Vertical Jaw Relations Contents Introduction Vertical jaw relation


















 • By using artificial landmarks on nose")




. • Advantages: measured on bony landmarks. no")
 • Principle : activity")


 suggested that distance")


,")

 defined rest position of the mandible as that “ position")
 believed that the rest position is determined by a balance of")

, took issue with the doctrine that physiologic rest position is not")
 felt that the mandibular rest position was completely dependent on the tonicity")
 performed a longitudinal radiographic analysis of face height before and")
 studied the rest position as a guide in prosthetic treatment. Lateral")
 adopted a refined technique using")

 indicated that mandibular pattern")
 concluded that swallowing may be used only as")
 conducted a study to test the accuracy of")








. • Measure anatomic landmarks.")




. - Exact guide")


 • Principle :")



. • Incisive guidance")
. • Rationale : An edentulous")

 • Theory : patient registers maximum amount")
. • Principle : the constant function")

 • Simple method for determining")



 – falling in of")








- Slides: 89
Vertical Jaw Relations
Contents • Introduction • Vertical jaw relation • Determinants of vertical relations of mandible to maxilla • Physiologic rest position • Vertical jaw relation at rest • Recording rest position • Free way space/ interocclusal space
• Discussion – review of literature • Vertical jaw relation of occlusion • Recording vertical relation at occlusion • What happens if vertical dimension is altered? • Summary • Conclusion • References
Introduction • Complete dentures must be used in most functions once served by natural dentition. • Mastication, speech and appearance all depend on specific vertical and horizontal relations of mandible to the maxilla. • Any horizontal jaw relation is valid only at a specific vertical dimension…. . hence the importance of vertical jaw relation.
What is Vertical Dimension? • The vertical dimension is the length of the face as determined by the amount of separation of the jaws.
Vertical Jaw Relation • The vertical jaw relations are those established by the amount of separation of the two jaws in a vertical direction under specified conditions… Boucher. • May be recorded as: vertical jaw relation at rest vertical jaw relation at occlusion • Vertical jaw relation at rest in denture construction is used as guide to the lost vertical dimension at occlusion.
Determinants of Vertical Relations of Mandible to Maxilla • The masticatory musculature • The occlusal stops (teeth or occlusion rims)
Physiologic Rest Position • The postural position of the mandible when an individual is resting comfortably in an upright position and the associated muscles are in a state of minimal contractural activity…GPT 8. • The mandible is said to be in its physiologic rest position when all the muscles that close and open the jaws are in a state of minimal tonic contraction only to maintain posture…. Boucher.
Importance of Physiologic Rest Position
• If this space is not given, the tissues under the denture bearing area get their much needed rest by resorption of the underlying bone.
Methods to Establish the Vertical Jaw Relations • Many methods to establish the vertical dimension at rest and in occlusion have been put forth. • To use several methods and to compare the results is advised.
Categorisation of Methods to Determine Vertical Jaw Relations • According to Sharry : pre-extraction determination post extraction records • According to Boucher : mechanical methods physiological methods • According to Heartwell : to determine, vertical jaw relation at rest vertical jaw relation of occlusion
Vertical Jaw Relation at Rest • The habitual postural position of the mandible when the patient is resting comfortably in the upright position and the condyles are in a neutral unstrained position in the glenoid fossa. …Academy of Denture Prosthetics.
Vertical Jaw Relation at Rest VDR
