Ventricular function recovery on LVAD For idiopathic or






![Circulation. 2008; 118[suppl 1]: S 94–S 105. Hetzer R](https://slidetodoc.com/presentation_image_h/0df4da849c052410b8679d0d8dd44c01/image-7.jpg "Circulation. 2008; 118[suppl 1]: S 94–S 105. Hetzer R")



















 • Every patient should be treated")
- Slides: 34
Ventricular function recovery on LVAD For idiopathic or ischemic CM P. Leprince, CT Surgery Institut of cardiology Pitié-Salpétrière Group Paris, France
Intermacs 1. 4%
Intermacs 0. 8% 0. 9% 0. 4% 1% 16% 0. 3%
Hetzer R
Hetzer R
Hetzer R
Circulation. 2008; 118[suppl 1]: S 94–S 105. Hetzer R
* 30<LVEF<44% at 55<LVEDD<66 mm before VAD removal. Hetzer R
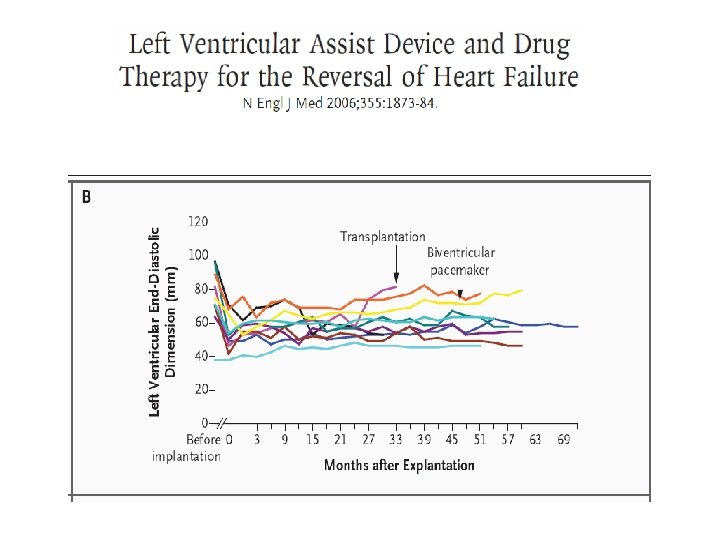
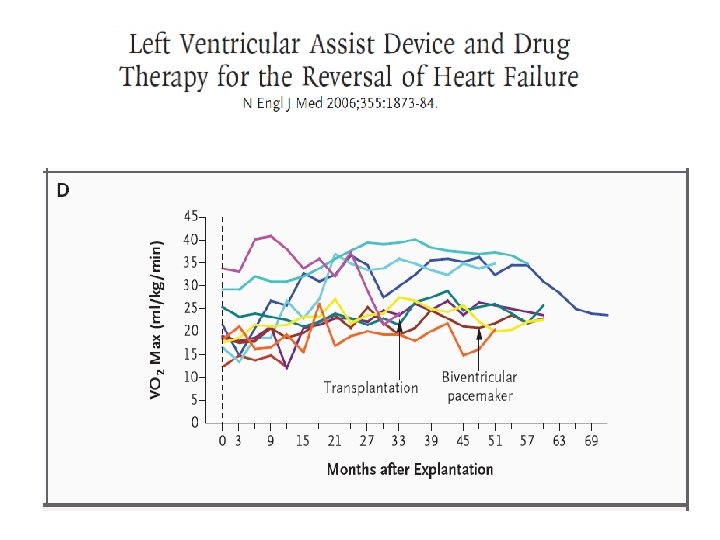
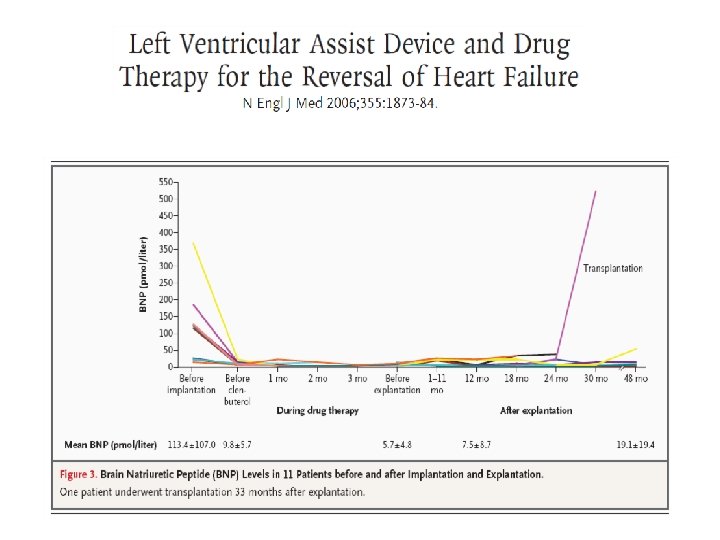
• 15 patients • The patients underwent implantation of left ventricular assist devices and were treated with – – lisinopril, carvedilol, spironolactone, and losartan to enhance reverse remodeling. • Once regression of left ventricular enlargement had been achieved, the β 2 -adrenergic–receptor agonist clenbuterol was administered to prevent myocardial atrophy.
