VERTIGO By Dr Ejaz Ahmed Assistant Prof Date

VERTIGO By Dr Ejaz Ahmed Assistant Prof Date 3 rd JULY

Learning Objectives ► At the end of today lecture student should be able to , 1 Know about Basic anatomy of inner ear 2 Define Vertigo 3 They should be able to differentiate between vertigo and dizziness 4 They should be able to enumerate different causes of Vertigo 5 They should be able to know specific points during History taking of vertigo patient
 should be assessed by 10")
Class Assessment Mode ► At end of vertigo lectures(2) should be assessed by 10 MCQs.
 ► Otolith organs")
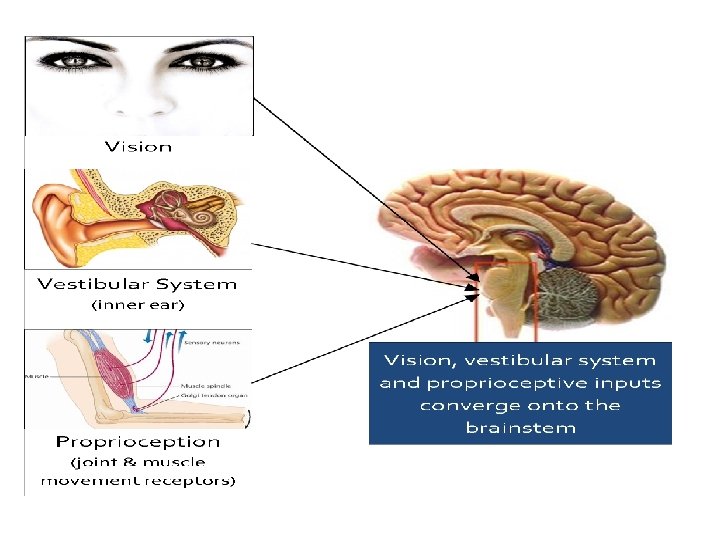
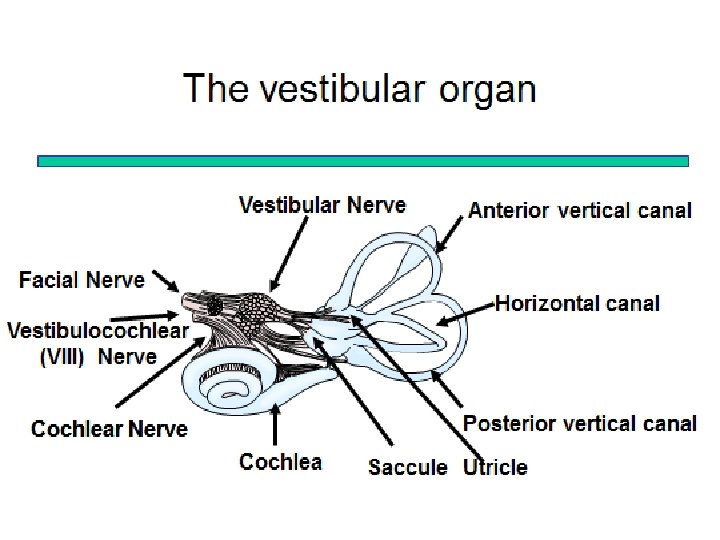
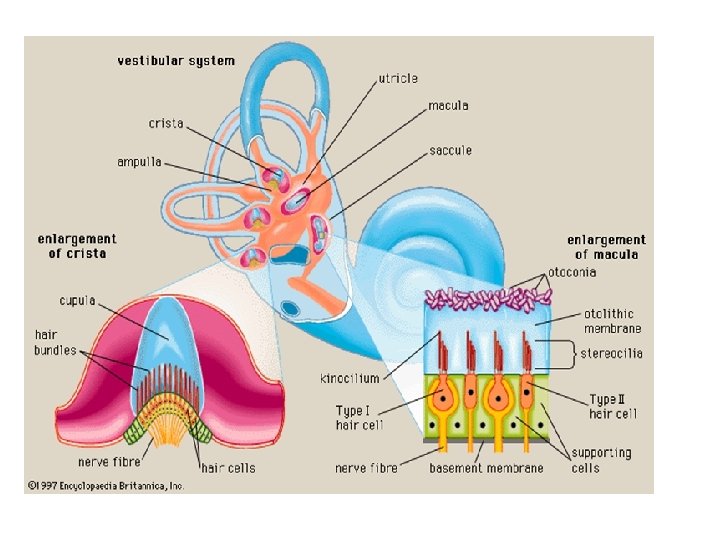
► Peripheral sensory apparatus ► Membranous Labyrinth ► Semicircular canals (SSC) ► Otolith organs

Vertigo Defination Vertigo is a symptom where a person has sensation of moving or of surrounding objects moving when they are not. Often it feels like a spinning or swaying movement. This may be associated with nausea, vomiting, sweating, or difficulties walking.