Features of Vertical Rest Dimension • It is a bone to bone relation. • The position of the mandible is influenced by gravity… • Rest position is a relaxed position… • It may not be easy to record in patients with neuromuscular disturbances. . • This position can not be maintained for any amount of time… • Failure to establish rest position may lead to pain, discomfort and residual ridge resorption…
Recording Rest Position • Niswonger’s method • Facial measurements • Tactile sense • Phonetics • Facial expression • Radiographs – cephalometric method
Niswonger’s Method • Given in 1934 by Niswonger. • He defined the rest position as “the neutral position of the mandible where the opening and closing muscles are in a state of equilibrium. ” • The method : - Patient seated such that ala tragal line parallel to floor. - Two marks are marked…. - Patient told to swallow and relax.
-The dimension is measured between the two points. -Occlusal rims are constructed so that they are 4/32 or 1/8 inch less than the original measurement. Disadvantages: soft tissue landmarks variability to obtain same measurements Interocclusal space {
Facial Measurements • Advocated by Pleasure (1951) • By using artificial landmarks on nose and chin. • photo
Tactile Sense • Patient asked to open mouth wide open until strain is felt in the muscles. • Then he is asked to close the mouth till it reaches a comfortable, relaxed position. • Measure the dimension between points of reference and compare with those got after swallowing.
Phonetics • Patient repeats any word which has the sound ‘em’ in it. till the lips contact. • Ask him to stop all jaw movements, measure between two points of reference. OR • Ask patient to pause in between normal speech and measure between two points.
Facial Expression • Evidence of relaxation of maxillo mandibular musculature… • lips even antero-posteriorly. • Skin around eyes and chin relaxed. • Relaxation around nares.
Clinical Means of Measuring Vertical Dimension…how accurate? ? • Made on soft tissues which are mobile…accuracy questionable. • Manipulation of face is necessary at the time of measurement. • Lack of a permanent reference point to return to, for checking subsequent measured dimensions.
Cephalometric Determination • Method by Atwood (1956). • Advantages: measured on bony landmarks. no manipulation of face needed. permanent record is available, even after months. • Disadvantages: measurements are made of shadow of the reference points. special equipment. radiographic exposure.
Electromyography. . to verify rest position • Shpuntoff and Shpuntoff(1956) • Principle : activity or lack of activity in muscle is measured as a change in its electric potential. muscle contracts electrical activity is measured and amplified. cathode ray oscilloscope tracing • Disadvantages : not practical equipment expensive difficult to interpret tracing
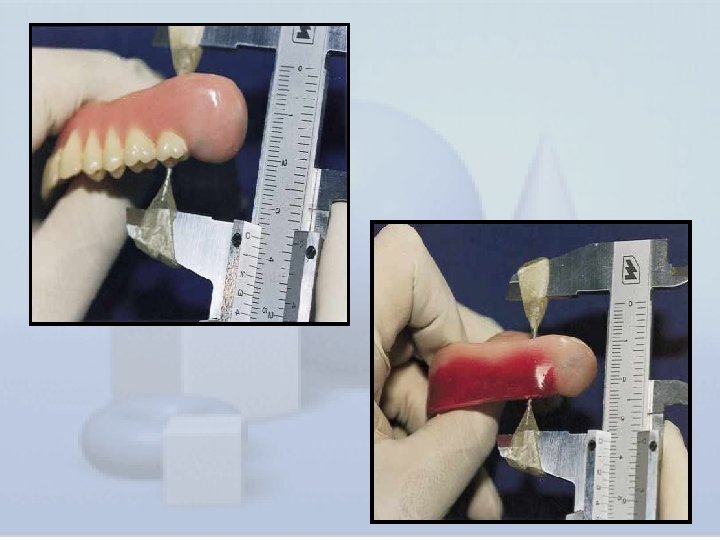
Discussion • Pre extraction records in determining vertical dimension: In spite of fallibility of most pre extraction recording instruments, some are more accurate than the post extraction aids. Measuring instruments like Willis gauge, Vernier calipers were used. But because of the soft tissue impingement, a more reliable method is to measure the distance between the upper and the lower frena with dividers when teeth are in centric occlusion.
• Alternate methods are : Turner’s cut out method using a simple pantograph acrylic face mask plaster face mask • But these methods displace the skin when formed and applied to the face. may lead to inaccuracy.
• Facial dimensions in establishing vertical dimension : • Goodfriend(1933) suggested that distance from the pupil of the eye to the junction of the lips equaled that from the subnasion to gnathion. • However, Willis(1935) has been said to popularise these measurements.