11 patients explanted, 1 death
Conclusions • LVAD removal should be considered as contraindicated if off-pump LVEF does not exceed 40%. • Patients with a history of HF of 5 years should be monitored very carefully after weaning • Neither the LVIDd nor the LVEF measured before LVAD implantation are predictive for potential myocardial improvement during mechanical unloading.
Weaning rate: 8. 8% Multivariate analysis: risk factor for sustained recovery Age: OR 1. 036 Pulsatile: OR 2. 719 (19. 4% vs 2. 46%)
J Heart Lung Transplant 2008; 27: 165– 72 14 BTR, 29 BTT, 29 Tx SF-36: Physical, mental, Global
HMII and Myocardial recovery in ischemic CM P. Leprince, Institut de cardiologie Chirurgie Cardiovasculaire Groupe Hospitalier Pitié-Salpétrière Paris pascal. leprince@psl. aphp. fr
Medical History • • 51 years old female Smoker Regular physical activity March 14 th: – Fast run to get the bus – Pain, Collapsed, spontaneous quick recovery • March 15 th: – Family practitioner: normal exam, normal EKG • March 16 and 17 th: – Dyspnea, fatigue
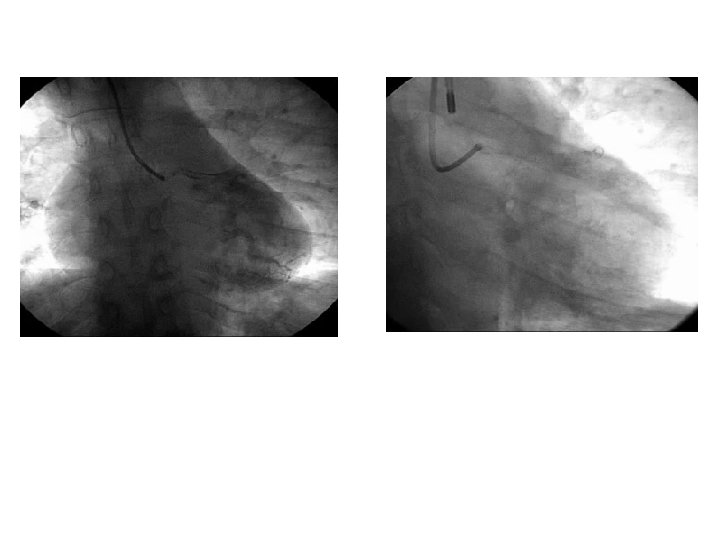
• March 18: – Pain recurrence, collapse Emergency room BP: 95/50 Persisting pain Heart rate : 110 TTE: extented akinesia (anterior and lateral wall, apex, septum). EF: < 25% Dobutamine
After PTCA • • • Dobutamine 10 mic IAPB BP 90 Pic troponin: 42 Stable biologie Clinical signs of poor peripheral perfusion after few hours ECMO
No recovery after 10 days
HMII Implantation instead of high emergency list cardiac transplantation ØTo test for potential recovery ØTo buy time before transplantation
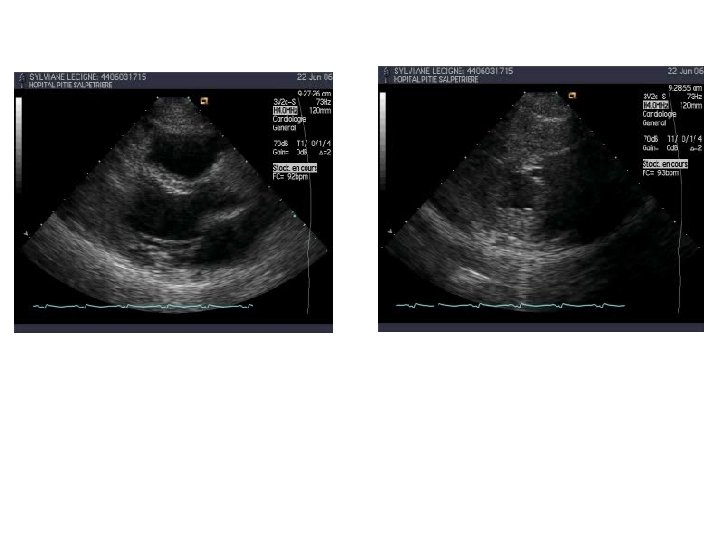
After implantation • Good general status recovery • Discharged directly to home after 20 days • Echocardiography: – Good LV unloading – No aortic valve opening – Myocardial contraction slightly better
Follow up • No complication • Good quality of life • New Echocardiography in June
Vacation time 8000 rpm
Explantation: September
Follow-up
> 5 years • Doing well on ACE inhinbitor and beta bloquers • Normal life • Back to physical activies • Disappearance of apical clot • Isotopic EF: 60%
5 ischemic patients /55 HMII patients • 3 males, 2 females • Age: 39 to 54 • All with – cardiogenic shock related to AMI – ECMO + IABP + inotropes 6 to 10 days – EF at implantation: 7 to 25% – B-, ACE Inhib, Aldactone • Weaning process started at 4 to 14 months • Weaned at 7 to 21 months (EF 25 to 55%) • 1 death related to septic shock
Conclusion • Recovery does exist (5 to 10%) • Every patient should be treated and screened for it • Young age and short duration of heart failure are favorable factors for sustained recovery • Role of pulsatility? • Another advocacy for early implantation