Vertigo vs Dizziness • Vertigo is a definite symptom while dizziness is an imprecise term. • Sensation of rotation when the patient is stationary is called dizziness, while sensation of rotation in which the patient feels that their surroundings are spinning or moving is called vertigo. • Vertigo is usually associated with nausea, vomiting and unsteadiness, but dizziness may or may not.
 ► Labyrinthitis")
Causes of Vertigo ► Peripheral vertigo ► Benign paroxysmal positional vertigo (BPPV) ► Labyrinthitis ► Vestibular neuronitis ► Ménière's disease

Central vertigo ► Vascular ► Wallenberg’s Syndrome ► Head Injury ► Cerebellar Infarct ► Demyelinating Disease ► Congenital

Differentiation Between Peripheral & Central Causes of Vertigo Peripheral Central Nausea Imbalance Hearing Loss Neurologic Symptoms Compensation severe mild common rare rapid moderate severe rare common slow (Furman JM, Whitney SL. 2000)

Duration of vertigo BPPV Duration Seconds, always < 1 min Migraine Varies sec, minutes, hours or days Meniere’s 20 minutes to hours Vest. neuritis Days Stroke Days

Vestibular Evaluation ► Thorough History ► Detail Physical Examination ► Manuvers and tests

Common Questions • • • Tell me about your symptoms. When did your symptoms begin? How long did/does your symptoms last? Are your current symptoms better, worse or the same? Do your symptoms increase with positional changes or certain movements? Do you have difficulty with keeping objects in focus? Do you have ear fullness, pressure, ringing or hearing loss? Do you have a history of these symptoms? Have you had any falls or unsteadiness? Currently what meds are you taking?

► Cont with next lecture …………. Next lecture we will discuss about COMMON PERIPHERAL CASUES OF VERTIGO BPPV, MENIER DISEASE and OTOSCLEROSIS (ASSISGNMENT AFTER NEXT LECTURE)

Any Questions?


Meniere's Disease

Meniere’s Disease ► it is defined as the symptom complex of episodic vertigo (sensation of whirling and spinning), tinnitus (ringing, roaring, and hissing that usually occurs in one ear), aural pressure (feeling of pressure in the concerned ear), and fluctuating hearing loss ► Typically lasts 20 minutes or more in duration

Meniere’s Disease On temporal bone histopathology, there is a distension of the entire endolymphatic system Audiogram: often low-frequency sensorineural hearing loss that increases during attacks.

► Diagnosis ► A diagnosis of Meniere's disease requires: Two episodes of vertigo, each lasting 20 minutes or longer but not longer than 12 hours • Hearing loss verified by a hearing test • Tinnitus •

►Hearing assessment ►A hearing test (audiometry. Meniere's disease typically have problems hearing low frequencies or combined high and low frequencies with normal hearing in the midrange frequencies.

Treatment ► No cure exists for Meniere's disease. A number of treatments can help reduce the severity and frequency of vertigo episodes. But, unfortunately, there aren't any treatments for the hearing loss

► Medications for vertigo • Motion sickness medications, such as meclizine or diazepam (Valium • Anti-nausea medications, such as promethazine. ► Long-term medication use Diuretic

Middle ear injections ► Medications injected into the middle ear, • Gentamicin, . • Steroids

Surgery ► If vertigo attacks associated with Meniere's disease are severe and debilitating and other treatments don't help, surgery might be an option. ► Endolymphatic sac procedure. • Labyrinthectomy. • Vestibular nerve section

Benign Paroxysmal Positional Vertigo

BPPV Statistics ► BPPV is the most common cause of vertigo in patients with vestibular disorders (Bath et al, 2000) ► About 20% of all dizziness is due to BPPV (Hain, 2010) ► About 50% of all dizziness in older people is due to BPPV (Hain, 2010)

BPPV Defined ► Benign- It does not signify anything life- threatening. Not malignant. ► Paroxysmal- Refers to the fact that the episodes are brief and self-limited – "paroxysm" means "attack. " ► Positional-Change in position provokes symptoms. ► Vertigo-Room spinning sensation.