• Using physiologic rest position as a guide to vertical dimension of occlusion: • Dates to as early as 1771. . • In 1771, Hunter wrote “ in the lower jaws, as in all the joints of the body, when the motion is carried to its greatest extent, in any direction, the muscles and ligaments are strained and the persons made uneasy. The state, therefore, into which every joint naturally falls, especially when we are asleep, is nearly in the middle between the extremes of motion, by which means all the muscles and ligaments are equally relaxed. ”
• According to Gottleib, Wallish was one of the first to define the physiologic rest position of mandible as “the position of the mandible where in all muscle action is eliminated and it is passively suspended. ” • Sicher and Tandler(1920), stated “ the rest position of the articulation, the middle position is that in which the mandible is at a slight distance from the maxilla. In this position the mandible is kept against gravity by the forces of the closing muscles”
• Constancy of rest position in a strict sense is doubtful. • Niswonger(1934), designed an instrument called ‘jaw relator’ for use in measuring the distance that the mandible moves from rest position to centric occlusion • He studied 200 dentulous patients. He established that the interocclusal clearance measured 4/32 inch ( 3+mm ) in 87% of pt’s and that the other 13% varies from 1/32 to 11/32 inch.
• He concluded that as the teeth slowly wear down, nature makes the necessary changes in bone and soft tissues to maintain this measurement of 4/32 • Niswonger’s work was the beginning of the dictum that the individual mandibular rest position remains constant throughout life. • This theory has since been referred to as concept of constancy of face height.
• Gillis (1941) defined rest position of the mandible as that “ position from which all mandibular movements begin and to which they return” • Schlosser (1941) conducted a series of phonetic experiments and found a space of from 1 -3 mm between the upper and lower incisors with the lips in contact when natural teeth were present.
• Thompson(1942) believed that the rest position is determined by a balance of tension in the musculature which suspends the mandible, & that the rest position is not affected by the presence or absence of teeth. He indicated that the interocclusal distance averaged 2 -3 mm in normal dentitions & may be 10 mm or more in abnormal dentitions.
• He related variations in rest positions to hypotonicity and hyper tonicity of muscles and described them as short term variations- stress, respiration long term variations- debilitated patients, mouth breathers.
• Leof(1950), took issue with the doctrine that physiologic rest position is not constant throughout life. • He pointed out that muscle tone rather than muscle length controls the rest position, and that muscle tone can and does vary. Leof further stated that we must never eliminate the interocclusal distance. • Oslen (1951) studied physiologic rest position radiographically, his findings suggested that the resting position was not rigidly stable.
Sicher (1954) felt that the mandibular rest position was completely dependent on the tonicity of the musculature and that only in disturbed muscle tonus as in disease, overwork, or nervous tension the rest position varies from normal. He also pointed out that “constancy in a living organism means simply that the range of variation or variability is negligible”.
• Atwood( 1958) performed a longitudinal radiographic analysis of face height before and after extraction on 42 subjects. This study demonstrated variability within a sitting, between sittings, and between readings with and without dentures.
Duncan & Williams(1960) studied the rest position as a guide in prosthetic treatment. Lateral roentgenographic cephalometric measurements were made on 10 patients for whom complete dentures were constructed. They found instability in rest position & hence concluded that, rest position is a poor guide for establishing the pre-extraction occlusal vertical dimension.
