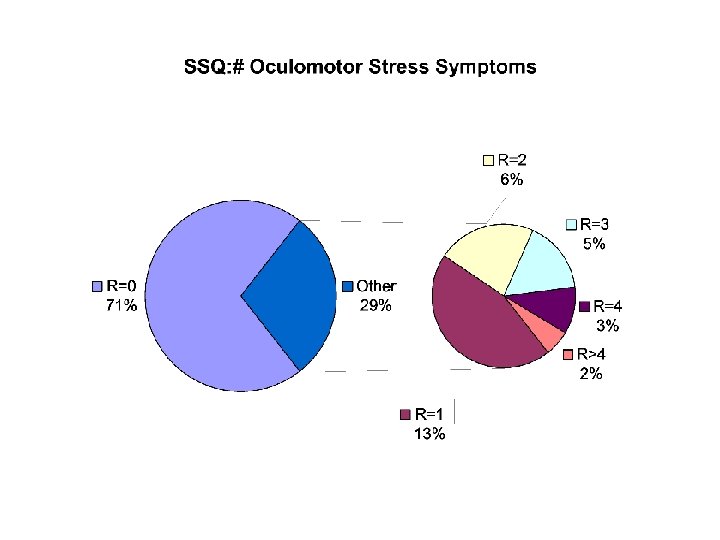
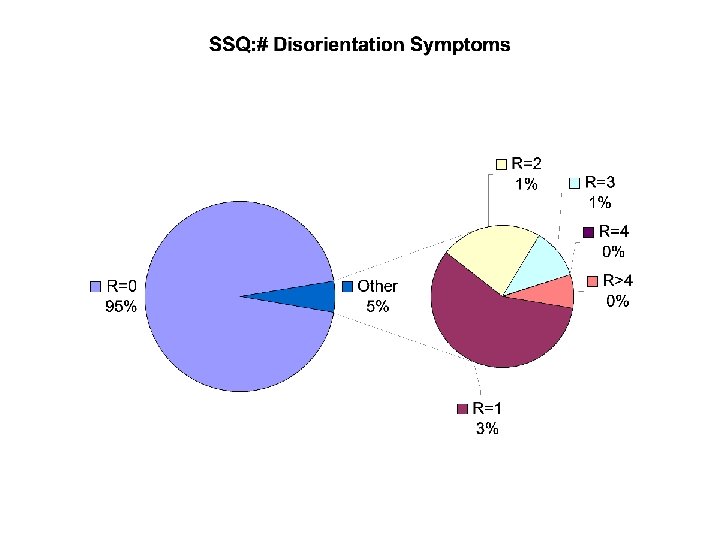
Device safety l l Subject Tolerance Subjective Units of Discomfort (SUDS) l – 0 to 10 Simulator Sickness Questionnaire (SSQ, Kennedy et al. ) l l 16 items rated 0 to 3 (none, slight, moderate, severe) Disorientation (blurred vision, dizziness, vertigo) Nausea (e. g. sweating, nausea, concentration) Oculomotor stress (e. g. fatigue, headache, eyestrain)

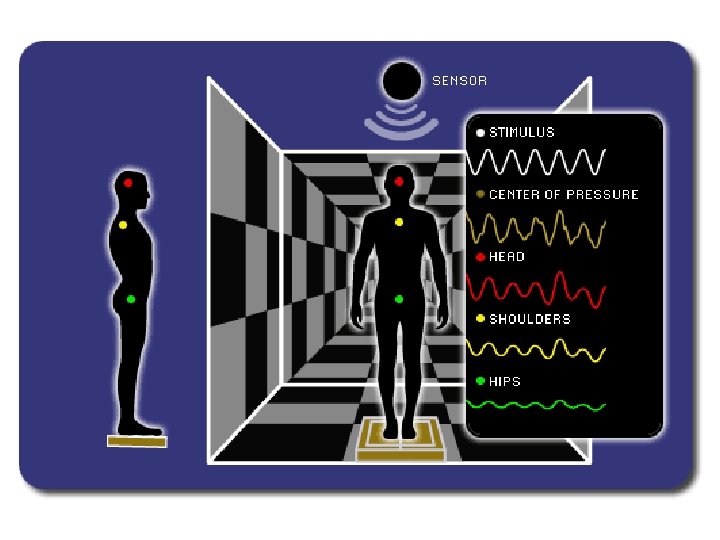
Gaze coordination l Motion Analysis – – – Postural Sway Head and eye movements (gaze) Timing and accuracy of movements
")
Head movements 6 DF Electromagnetic sensor Eye movements Horizontal and vertical Video-oculography (VOG)
 60 T H E 40 20 0 -20 -40 -60 0 10")
Position (deg) 60 T H E 40 20 0 -20 -40 -60 0 10 20 30 40 50 60 70 80 90 100 Position (deg) 60 T G 40 20 0 -20 -40 -60 0 10 Time (sec)

Next steps l 3 subjects with dizziness have begun trials to determine safety l Run experiment in virtual grocery

Clinical research flow chart Show store target

Next steps l Run experiment using HMD l Add treadmill l Clinical trials - efficacy

University of Pittsburgh Depts of Physical Therapy, Otolaryngology, Bio. Engineering UNC-Charlotte Dept of Computer Science Invaluable contributors Jeffrey Jacobson, Leigh Mahoney, Sabarish Babu, Chad Wingrave, many others www. mvrc. pitt. edu
- Slides: 33