Causes of BPPV • “Idiopathic”-50%-70% • Head injury- 7%-17% • Viruses

BPPV § Nystagmus ► ► ► Non-voluntary oscillation of the eye Defined fast and slow phases in opposite direction Fast phase defines direction of nystagmus Semicircular canals connected to specific eye muscles, which dictates direction of nystagmus Video

BPPV – Clinical Exam ► Dix-Hallpike Test ► 45 degree cervical rotation ► Align canals with gravity ► Sit to supine with 20 deg of cervical extension ► Look for nystagmus and symptoms of vertigo Herdman, 2000

BPPV – Clinical Exam § Typical Nystagmus ► Latency- before nystagmus starts § ► Direction § ► 1 -30 seconds Mixed up-beating, torsional nystagmus (post. ) Duration § Less than 1 minute § Fatigues with repeated testing
 ► Cupulolithiasis")
BPPV – Clinical Exam § Two types of BPPV ► Canalithiasis (A) ► Cupulolithiasis (B)

Repositioning Procedures Parnes, 2003

BPPV Treatment ► Post-Treatment Instructions- typically 24 hours ► ► Avoid lying down until you go to bed. Avoid up and down head movements. Prop head up at night with pillows. Avoid sleeping on affected side. ► Debate

Otosclerosis ► Otosclerosis is a condition where one or more foci of irregularly laid spongy bone replace part of normally dense enchondral layer of bony otic capsule in the bony labyrinth. This condition affects one of the ossicles (the stapes) resulting in hearing loss, tinnitus, vertigo or a combination of symptoms ► Cause : ► Hereditary , endocrine , biochemical , metabolic , infectious ( eg. Measles ) , traumatic , vascular & autoimmune 38
 : otoscopic exam Schwartz sign")
Histology 3 form: 1 otospongiosis ( early phase ) : otoscopic exam Schwartz sign 2 transitional phase 3 otosclerosis ( late phase ) 39

Clinical manifestation ► CHL : due to fixation of stapes footplate ► SNHL �� 3 mech : 1 toxic metabolite injury to neuroepithelium 2 vascular compromise 3 direct extension to cochlea ► Dizziness : OS inner ear syn; DDX : Meniere dz , superior semicircular canal dehiscence (SSCD) 40

History & Physical examination Age 15 -35 years • Women are affected ► slowly HL over progressive yrs ► Good hearing in noisy situation ( paracusis of Willis ) ► Present tinnitus ~ 75 % ► Otoscopy : TM is normal in most pt , Schwartze sign may be present ► Weber test : lateralize to greater degree of CHL • 41

History & Physical examination ► Initial phase Rinne - ve may be limited to 256 Hz ► Footplate fixation Rinne - ve at 512 Hz & 1024 Hz ► Rinne – ve : air-bone gap ~ 10 -15 d. B at 256 Hz ~ 20 -25 d. B at 512 Hz 42

Audiologic testing ► Audiogram : Cahart notch 43

Audiologic testing ► Tympanogram : type A , As 44

Audiologic testing ► Stepedial reflexes : abn or norm depending degree of fixation 45

► Vestibular test should be in pt with dizziness ► HRCT : v. Early Dz : radiolucent areas around Cochlea Halo sign v. Mature case : diffuse sclerosis ► CT scan helpful R/O middle ear Dz : mass , vascular anomalies 46

Management Amplification pt with HL & not be suitable candidate for Sx ► ����� § Avoid potential risk of profound HL from Sx ► ������� § Usually not used at night § Physical sensation of device in EAC negative sensation In pt with severe to profound SNHL cochlear impant 47

Medical management ► use sodium fluoride ion replace hydroxyl radical form stable fluorapatite complex resist osteoclast activites ► Recommended Dose 20 -120 mg per day ► Side effect : § usually minor GI irritation ( prevent : low dose , enteric coat ) § occasional complaint of jt , bone , muscle pain resolves with temporary discontinuation of therapy § Rare : fluid retention , cutaneous eruption & eye problem 48

Surgical management ► ► 1. 2. 3. Stapedectomy : indicated the stapes fix (A-B gap at least 30 d. B) negative Rinne test at 256 , 512 Hz ( Shambaugh( Successful stapedectomy : correct CHL remove Carhart’s notch closure pre-op A-B gap 49

Contraindication Poor speech discrimination & Hx of vertigo in recent month (because possibility of endrolymohatic hydrop labyrinth open( 2. Pt with only hearing ear should be avoid (relative( 3. Pt with ME infection or effusion (absolute( 1. 50

THANK YOU 51

Assignment ► SAQ ► A 26 YEAR OLD PREGNANT FEMALE PRESENTED IN ENT OPD BY C/O HEARING LOSS AND TINITUS ► 1 MOST LEKLY DIAGNOSIS ► 2 NAME TWO AUDIOLOGICAL TESTS AND FINDING ► 3 ENUMERATE TREATMENT OPTIONS
- Slides: 52