• Tactile sense in establishing vertical dimension: Lytle(1964) adopted a refined technique using a central bearing device fixed to upper and lower occlusal rims. Mc. Gee stated that methods which relied on patients’ neuromuscular perception transferred the responsibility of registering the occlusal dimension from the dentist to the patient.
• Phonetics in establishing vertical dimension: • This theory is dependent upon the correlation during speech of the inter occlusal distances and position of the occlusal plane. • Silverman (1953) maintains that it is easier and more accurate to record a measurement which relies upon muscular phonetic enunciation…
• Deglutition in establishing vertical dimension: • Shanahan (1956) indicated that mandibular pattern during deglutition dictates the eruption of teeth so that they are maintained at the occlusal plane by the act of swallowing. this establishes the vertical dimension.
• Ward and Osterholtz (1963) concluded that swallowing may be used only as a guide to the vertical dimension of occlusion. • They advised the dentures should be removed for sometime before recording the occlusal vertical dimension to obliterate the memory of acquired neuromuscular patterns.
• Ismail and George (1968) conducted a study to test the accuracy of the swallowing technique for determining and recording the occlusal vertical relation of jaws as compared to occlusal vertical relation in the same patients before extraction. • They concluded that with the swallowing method, the occlusal face height showed an increase of mean 2. 8 mm before and after extraction.
Acceptance of clinical assessment of vertical dimension of occlusion established by different methods • Under the guidance of Dr. N. P. Patil sir, • Objective : to evaluate the most acceptable method of establishing vertical dimension. • 3 methods: physiologic rest position phonetics swallowing threshold • Results : swallowing threshold method is the most acceptable and comfortable to the patients as compared to the other two.
Free- Way Space/ Interocclusal Space • The difference between the vertical dimension at rest and the vertical dimension while in occlusion…GPT 8.
Average of 2 – 3 mm. Depends on position of head. Is 2 – 3 mm of free-way space a scientific average for rest position of mandible? . . can it be a static entity at any time?
• A study ‘the free-way space and its significance in rehabilitation of masticatory apparatus’ was done by J. S. Landa (1952). • Four methods, the clinical method, measurement by mechanical devices, radiography and registrations by means of extra oral needle point tracers were used to determine inter occlusal space. • Conclusions: Average free way space was 3. 07 to 3. 67 mm. Complex architectural structure of the freeway space cannot be incorporated into an articulator. It cannot be used as the only criterion… It is effected by mandibular movement and by gravity.
Vertical Dimension of Occlusion • The relationship of the mandible to the maxillae when the jaw is closed and the teeth are in contact, this position may or may not coincide with centric occlusion…GPT 8.
• It is a static position, the teeth being the vertical stops. • When used in construction of dentures, the teeth are in centric relation. • When in natural teeth, it may not be in centric relation. So pre extraction records – evaluated carefully.
Recording Occlusal Vertical Dimension • Pre extraction records • Ridge relation • Phonetics • Tactile sensation • Measurement of old dentures • Biting force • Relate Interpupillary distance on photographs to that on face • Swallowing threshold
Pre Extraction Records • Profile photographs: Anatomical landmarks measured. With teeth in maximum occlusion.
• Anatomical Landmarks: • Given by Willis (1935). • Measure anatomic landmarks.
Demerits : inaccuracy because of -inconsistent angulation especially convex profile, people with moustache. -soft tissue compression.
• Facial silhouettes: May be made with card board or lead wires. Placed against profile when establishing vertical dimension.
• Radiography: 1. profile radiographs 2. radiographs of position of condyles • method of radiography may give rise to discrepancy. • inaccuracy also because measurements are made of shadow structures.
• Articulated casts: - obtained with natural teeth in occlusion. - measurements are made of relatively stable landmarks. . - mounted on an articulator with a face bow transfer. - useful in patients whose ridges have not been sacrified.
• Acrylic resin face mask: - Given by Swenson (1959). - Exact guide for reproduction of the vertical dimension. -Shows fullness or lack of fullness of face. . hence gives the third dimension. . plaster face mask : Given by Oslen.
Ridge Relation • Distance of incisive papilla from mandibular incisors Proposed by Mc. Kevitt (1957). incisive papilla – a stabilised landmark.
• Parallelism of the ridges: - Given by Sears. - Paralleling the ridges and 50 opening in the posterior region. - Based on the concept that teeth leave the ridges parallel to each other. - But doesnot always hold good, because teeth are lost at different times…. .
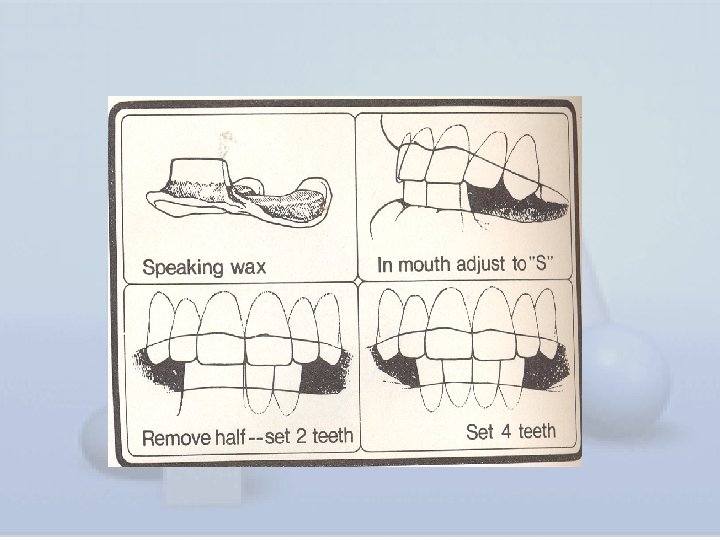
Phonetics – The Speaking Method • Introduced by Meyer Silverman (1956) • Principle : uses the physiologic stimulation of muscle activity during production of speech sounds measure vertical dimension before teeth are lost to be reproduced in complete dentures. • Sibilant ‘s’ is commonly used when mandible is at closest level to maxilla.
• The closest speaking space is the distance between the centric occlusion line and the closest speaking line. • When natural teeth are lost, this space should be reproduced in complete dentures.
Difference Between Freeway Space and Closest Speaking Space. . Silverman Features Closest speaking space Free way space Measured during phonation rest Muscles involved Phonetic action At rest Patient co operation Not required Required Average value 3 to 4 mm 0 to 10 mm
Post Extraction Determination of Closest Speaking Space • Width of occlusal rims is adjusted to provide tongue space. • Asked to say ‘es’ sound. • Note approximate closest speaking space. • Arbitrary 2 mm is decided, depending on appearance. • This relation is rechecked after teeth setting. • Should not be increased beyond normal.
Anterior Teeth Relation While Speaking • By Pound and Murrell (1971). • Incisive guidance is estalished by arranging the anterior teeth in occlusal rims before recording VDO. • Maxillary teeth position is determined by the position of maxilla when patient says ‘f ’, ‘ v ’ and mandibular teeth when he says words with ‘ sound.
Patient’s Neuromuscular Perception • Given by Robert Lytle (1964). • Rationale : An edentulous patient can determine by neuromuscular perception, the occlusal vertical relation position that his mandible should assume when it is in retruded position.
The procedure :
Biting Force • Suggested by Boos (1956) • Theory : patient registers maximum amount of biting force when the teeth first contact in centric occlusion. • This registration is done by means of an instrument called BIMETER.
Swallowing Threshold • Proposed by Thomas Shanahan (1955). • Principle : the constant function of swallowing saliva is the basis for establishing mandibular position and occlusion. During swallowing saliva Mandible rises to habitual closing terminal When saliva is forced back Mandible is retruded to physiologic rest position
The procedure Lower occlusal rim reduced by 3 mm. Soft wax placed on it. Patient asked to bite several times.
Measurement of Old Dentures • Described by Majid Bissasu(2001) • Simple method for determining vertical dimension at occlusion and plane of occlusion. • Can be used only if occlusal plane and vertical dimension are within normal limits.
Interpupillary Distance on Old Photographs in Relation to Interpupillary Distance on Face • Proposed by Wright(1939) • A suitable photograph can be an aid to the establishment of vertical dimension. • According to him, Interpupillary distance on photograph Patient’s Brow-chin Patient’s : interpupillary = distance of : brow-chin distance photograph distance • Now the obtained brow chin distance is equted with the rims plced inside the mouth.
What Happens if Vertical Dimension is Altered? Increased vertical dimension: 1. Discomfort – teeth come into contact sooner than expected. 2. Trauma – caused by constant pressure on the mucous membrane. 3. Clicking of teeth – teeth are raised & the opposing cusps frequently meet each other during speech & mastication. 4. Appearance – over opening may cause elongation of the face & at rest the lips are parted. 5. Loss of freeway space
• Decreased vertical dimension : Inefficiency – the force exerted with the teeth in contact decreases considerably with over closure. Cheek biting – the flabby cheek tend to become trapped between the teeth & bitten during mastication. Appearance – Closer approximation of nose to chin, soft tissue sag & fall in, & the lines on the face are deepened.
• Soreness at the corner of the mouth(Angular cheilitis) – falling in of the corner of the mouth beyond the vermilion border & the deep fold thus formed become bathed in saliva. This area becomes infected & sore. • Pain in TMJ – caused due to strain of the joint & associated ligaments. Associated with pain in the ear, tinnitus & headache.
Evaluating Vertical Dimension • Patient’s tactile sense • Swallowing followed by relaxing • Phonetics
Summary • The vertical dimension of occlusion refers to the length of face as determined by the amount of separation of the jaws. • Many techniques have been used to determine the vertical dimension which range from using pre extraction records to the use of swallowing functionally acquired jaw positions by phonetics and even Cephalometrics. • What so ever there is no universally accepted or completely accurate method to determine the vertical dimension in edentulous patients.
Conclusion • Whatever the method in use, it is the end result that matters. • It should be satisfactory to the dentist and the patient from the esthetic point of view and not induce degenerative changes from a functional standpoint. • So, the vertical dimension must be carefully determined for the success of the prosthesis.
References 1. Boucher’s prosthodontic treatment for edentulous patients 9 th edition 2. Heartwell CM- Textbook of complete dentures 4 th edition 3. Dawson P. E. – Evaluation, diagnosis & treatment of occlusal problems. 2 nd edi. 1989 4. Duncan E. T. & Williams S. T. – Evaluation of rest position as a guide in prosthetic Treatment. JPD 1960; 10, 643 -650. 5. Fayz and Eslami; Determination of occlusal vertical dimension: a literature review JPD 1988; 59: 321 -
6. Garnick J & Ramfjord S. P. – Rest position, An electromyographic & clinical investigation JPD 1962; 12, 895 -911 7. Ismail Y H, George A – The consistency of the swallowing technique in determining the occlusal vertical relation in edentulous patients JPD 1968; 19, 230 -236 8. Silverman Meyer M. – The speaking method in measuring vertical dimension JPD 1953; 3 193 -199 9. Silverman M – Determination of Vertical Dimension by phonetics JPD 1956; 6, 465 -471
10. Swenson M G –Complete Dentures, 4 th edition 11. Swerdlow H. – Vertical dimension literature review JPD 1965; 15, 241 -247 12. J. Landa- free way space and its significance JPD 1952 Vol 2 ; 75613. MM Silverman- vertical dimension must not be increased JPD 1952 Vol 2: 19014. Thomas E J Shanahan-Physiologic vertical dimension and centric relation JPD 1956 vol 6 742 -751
15. Turrell A J –Clinical assessment of vertical dimension JPD 1972; 28: 239 -244 16. Vertical relation of occlusion by the pt’s neuromuscular perception JPD 1964; 14: 12 -21 17. Use of pt’s old denture to determine VD at occlusion JPD 2001; 85: 41318. Winkler- essential of complete denture prosthodontics 2 nd edition 19. Zarb G. A. – Prosthodontic treatment for edentulous patients 12 th edi. 2004
Thank You